

Abstract
Background:
Aging is associated with a gradual physiological decline, including an imbalance in hormone profile, increased adiposity, and reduced anti-inflammatory cytokines. However, lifelong physical exercise mitigates aging, as observed in endurance-trained middle-aged athletes (EMA).
Aim:
We compared and associated testosterone, interleukin 10 (IL-10), and body fat in EMA and untrained age-matched individuals (UAM).
Methods:
Participants were EMA (n=25; 51.48±9.49 years) and UAM (n=23; 46.0±9.37 years). Both groups underwent body composition measurements (evaluated by a skinfold protocol) and blood sampling for IL-10 (assessed through ELISA® kit) and testosterone (assessed with Roche Diagnostics® kit, Mannheim, Germany, by chemiluminescence technique in a third-party laboratory).
Results:
EMA had lower body fat (14.15±3.82% vs. 23.42±4.95%; P<0.05), higher testosterone (751.68±191.45 ng/dL vs. 493.04±175.15 ng/dL; P<0.05), and higher IL-10 (8.00±1.21 pg/mL vs. 5.89±1.16 pg/mL; P<0.05) compared to UAM. A significant linear correlation was found between testosterone and IL-10 (r=0.56; P=0.001), whereas significant inverse correlations were observed between body fat and testosterone (r=–0.52; P=0.001) and body fat and IL-10 (r=–0.69; P=0.001).
Conclusions:
EMA had higher levels of IL-10 and testosterone and lower body fat in comparison with UAM. In addition, higher IL-10 was associated with increased levels of circulating testosterone and lower body fat.
Relevance for Patients:
The adoption of endurance training as part of a healthy lifestyle may contribute to decreasing age-related testosterone reduction, besides reducing markers of inflammaging, preventing the occurrence of chronic age-related diseases, and thus contributing to healthy aging. For people who already have chronic diseases, physical exercise can shift the immune system toward a more anti-inflammatory profile and, thus, improve their pathological condition. In both cases, physical exercise can help attenuate the decline in testosterone, decrease body fat, and increase anti-inflammatory levels.
Keywords: aging, chronic training, anti-inflammatory markers, body composition
1. Introduction
The aging process is associated with the clinical condition of sarcopenia [1], whose pathophysiology is associated with progressive degeneration of muscle mass and strength, and consequently, a reduction of musculoskeletal function [2]. Sarcopenia is considered one of the major geriatric syndromes that favor the increase in morbidity and mortality of affected individuals [3]. Reduced levels of androgen hormones, especially testosterone, have been frequently observed during aging and have been associated not only with sarcopenia, but also with increased body fat, in parallel with high concentrations of pro-inflammatory cytokines [4,5]. These features may be related to the hypofunction of the hypothalamus-pituitary-gonadal axis and low stimulation of Leydig cells [6,7], probably associated with increased oxidative stress in these cells as we age, which would lead to a decrease in androgen hormone levels, such as testosterone [8]. On the other hand, individuals with a high level of physical fitness, who maintain a balanced diet, lower body fat, and control of stress throughout life, have a lower chronic inflammatory state and higher circulating levels of testosterone [9-11].
Endurance-trained middle-aged athletes (EMA) are individuals over 35 years old, who adhere to consistent and intensive physical training for decades, participating in national and international competitions at a high level. EMA have attenuated aging successfully [12-14] as a result of chronic physiological adaptations, including better body composition [14-16], more favorable oxidative and inflammatory balance [15-17], and maintenance of androgen hormones [4,11,18] compared to untrained age-matched individuals (UAM). In addition, long-term physical exercise also reduces the risk of diseases and disorders, such as metabolic syndrome [19], hypogonadism [20], and neoplasms [21,22].
Testosterone exerts an inhibitory effect on pro-inflammatory cytokines [23], while its low level may be correlated with the expression of inflammatory markers, enhanced by increased body fat [24]. Minuzzi et al. [4] demonstrated that master athletes have an interleukin 10 (IL-10) concentration 27% higher compared to middle-aged controls, and their better body composition was significantly associated with an improved immune response. General physiological function is preserved in chronically trained individuals [25,26] that in turn may be associated with the attenuation of age-related decline in circulating testosterone of master athletes [25]. However, the relationships among testosterone concentration, body composition, and pro-inflammatory cytokines, particularly IL-10, have not been investigated in lifelong trained middle-aged individuals. Therefore, we wanted to compare and associate an anti-inflammatory parameter, IL-10, with testosterone and body fat of EMA and UAM. The hypothesis was that EMA have higher testosterone and IL-10 and lower body fat compared to UAM, with testosterone being positively associated with IL-10 and negatively associated with body fat.
2. Materials and Methods
This study was approved by the Ethics and Research Committee of the Catholic University of Brasilia (protocol: 3,779,535), and it was conducted according to the Helsinki declaration. All volunteers signed an informed consent form, with all procedures explained in a clear and complete manner.
2.1. Participants
A convenience sample of male EMA and UAM was used for the present analysis. These subjects were recruited as part of previous research carried out at the Catholic University of Brasilia. EMA were recruited at national and international athletic competitions and from personal recommendations from other athletes. The inclusion criteria for EMA were: (1) training continuously for at least 15 years; (2) continuing to compete in national and international endurance running events at the time of data collection; (3) not having a diagnosis of recent infection or chronic metabolic diseases; and (4) not taking hormone replacement or any type of pharmaceutical stimulant or depressant of the immune system. The inclusion criteria for UAM were (1) being sedentary; (2) not having a diagnosis of recent infection or chronic metabolic diseases; and (3) not taking hormone replacement or any type of pharmaceutical stimulant or depressant of the immune system.
2.2. General procedures
All volunteers arrived at the laboratory in the morning (between 7:00 am and 8:00 am), on days according to the volunteer’s convenience and availability, with 8-h fasting, and abstaining from physical exercise for at least 24 h before procedures. The blood collections of 2 samples of ~4 mL were drawn and deposited each in Vacutainer tubes with and without EDTA. Those procedures were conducted on the same day of anamnesis and anthropometric measurements. All blood samples were collected from an antecubital vein and centrifuged at 1500 turns for 15 min, to determine IL-10 and total testosterone, and stored in cryogenic vials at −80°C. Serum IL-10 was analyzed in triplicate by ELISA® according to the manufacturer’s instructions (R and D Systems, Minneapolis, MN, USA). The detectable limit for IL-10 was 1.0 pg/mL. The overall inter-assay coefficient of variation for IL-10 was 8%. The total testosterone fraction was analyzed in a third-party reference laboratory, with the Atellica® - Siemens® automatic immunoassay equipment, using the chemiluminescence technique [27]. A Roche commercial kit (Roche Diagnostics®, Mannheim, Germany) was applied to the Modular E170 automated platform, which uses biotinylated anti-testosterone antibody and a testosterone derivative labeled with a ruthenium complex. The separation was performed with microparticles covered with streptavidin, captured by magnetic action and subjected to washing. After this procedure, the reading was performed by applying a voltage that induced the emission of light by the ruthenium complex (electrochemiluminescent test). Standard solutions were prepared for all procedures, one containing only the reagent and a control solution containing the reagent plus a known solution, in duplicate.
Body mass index (BMI) was calculated from weight in kilograms divided by height in meters squared (kg/m2). The relative body fat was estimated using the seven skinfolds protocol proposed by Jackson and Pollock, obtaining the values of the pectoral, axillary, triceps, subscapular, medial thigh, suprailliac, and abdominal folds [28]. A single researcher measured all skinfolds with a Lange® caliper (Cambridge Scientific Instruments, MA, USA). Body density was then calculated following the equation: Body density (g/cm3)=1.112–0.00043499* (sum of 7 skinfolds)+0.00000055* (sum of 7 skinfolds) 2–0.00028826* (Age), and converted into a percentage of body fat, using a formula: Fat%=([4.95/DENS]–4.50)×100 [29].
2.3 Statistical analysis
The normality of the data was verified with the Shapiro-Wilk test. The data were expressed as mean±standard deviation. Independent samples t-tests were conducted to compare each variable between the EMA and UAM groups. In addition, the effect size (Cohen’s d) was calculated [30]. Pearson’s correlation coefficients were calculated to determine the relationships among testosterone, IL-10, and body fat, adjusted for BMI and age together. The level of significance was set at P<0.05. The total sample size in this study conferred statistical power of 86% (post hoc) with a significance level of a=0.05 and a large effect size of d=0.8. All procedures were performed using GraphPad Prism (v. 6.0), Gpower® (v. 3.1), and SPSS 21.
3. Results
The sample consisted of 25 EMA (51.48±9.49 years of age; 21.71±10.19 years of training; 102.08±39 min of daily training; 4.67±1.4 days of weekly aerobic training; and 2.23±1.22 days of weekly strength training) and 23 UAM (46.0±9.37 years). Compared to the EMA, the UAM group had higher body weight (+28.3%; P=0.001), BMI (+22.8%, P=0.001), and height (+2.25%, P=0.047). Age differed slightly between groups (P=0.056). The age range of EMA was 38–71 years (52.21±8.959 years). The age range of UAM was 36–65 years (48.22±8.135 years). The age range of the two groups together was 36-71 years (50.50±8.744 years). The sample characteristics are shown in Table 1.
Table 1. Biometric characteristics of UAM and EMA.
| Variables | UAM | EMA | P-value |
|---|---|---|---|
| Age (years) | 46.0±9.37 | 51.48±9.49 | 0.056 |
| Weight (kg) | 91.1±15.29 | 70.99±7.35 | 0.001 |
| Height (m) | 1.78±0.06 | 1.74±0.06 | 0.047 |
| BMI (kg-m2) | 28.48±4.47 | 23.19±2.09 | 0.001 |
Data expressed as mean and (±) standard deviation. UAM, untrained age-matched individuals; EMA, endurance-trained middle-aged athletes.
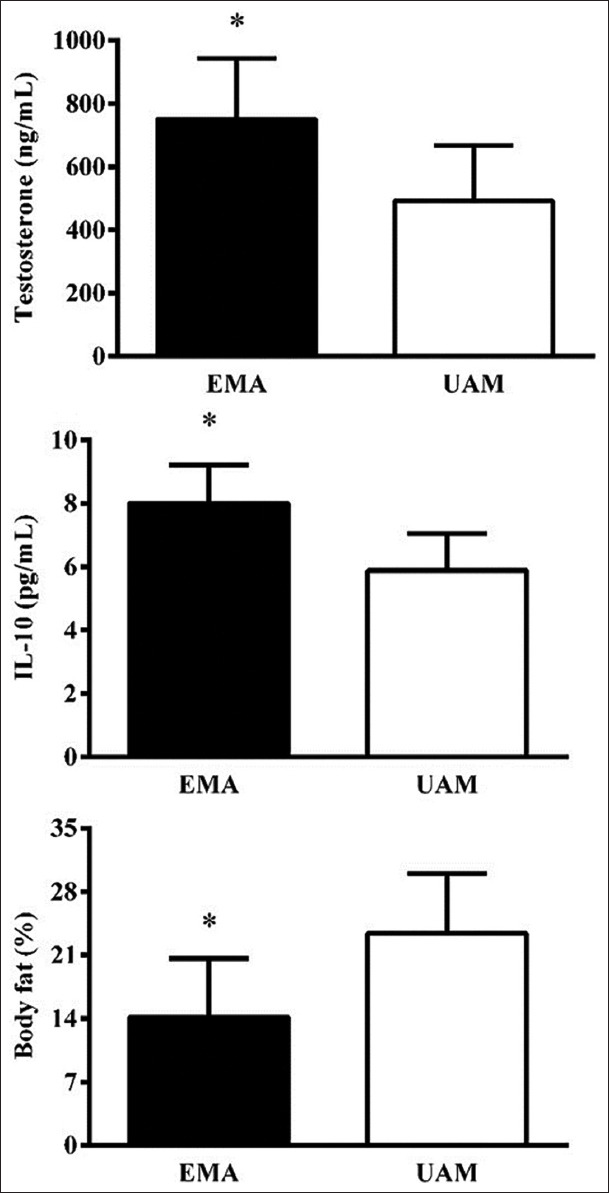
Testosterone was higher (P=0.001) in EMA (751.68±191.45 ng/dL) compared to UAM (493.04±175.15 ng/dL), with a Cohen’s d of 1.41, indicating a very large effect size. IL-10 was higher (P=0.001) for EMA (8.00±1.21 pg/mL) compared to UAM (5.89±1.16 pg/dL), with a very large effect size (d=1.78). Body fat was lower (P=0.001) in EMA (14.15±3.82%) compared to UAM (23.42±4.95%), with a very large effect size (d=2.10); (Figure 1).
Figure 1. Testosterone, IL-10, and body fat of endurance-trained middle-aged and untrained age-matched individuals. IL-10, interleukin 10; * statistical difference; P=0.001.
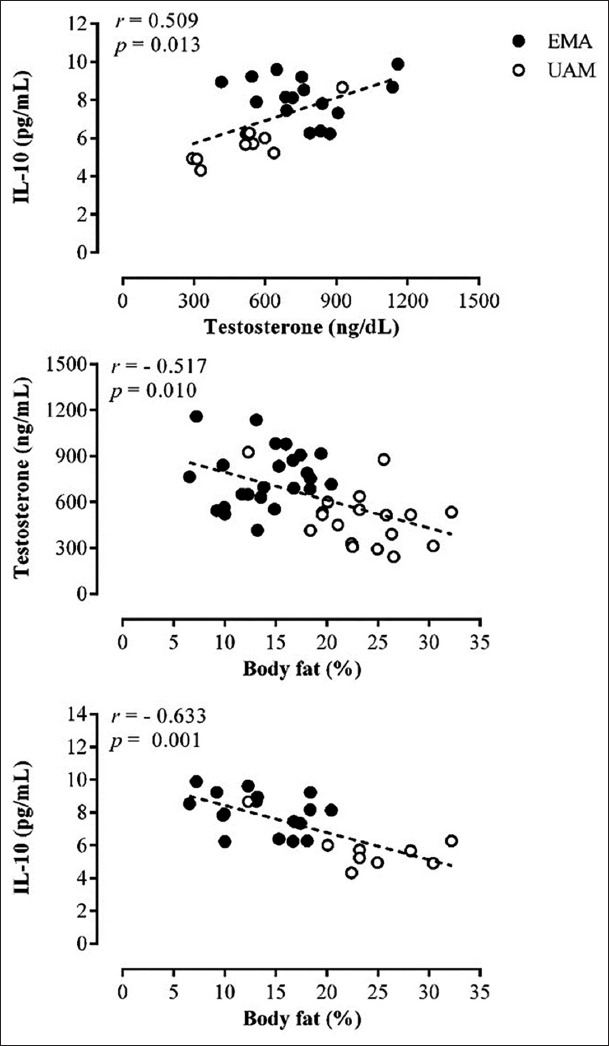
A significant linear correlation was found between testosterone and IL-10 (r=0.56; P=0.001). In addition, body fat was inversely correlated with testosterone (r=–0.52; P=0.001) and IL-10 (r=–0.69; P=0.001); (Figure 2).
Figure 2. Relationship between IL-10 and testosterone (a), testosterone and body fat (b), and IL-10 and body fat (c) of resistance-trained and untrained middle-aged individuals, adjusted for body mass index and age together. IL-10, interleukin 10.
4. Discussion
In the present study, IL-10 and testosterone were compared and correlated in EMA and UAM. EMA were shown to have increased IL-10, whereas it was lower in UAM, possibly suggesting an initial deregulation of inflammatory status for untrained middle aged men [6,31]. In addition, EMA had a higher testosterone concentration compared to UAM. Moreover, a positive correlation between testosterone and IL-10 and a negative correlation between testosterone and body fat demonstrated that EMA are aging healthily [32].
Aging is generally associated with a systemic functional decline in health, due to an accumulation of genetic mutations and cellular damage throughout life [33]. However, exercise and other healthy habits modulate several biomarkers of aging [4,14-17,34], and EMA are a successful model of adequate nutrition, stress management, and consistent training for decades [13]. This lifestyle seems to decrease inflammation [4,17,16,34] and mitigate the decline of testosterone during the usual aging process [35], which is corroborated by the findings of the present study.
Among men, testicular hypofunction occurs over the lifespan due to an increase in reactive oxygen species (ROS) and a decrease in antioxidant defenses, which reduce the sensitivity of luteinizing hormone (LH) receptors and, consequently, decrease the biosynthesis and secretion of testosterone [8]. Further, low testosterone is a predictor of the development of type 2 diabetes, hypertriglyceridemia, hypercholesterolemia, and cardiovascular diseases [36]. Freeman et al. [37] demonstrated that androgen deficiency is a pro-inflammatory modulator, and these cytokines contribute to dysfunctional vascular remodeling from endothelial inflammation. Thus, low testosterone is typically associated with functional decline and a predisposition to chronic diseases mediated by inflammation, mainly cardiovascular diseases, whose morbidity and mortality increase proportionally with age [38].
In addition, we showed that UAM have lower IL-10, an anti-inflammatory marker, and decreased testosterone, while these were elevated in EMA. While testosterone levels were positively associated with IL-10, body fat was negatively associated with both testosterone and IL-10. Besides being the first study to date to demonstrate the relationships among testosterone, IL-10, and body composition in endurance trained middle aged individuals, our findings reinforce that chronic exercise training and the maintenance of low body fat may be pivotal for a healthy anti-inflammatory status and testosterone levels as previously demonstrated [35,39]. Moreover, lifelong exercise training also improves antioxidant defenses [8,17,15,16], and all of the above-mentioned aspects are associated with longevity and healthy aging [13].
According to Bianchi [23], testosterone is immunoregulatory by suppressing the synthesis and proliferation of pro-inflammatory cytokines, such as TNF-alpha, thereby reducing the risk of obesity, atherosclerosis, and metabolic syndrome. Furthermore, Bini [40] demonstrated that an increase in pro-inflammatory cytokines and a decrease in anti-inflammatory cytokines during infectious-inflammatory conditions stimulate excess production of ROS. While exercise may initially protect against pathogens, over time chronic inflammation may lower antioxidant defenses, leading to Leydig cell hypofunction and gonadal resistance to LH stimulation, interfering in steroidogenesis and biosynthesis for the production of testicular testosterone [8]. Thus, higher testosterone in the EMA group may at least partially explain their elevated IL-10, demonstrating positive and continuous feedback between the immune and endocrine systems.
The possible limitations of this study include not measuring nutritional status and dietary intake and not controlling for the use of dietary supplementation among participants. Furthermore, the level of physical fitness of participants was not analyzed because of the short time researchers had with each participant and also because of limitations inherent to international trips for data collection. The initial intent of the study was to form two groups only, athletes and untrained individuals, regardless of their level of physical activity. However, it is important to mention that master athletes have better nutrition and vigorous training routines than non-athletes. In addition, we studied a group of high-level master endurance athletes, which is a very specific and small portion of the population.
5. Conclusions
Endurance trained middle-aged participants had higher testosterone and IL-10 concentrations and lower body fat compared to untrained peers. Testosterone concentrations were associated with a better anti-inflammatory profile and improved body composition. Our athlete sample was comprised of people whose training regimen may result in attenuated inflammaging without chronic disease. Given the global preponderance of chronic diseases, a more widespread adoption of endurance training as part of an overall healthy lifestyle should eventually reduce the occurrence of inflammaging and chronic diseases in the population. Proper physical training may have clinical applications for attenuating testosterone decline, decreasing body fat, and maintaining an adequate anti-inflammatory status, especially in middle age. Longitudinal studies with more subjects and involving master athletes from other sports, such as sprinting, are needed in addition to the current findings to determine how testosterone, IL-10, and body fat are related to functional and health status over time, and the influence of exercise training mode.
Acknowledgments
The authors are thankful to the participants, to FAP-DF for financial support, to CAPES and CNPq for granting scholarships. This study was financed by the Fundação de Apoio à Pesquisa do Distrito Federal (FAP/DF): Demanda espontânea - Edital April 2017, process n° 0193.001762/2017, coordinated by Herbert Gustavo Simões, Ph.D.
Conflict of Interest
The authors declare no conflicts of interest.
References
- [1].Rossetti ML, Steiner JL, Gordon BS. Androgen-Mediated Regulation of Skeletal Muscle Protein Balance. Mol Cell Endocrinol. 2017;447:35–44. doi: 10.1016/j.mce.2017.02.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Yakabe M, Hosoi T, Akishita M, Ogawa S. Updated Concept of Sarcopenia Based on Muscle-bone Relationship. J Bone Miner Metab. 2020;38:7–13. doi: 10.1007/s00774-019-01048-2. [DOI] [PubMed] [Google Scholar]
- [3].Malta DC, Moura L, Prado RR, Oliveira PP, Campos MO. Chronic Non-Communicable Disease Mortality in Brazil and its Regions, 2000-2011. Epidemiol Serv Saúde. 2014;23:599–608. [Google Scholar]
- [4].Minuzzi LG, Chupel MU, Rama L, Rosado F, Munoz VR, Gaspar RC, et al. Lifelong Exercise Practice and Immune Senescence:Master Athletes Cytokine Response to Acute Exercise. Cytokine. 2019;115:1–7. doi: 10.1016/j.cyto.2018.12.006. [DOI] [PubMed] [Google Scholar]
- [5].Nascimento CM, Cardoso JF, de Jesus IT, Orlandi FS, Costa-Guarisco LP, de Oliveira Gomes GA, et al. Are Body Fat and Inflammatory Markers Independently Associated with Age-Related Muscle Changes? Clin Nutr. 2020;2020:30477–5. doi: 10.1016/j.clnu.2020.09.021. [DOI] [PubMed] [Google Scholar]
- [6].López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. The Hallmarks of Aging. Cell. 2013;153:1194–217. doi: 10.1016/j.cell.2013.05.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Wang Y, Chen F, Ye L, Zirkin B, Chen H. Steroidogenesis in Leydig Cells:Effects of Aging and Environmental Factors. Reproduction. 2017;154:R111–22. doi: 10.1530/REP-17-0064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Darbandi M, Darbandi S, Agarwal A, Sengupta P, Durairajanayagam D, Henke R, et al. Reactive Oxygen Species and Male Reproductive Hormones. Reprod Biol Endocrinol. 2018;16:87. doi: 10.1186/s12958-018-0406-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Tang Fui MN, Prendergast LA, Dupuis P, Raval M, Strauss BJ, Zajac JD, et al. Effects of Testosterone Treatment on Body Fat and Lean Mass in Obese Men on a Hypocaloric Diet:A Randomised Controlled Trial. BMC Med. 2016;14:153. doi: 10.1186/s12916-016-0700-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Mohamad NV, Wong SK, Wan Hasan WN, Jolly JJ, Nur-Farhana MF, Ima-Nirwana S, et al. The Relationship between Circulating Testosterone and Inflammatory Cytokines in Men. Aging Male. 2019;22:129–40. doi: 10.1080/13685538.2018.1482487. [DOI] [PubMed] [Google Scholar]
- [11].Barbosa LP, da Silva Aguiar S, Santos PA, Dos Santos Rosa TD, Maciel LA, de Deus LA, et al. Relationship between Inflammatory Biomarkers and Testosterone Levels in Male Master Athletes and Non-Athletes. Exp Gerontol. 2021;151:111407. doi: 10.1016/j.exger.2021.111407. [DOI] [PubMed] [Google Scholar]
- [12].Korhonen MT, Haverinen M, Degens H. Training and Nutritional Needs of the Masters Sprint Athlete. In:Nutrition and Performance in Masters Athletes. Boca Raton, Florida:CRC Press. 2014:291–321. [Google Scholar]
- [13].Kusy K, Zieliński J. Sprinters Versus Long-distance Runners:How to Grow Old Healthy. Exerc Sport Sci Rev. 2015;43:57–64. doi: 10.1249/JES.0000000000000033. [DOI] [PubMed] [Google Scholar]
- [14].Simões HG, Sousa CV, Dos Santos Rosa T, da Silva Aguiar S, Deus LA, Rosa EC, et al. Longer Telomere Length in Elite Master Sprinters:Relationship to Performance and Body Composition. Int J Sports Med. 2017;38:1111–6. doi: 10.1055/s-0043-120345. [DOI] [PubMed] [Google Scholar]
- [15].Aguiar SS, Rosa TS, Sousa CV, Santos PA, Barbosa LP, Deus LA, et al. Influence of Body Fat on Oxidative Stress and Telomere Length of Master Athletes. J Strength Cond Res. 2021;35:1693–9. doi: 10.1519/JSC.0000000000002932. [DOI] [PubMed] [Google Scholar]
- [16].Aguiar SS, Sousa CV, Deus LA, Rosa TS, Sales MM, Neves RV, et al. Oxidative Stress, Inflammatory Cytokines and Body Composition of Master Athletes:The Interplay. Exp Gerontol. 2020;130:110806. doi: 10.1016/j.exger.2019.110806. [DOI] [PubMed] [Google Scholar]
- [17].Sousa CV, Aguiar SS, Santos PA, Barbosa LP, Knechtle B, Nikolaidis PT, et al. Telomere Length and Redox Balance in Master Endurance Runners:The Role of Nitric Oxide. Exp Gerontol. 2019;117:113–8. doi: 10.1016/j.exger.2018.11.018. [DOI] [PubMed] [Google Scholar]
- [18].Mikkelsen UR, Couppé C, Karlsen A, Grosset JF, Schjerling P, Mackey AL, et al. Life-long Endurance Exercise in Humans:Circulating Levels of Inflammatory Markers and Leg Muscle Size. Mech Ageing Dev. 2013;134:531–40. doi: 10.1016/j.mad.2013.11.004. [DOI] [PubMed] [Google Scholar]
- [19].Tuttor M, von Stengel S, Kohl M, Lell M, Scharf M, Uder M, et al. High Intensity Resistance Exercise Training vs High Intensity (Endurance) Interval Training to Fight Cardiometabolic Risk Factors in Overweight Men 30-50 Years Old. Front Sports Act Living. 2020;2:68. doi: 10.3389/fspor.2020.00068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Mintziori G, Nigdelis MP, Mathew H, Mousiolis A, Goulis DG, Mantzoros CS. The Effect of Excess Body fat on Female and Male Reproduction. Metabolism. 2020;107:154193. doi: 10.1016/j.metabol.2020.154193. [DOI] [PubMed] [Google Scholar]
- [21].Ortega MA, Fraile-Martínez O, García-Montero C, Pekarek L, Guijarro LG, Castellanos AJ, et al. Physical Activity as an Imperative Support in Breast Cancer Management. Cancers (Basel) 2020;13:55. doi: 10.3390/cancers13010055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Rosa-Neto JC, Silveira LS. Endurance Exercise Mitigates Immunometabolic Adipose Tissue Disturbances in Cancer and Obesity. Int J Mol Sci. 2020;21:9745. doi: 10.3390/ijms21249745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Bianchi VE. The Anti-Inflammatory Effects of Testosterone. J Endocr Soc. 2018;3:91–107. doi: 10.1210/js.2018-00186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].de Heredia FP, Gómez-Martínez S, Marcos A. Obesity, Inflammation and the Immune System. Proc Nutr Soc. 2012;71:332–8. doi: 10.1017/S0029665112000092. [DOI] [PubMed] [Google Scholar]
- [25].Hayes LD, Grace FM, Sculthorpe N, Herbert P, Kilduff LP, Baker JS. Does Chronic Exercise Attenuate Age-related Physiological Decline in Males? Res Sports Med. 2013;21:343–54. doi: 10.1080/15438627.2013.825799. [DOI] [PubMed] [Google Scholar]
- [26].Minuzzi LG, Rama L, Chupel MU, Rosado F, Kuga GK, Gaspar RC, et al. Immune-Endocrine Responses and Physical Performance of Master Athletes during the Sports Season. J Cell Biochem. 2019;120:5551–7. doi: 10.1002/jcb.27839. [DOI] [PubMed] [Google Scholar]
- [27].Fasano T, Bedini JL, Fle PA, Jlaiel M, Hubbert K, Datta H, et al. Multi-site Performance Evaluation and Sigma Metrics of 20 Assays on the Atellica Chemistry and Immunoassay Analyzers. Clin Chem Lab Med. 2019;58:59–68. doi: 10.1515/cclm-2019-0699. [DOI] [PubMed] [Google Scholar]
- [28].Jackson AS, Pollock ML. Generalized Equations for Predicting Body Density of men. Br J Nutr. 1978;40:497–504. doi: 10.1079/bjn19780152. [DOI] [PubMed] [Google Scholar]
- [29].Siri WE. Body Composition from Fluid Spaces and Density:Analysis of Methods 1961. Nutrition. 1993;9:480–92. [PubMed] [Google Scholar]
- [30].Cohen J. Statistical Power Analysis for the Behavioral Sciences. Cambridge, Massachusetts:Academic Press. 2013 [Google Scholar]
- [31].Blaya R, Blaya P, Rhoden L, Rhoden EL. Low Testosterone Levels and Metabolic Syndrome in Aging Male. Curr Pharm Des. 2017;23:4470–4. doi: 10.2174/1381612823666170503150955. [DOI] [PubMed] [Google Scholar]
- [32].Geard D, Reaburn PR, Rebar AL, Dionigi RA. Masters Athletes:Exemplars of Successful Aging? J Aging Phys Act. 2017;25:490–500. doi: 10.1123/japa.2016-0050. [DOI] [PubMed] [Google Scholar]
- [33].Beyret E, Redondo PM, Luengo AP, Belmonte JC. Elixir of Life:Thwarting Aging with Regenerative Reprogramming. Circ Res. 2018;122:128–41. doi: 10.1161/CIRCRESAHA.117.311866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Rosa TS, Neves RV, Deus LA, Sousa CV, da Silva Aguiar S, de Souza MK, et al. Sprint and Endurance Training in Relation to Redox Balance, Inflammatory Status and Biomarkers of Aging in Master Athletes. Nitric Oxide. 2020;102:42–51. doi: 10.1016/j.niox.2020.05.004. [DOI] [PubMed] [Google Scholar]
- [35].Ari Z, Kutlu N, Uyanik BS, Taneli F, Buyukyazi G, Tavli T. Serum Testosterone, Growth Hormone, and Insulin-like Growth Factor-1 Levels, Mental Reaction Time, and Maximal Aerobic Exercise in Sedentary and Long-Term Physically Trained Elderly Males. Int J Neurosci. 2004;114:623–37. doi: 10.1080/00207450490430499. [DOI] [PubMed] [Google Scholar]
- [36].Brand JS, Rovers MM, Yeap BB, Schneider HJ, Tuomainen TP, Haring R, et al. Testosterone, Sex Hormone-binding Globulin and the Metabolic Syndrome in Men:An Individual Participant Data Meta-Analysis of Observational Studies. PLoS One. 2014;9:e100409. doi: 10.1371/journal.pone.0100409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Freeman BM, Mountain DJ, Brock TC, Chapman JR, Kirkpatrick SS, Freeman MB, et al. Low Testosterone Elevates Interleukin Family Cytokines in a Rodent Model:A Possible Mechanism for the Potentiation of Vascular Disease in Androgen-deficient Males. J Surg Res. 2014;190:319–27. doi: 10.1016/j.jss.2014.03.017. [DOI] [PubMed] [Google Scholar]
- [38].Brant LC, Nascimento BR, Passos VM, Duncan BB, Bensenõr IJ, Malta DC, et al. Variations and Particularities in Cardiovascular Disease Mortality in Brazil and Brazilian States in 1990 and 2015:Estimates from the Global Burden of Disease. Variações e Diferenciais da Mortalidade por Doença Cardiovascular no Brasil e em Seus Estados, em 1990 e 2015:Estimativas do Estudo Carga Global de Doença. Rev Bras Epidemiol. 2017;20:116–28. doi: 10.1590/1980-5497201700050010. [DOI] [PubMed] [Google Scholar]
- [39].Petersen AM, Pedersen BK. The Anti-inflammatory Effect of Exercise. J Appl Physiol (1985) 2005;98:1154–62. doi: 10.1152/japplphysiol.00164.2004. [DOI] [PubMed] [Google Scholar]
- [40].Bini EI, D'Attilio L, Marquina-Castillo B, Mata-Espinosa D, Díaz A, Marquez-Velasco R, et al. The Implication of Pro-inflammatory Cytokines in the Impaired Production of Gonadal Androgens by Patients with Pulmonary Tuberculosis. Tuberculosis (Edinb) 2015;95:701–6. doi: 10.1016/j.tube.2015.06.002. [DOI] [PubMed] [Google Scholar]