

Abstract
Pandemics are associated with high rates of morbidity and mortality, and the coronavirus disease (COVID-19) pandemic has been the most fatal coronavirus outbreak of the 21st century. To reduce person-to-person transmission, interventions such as social distancing have been recommended; however, it is anticipated that 80% compliance is required to control the outbreak. A questionnaire was used to assess the factors related to compliance with social distancing restrictions using a modified version of the Theory of Planned Behavior (TPB) that included participants’ understanding of restrictions. The questionnaire included 18 vignettes (violating, non-violating and ambiguous) to assess participants’ knowledge of the social distancing restrictions and intentions to violate them. Participants were also presented the social distancing restrictions relevant at the time of completion and they were asked to consider the restrictions when anticipating their behavior in the vignettes. In line with the predictions of the TPB, intentions to adhere to restrictions and perceived behavioral control predicted participants’ self-reported behaviors. Further, attitudes (ATT) toward social distancing restrictions and knowledge of the restrictions predicted intentions to adhere to them. Public health messaging should aim to increase the understanding of the restrictions, e.g. through the use of example scenarios of permitted and prohibited behaviors. This would be particularly beneficial when changes are implemented to promote the understanding of the restrictions and positive ATT toward them.
Pandemics pose a global threat to human health, and the coronavirus disease (COVID-19) pandemic has caused the highest mortality rate of any coronavirus outbreaks in the 21st century [1]. In the absence of pharmaceutical interventions, strategies such as social distancing are commonly employed during pandemics to reduce person-to-person transmission [2]. Social distancing refers to behaviors or policies that are promoted or mandated by government authorities with the objective of reducing contact rates between individuals in the general population [3]. Examples from previous pandemics include the isolation of confirmed or suspected cases, bans placed on mass gatherings and school closures [3]. However, the effectiveness of social distancing depends upon individuals’ adherence to these rules [4]. Therefore, it is important to identify the factors that promote compliance with social distancing.
Prior research has shown that there are individual differences in adherence to health recommendations. In addition to demographic variables, social cognitive factors have been found to explain individual differences, and these are more easily modified than demographic factors [5]. Therefore, social cognition models are often used to explain the variations in the adoption of health recommendations [6] and identify the factors that can be targeted to improve compliance.
The Theory of Planned Behavior (TPB) has been one of the most widely tested social cognition frameworks examining health-related behaviors [7]. It has been shown through meta-analyses to account for 27% of variance in behaviors and 39% of variance in intentions [8], with perceived behavioral control (PBC) accounting for a significant portion of variance. Given the potential challenges associated with social distancing compared with other health behaviors (e.g. handwashing), this framework was selected to examine adherence to social distancing restrictions.
The TPB [9] posits that intentions are the most proximal predictor of behavior, and intentions mediate the effect of ATT, subjective norms (SN) and PBC on behavior. According to the TPB, it would be expected that more favorable ATT toward social distancing, stronger SN endorsing social distancing, and greater perceived ability to adhere to restrictions would predict greater intentions to adhere to social distancing. Additionally, intentions to comply with restrictions and increased behavioral control should predict more compliant social distancing behavior.
ATT
ATT are defined as an individual’s favorable or unfavorable evaluations of the social distancing requirements and the importance of social distancing for limiting the transmission of COVID-19. In the case of social distancing, people with favorable ATT toward restrictions might believe that contracting COVID-19 would have adverse health effects and that social distancing is likely to be effective in preventing transmission. ATT toward health recommendations have previously been found to predict adherence to them, as individuals who believe that health behaviors control the spread of infectious disease are more likely to adhere to them [10]. Conversely, individuals perceiving public health messaging as dishonest and disproportionate are less likely to comply [11], and distrust in the government has been cited as a reason for non-adherence [12]. In one study, individuals who agreed with their government’s isolation requirements during a pandemic reported greater intentions to adhere to them [13]. Holding these beliefs is likely to influence the ATT held toward the recommendations to socially distance and the restrictions imposed to reduce transmission. However, in past studies, these intentions to adhere were examined through direct questioning (e.g. if you were instructed to self-isolate, do you think you could do it? [13]) whereby the desired response might be apparent and lead participants to respond favorably given the consequences of non-adherence. Participants were also not asked in the context of specific scenarios, and therefore, it is unclear whether respondents understood the restrictions and if they accounted for circumstantial factors when responding.
SN
SN, which refer to the perceived social pressure to adhere to social distancing restrictions, are also likely to be important in predicting compliance during a pandemic. People with high SN might perceive that others who are important to them would support them in adhering to social distancing restrictions. Prior research has found that people are more likely to wear a face mask when they observe other people doing so and when they perceive that their friends and family consider them to be effective in reducing transmission [14]. Conversely, adherence to quarantine orders is reduced when individuals believe that others consider it unimportant and when they observe other people violating orders [15].
PBC
The third factor posited to influence intentions during a pandemic is PBC, which is the perceived ease or difficulty of performing a behavior [9]. People with a high PBC perceive less barriers to complying, and they perceive that the barriers are more easily overcome than people with a low PBC. In addition to influencing intentions, PBC is also believed to influence behavior directly [9]. Compliance with social distancing has been found to be lower when individuals are unable to work from home and when adhering to restrictions would negatively impact their income [16]. People also report that difficulty accessing groceries and medical supplies is a barrier to adhering to social distancing requirements [15] and might inhibit compliance with restrictions. These perceived barriers to adhering to social distancing provide support for the PBC construct for predicting compliance with social distancing requirements.
Unlike recommendations such as wearing a mask or practicing regular handwashing, adhering to social distancing restrictions is contingent on people understanding the restrictions, and this is likely to influence the perceived difficulty of complying. That is, it may be difficult to comply when restrictions are viewed as confusing or unclear. Adhering to social distancing restrictions likely depends on understanding the restrictions, and this has been much less examined than ATT, SN, and PBC. Given the increased complexity associated with understanding social distancing than other health behaviors (such as mask wearing or handwashing) and that many people are less familiar with the concept of social distancing, it is an important factor to examine.
Understanding of COVID-19 restrictions
With social distancing restrictions rapidly evolving, another factor thought to influence intentions to comply is understanding of social distancing restrictions. Understanding refers to the ability to accurately identify behaviors that are allowed and prohibited by the restrictions. This is important as people are unlikely to make accurate evaluations of ATT, SN and PBC if they possess poor knowledge and understanding of the restrictions. This is particularly important as the social distancing restrictions have been frequently changed during the COVID-19 outbreak in Australia.
It seems likely that to hold positive ATT toward social distancing restrictions, a level of understanding of the restrictions is required. Similarly, it is likely that poor understanding of the restrictions would pose a barrier to complying with them, influencing individuals’ PBC, given they have a level of insight into their understanding. Prior research has found that increased awareness of COVID-19, including symptoms and transmission, is associated with greater performance protective health behaviors including social distancing [17, 18]. Similar results have been found in studies assessing knowledge of COVID-19, including knowledge of the protocols if individuals exhibit COVID-19 symptoms [18]. These authors [18] found higher knowledge was associated with higher SN, PBC and intentions to follow recommendations including handwashing and wearing a mask. While greater understanding of COVID-19 is associated with more positive ATT and adoption of preventative behaviors, understanding of specific social distancing restrictions has seldom been examined.
Although useful, existing research into adherence to health recommendations during a pandemic has limitations. As COVID-19 is the most widespread pandemic of the 21st century, many people were not familiar with the term ‘social distancing’ or the strategies it referred to before the outbreak of COVID-19. In addition, the concept of social distancing is more multi-faceted than practices such as handwashing and mask wearing, and it is possible that understanding of the requirements of social distancing varies more than the understanding of practices used to prevent the transmission of infectious diseases previously. Although prior research has examined practices such as handwashing and mask wearing [14], the requirements of engaging in these behaviors are less likely to be misunderstood than the requirements to adhere to social distancing recommendations.
In addition, past research has typically replied on self-report measures whereby participants are asked to indicate the extent to which they intend to adhere to social distancing restrictions [e.g. 19]. This assumes that participants understand the social distancing restrictions and what activities are permitted and not permitted. Consequently, individuals may intend to adhere to restrictions, when indeed their intended behavior would violate the restrictions.
The current study
This study utilized an online questionnaire featuring 18 vignettes to measure intentions to comply with social distancing restrictions. In addition, factors of a modified version of the TPB, including ATT, understanding of restrictions, SN, PBC, intentions and behavior were examined. The questionnaire included the social distancing restrictions imposed by the Australian Government on 13 May 2020 and applicable for all participants at the time of completion. Vignettes, including 13 violating vignettes, three non-violating vignettes and two ambiguous vignettes, assessed participants’ understanding of the restrictions and intentions to violate them. Understanding was assessed as the number of violations and non-violations of the restrictions correctly identified.
Vignette studies have increased utility compared with direct questions as they standardize conditions to all respondents to control for individual differences or differences in interpretation [19]. The use of vignettes in this study also aims to assess understanding of social distancing restrictions, as participants were asked whether they believe that the protagonists violated the restrictions presented. This allows for participants’ understanding of the restrictions to be examined as a predictor of their intentions to comply with them.
In line with previous research into social distancing and other preventative practices against pandemic diseases, it is hypothesized that intentions to violate social distancing restrictions will be predicted by poorer understanding of restrictions (H1), more negative ATT toward restrictions (H2), lower reported adherence among family and friends (H3) and a lower reported ability to adhere to restrictions (H4). It is further hypothesized that reported violations of social distancing restrictions will be predicted by a lower reported ability to adhere to restrictions (H5) and higher intentions to violate them (H6; see Fig. 1).
Fig. 1.
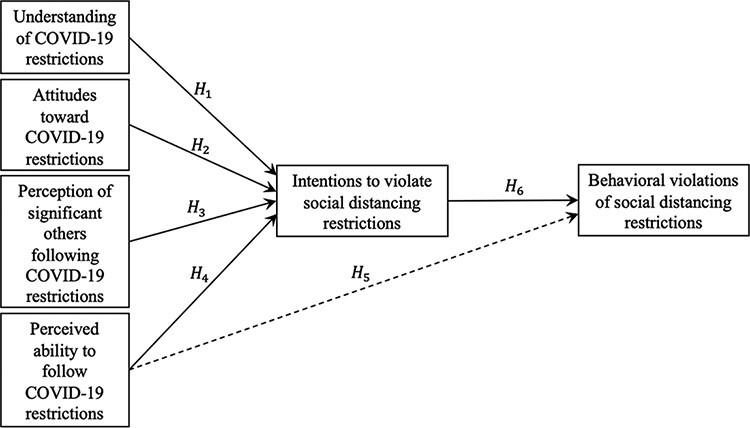
Hypotheses of the current study.
Method
Participants
A total of 110 Australian residents (87 females) participated in the study between 16 May 2020 and 30 May 2020. Participants were invited to partake in the study via the University’s Research Participation System and through the distribution of the survey among the authors’ professional networks by email and networking forum posts, with a potential sample of approximately 700 individuals. Many of the participants were recruited from allied health and education disciplines. The response rate was approximately 15%.
Participants were residents from South Australia (63.6%), New South Wales (26.4%), Western Australia (3.6%), Queensland (2.7%), Victoria (2.7%) and the Australian Capital Territory (0.9%). Participants ranged in age from 18 to 63 years (M = 32.5, SD = 12.7). At the time of data collection, social distancing restrictions were consistent across all Australian states and territories. Therefore, there were no variations in restrictions according to participants’ state of residence.
Procedure
The study received approval from the University of Adelaide’s Human Research Ethics Committee (reference 20/50). Participation was voluntary and anonymous, and participants could withdraw at any time. Data were collected between 16 May and 30 May 2020. Data collection was ceased on 30 May 2020 as social distancing restrictions were eased from 1 June 2020 in some Australian states. This provided greater consistency of the restrictions applicable to participants and ensured that behaviors reported by participants were actually prohibited at the time they were performed.
Participants completed all scales via a single online survey. Across all three recruitment methods, participants were presented with a recruitment script outlining the purpose of the study and a link to the survey on Qualtrics. Upon accessing the link, participants were presented with a consent form, which they were required to complete before proceeding to the survey questions. After completing the demographic questions, participants completed the SN scale, PBC scale, ATT scale, the vignettes assessing understanding and intention and finally the behavioral questions. Behavioral questions were presented last to minimize the potential influence of participants’ past behavior on their responses to the earlier questions.
Materials
Social distancing vignettes
Social distancing vignettes consisted of 18 short scenarios. Thirteen vignettes described violations of the social distancing restrictions (e.g. exercising in groups larger than two), three described situations in which the protagonist was not violating the restrictions (e.g. collecting a grocery order from a Service Desk) and two described ambiguous scenarios (e.g. making a cash payment).
Before participants viewed and responded to the vignettes, they were presented with a list of the Australian government restrictions for social distancing from 13 May 2020. All participants completed the study while these restrictions were in place and they were asked to respond assuming the restrictions were current. When responding to the vignettes, participants were unable to return to the previous screen with the restrictions. This was intended to control for individual differences in prior exposure to the restrictions, e.g. by accessing them online prior to participating. It is possible that participants’ existing knowledge of restrictions prior to survey completion varied according to whether they had accessed the list of restrictions previously and the source of information relied upon.
The restrictions, provided by the Australian Government, were presented under the headings, ‘In public’, ‘Households’, ‘At work’ and ‘In schools’, with each section containing between 8 and 13 bullet points. The restrictions used simple language; however, each section included up to 20 lines of text. Of the 13 violating and 3 non-violating vignettes, all behaviors were referred to in the restrictions as either permitted or prohibited.
In response to each vignette, participants were asked to indicate whether they believed the protagonist violated the social distancing restrictions on a scale from 1 (‘Strongly Disagree’) to 6 (‘Strongly Agree’). Responses were combined such that scores between 1 and 3 were considered correct for vignettes where no violation had occurred, and scores between 4 and 6 were considered correct for vignettes where the restrictions had been violated. An understanding score was calculated by summing participants’ total number of correct identifications for violating and non-violating vignettes, with higher scores indicating greater understanding of COVID-19 restrictions.
Intentions to violate social distancing restrictions were assessed by asking participants to rate on a scale from 1 (‘Strongly Disagree’) to 6 (‘Strongly Agree’) whether they would perform the behavior in each vignette if they were in the protagonist’s position. Scores from the violating vignettes only were summed to create an intentions score, where higher scores represented greater intentions to violate social distancing restrictions.
ATT scale
ATT toward social distancing restrictions were examined using eight items assessing participants’ agreeance with the restrictions imposed by the Australian government. The first four items asked participants to rate their evaluations of the restrictions as necessary, important for their health, important for the health of their family members and important for the health of others. Four additional items from Georgiou, Delfabbro and Balzan’s [20] government response scale were also used (e.g. ‘During the COVID-19 pandemic, the Australian Government’s response has been the correct course of action’). All items used a scale from 1 (‘Strongly Disagree’) to 5 (‘Strongly Agree’). Participants’ ratings of the government’s response as too strict were reverse coded and the eight items were summed. Higher scores indicated more favorable ATT. A Cronbach’s alpha of 0.75 indicates adequate internal consistency.
SN scale
SN were assessed using two items. Participants rated the extent to which they agreed their friends and family were adhering to the social distancing restrictions and to what extent they perceived pressure to attend an event that violated the social distancing restrictions (reverse coded). Participants rated their agreement on a scale of 1 (‘Strongly Disagree’) to 5 (‘Strongly Agree’) and the responses were summed. Higher scores indicated stronger perceived social endorsement to adhere to the restrictions. Scores from the two items were significantly and negatively correlated (r = −0.240).
PBC scale
PBC was assessed using the item, ‘I feel that I have the ability to follow the current social distancing restrictions’. Participants rated their agreement on a scale from 1 (‘Strongly Disagree’) to 5 (‘Strongly Agree’), with higher scores indicating greater perceived ability to adhere.
Behavior scale
Behavior was assessed using five items that asked participants to indicate the frequency at which they performed behaviors during the previous month that were prohibited by the social distancing restrictions. These included leaving their household for a non-permitted purpose, attending an event or gathering with more than 10 people present, performing physical greetings (e.g. hugging or kissing) with someone from outside of their household, exercising with more than one person from outside their household, and making a cash payment. Participants provided a numerical value for the number of times they estimated performing the behaviors during the month prior to survey completion, and the five responses were summed to produce an overall behavior score whereby higher scores indicated more frequent violations of social distancing restrictions. There was a wide range of scores (min = 0, max = 70) due to a positive skew in behavior scores. During statistical analyses, residuals were closely examined to ensure that the assumption of normality was not violated.
Results
Preliminary statistical analyses consisted of Pearson correlation coefficients to identify significant relationships between variables. A path analysis was then conducted (see Fig. 1) to determine the strength and direction of relationships between the main variables of interest controlling for other predictors in the model. Parameter estimates from the path analysis are summarized in Fig. 2.
Fig. 2.
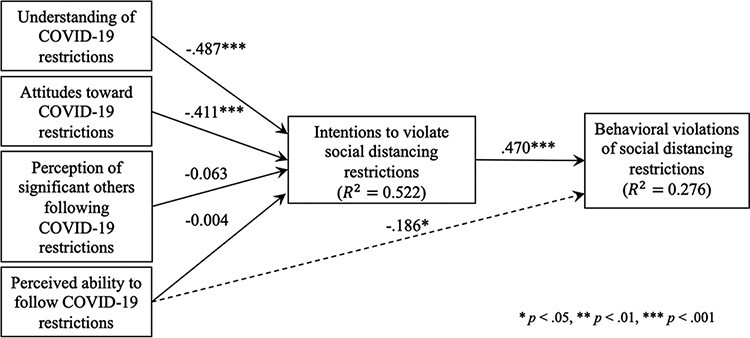
Path model of the current study.
Descriptive statistics are presented in Table I. The mean behavior score was 8.17 ± 12.30 and intentions were 39.41 ± 10.94 (from a possible 78 whereby higher scores indicated greater intentions to violate restrictions). The mean ATT score was 34.93 ± 4.71 (of a possible 40, whereby higher scores indicated more favorable ATT) and the mean SN score was 9.70 ± 1.46 (of a possible 10, whereby higher scores indicated stronger endorsement to adhere to restrictions). The mean PBC score was 4.69 ± 0.60 (of a possible five, with higher scores representing stronger ability to adhere). Additionally, participants correctly identified 10.48 behaviors (±2.68, from 16 vignettes). Therefore, participants correctly identified violations and non-violations of the social distancing restrictions at a rate of 65.5%. Understanding was higher for non-violating vignettes (M = 75.67 ± 30.50) than violating vignettes (M = 71.23 ± 15.48), indicating that participants were marginally more likely to categorize a violating behavior as being permitted than a non-violating behavior as breaking the restrictions.
Table I.
Means, standard deviations and correlation coefficients
| M | SD | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|---|
| 1 Behavior | 8.17 | 12.30 | – | – | – | – | – | – |
| 2 Intentions | 39.41 | 10.94 | 0.49** | – | – | – | – | – |
| 3 Understanding | 10.48 | 2.68 | −0.22* | −0.59** | – | – | – | – |
| 4 ATT | 34.93 | 4.71 | −0.29** | −0.55** | 0.23* | – | – | – |
| 5 SN | 9.70 | 1.46 | −0.27** | −0.22* | 0.04 | 0.00 | – | – |
| 6 PBC | 4.69 | 0.60 | −0.24* | −0.12 | 0.04 | 0.18 | 0.38** | – |
P < 0.05
P < 0.01.
Behavioral violations of social distancing correlated positively with intentions to violate restrictions (r = 0.49, p < 0.001) and negatively with PBC (r = −0.24, p = 0.014). Intentions to violate restrictions also correlated negatively with understanding of social distancing restrictions (r = −0.59, p < 0.001), ATT (r = −0.55, p < 0.001) and SN (r = −0.22, p = 0.024). Path analyses were used to identify significant paths within the model (see Table II and Fig. 2). Assumption testing revealed that, for each model, all endogenous variables were continuous and had normally distributed residuals, there were no missing data or outliers and there was a theoretical basis for model specification. Model fit statistics revealed a good model fit, χ2(3) = 2.45, P = 0.484, RMSEA (0.001), TLI (1.00), CFI (1.00).
Table II.
Parameter estimates
| Relationship | Unstandardized paths | Standard error | P |
|---|---|---|---|
| Intention ➔ Behavior | 5.45 | 0.10 | <0.001 |
| PBC ➔ Behavior | −2.28 | 1.66 | 0.023 |
| Understanding ➔ Intention | −7.35 | 0.27 | <0.001 |
| ATT ➔ Intention | −6.20 | 0.15 | <0.001 |
| SN ➔ Intention | −0.94 | 0.50 | 0.345 |
| PBC ➔ Intention | −0.07 | 1.20 | 0.947 |
Lower intentions to violate restrictions were predicted by a higher understanding of social distancing restrictions (β = −7.35, P < 0.001) and more positive ATT toward them (β = −6.20, P < 0.001), supporting H1 and H2. Perceived endorsement for social distancing (β = −0.94, P = 0.345) and perceived ability to follow social distancing restrictions (β= −0.07, P = 0.947) did not predict intentions to violate restrictions, and H3 and H4 were not supported. Stronger intentions to violate social distancing restrictions (β= 5.45, P < 0.001) and lower perceived ability to follow restrictions (β = −2.28, P = 0.023) predicted higher behavioral violations during the previous month, providing support for H5 and H6. The model explained 52.2% of variance in intentions and 27.5% in behavior.
Discussion
The aim of this study was to evaluate whether ATT, SN, PBC and understanding of social distancing restrictions predict intentions to comply with social distancing in an Australian sample. As hypothesized, a higher understanding of social distancing restrictions and more favorable ATT toward restrictions predicted lower intentions to violate the restrictions. However, SN and PBC did not predict intentions to violate restrictions. That positive ATT predicted lower intentions to violate restrictions is congruent with prior research [13]. Unlike the current study, the authors [13] also found that SN and PBC predicted intentions, although these were weaker predictors than ATT.
This study also evaluated the predictors of self-reported behavioral violations of social distancing restrictions. Greater intentions to violate the restrictions and lower perceived ability to adhere to restrictions predicted higher social distancing violations, as hypothesized. This finding supports those of previous studies [18]. These authors demonstrated that stronger intentions to follow restrictions and higher levels of control led to greater adherence to social distancing, as well as handwashing, using a hand sanitizer, working from home and using face masks.
Within this study, SN and PBC did not affect intentions to adhere to social distancing restrictions. SN have previously been found to be a weak predictor of intentions to perform a range of health behaviors [21]. More recently, however, SN have been found to be important in predicting compliance with social distancing [13]. Like the previous study [13], SN had a greater association with intentions than PBC in this study; however, they did not achieve significance. A possible reason for this is the use of items assessing SN. Specifically, the prior study [13] asked participants if they would advise their neighbors or colleagues if they were infected with a pandemic disease, and to what extent they would trust the infectious disease prevention information from the health department. As the study was not conducted during an infectious disease outbreak, participants considered a hypothetical pandemic rather than reflecting on others’ opinions or behaviors during an actual pandemic. Because of this, they were also unable to consider the consequences of disclosing their infected status to neighbors or colleagues due to the unknown disease. Without the lived experience of a pandemic, it is likely that participants were unable to accurately anticipate their and others’ behavior.
An additional difference in this study compared with the aforementioned study [13] is the influence of PBC on intentions. PBC significantly predicted intentions to adhere to isolation requirements in the prior study, although this was not replicated in this study. Although PBC was not associated with intentions, it significantly predicted self-reported behavior during the previous month. It is possible that participants did not consider their level of control over their behavior when responding to the vignettes as these were presented as actions performed by another person. However, PBC is likely to have influenced participants’ actual behavior during the month prior, resulting in the direct effect of perceived control on reported behavior. Other considerations include that participants did not consider the full extent of barriers to complying with social distancing restrictions when indicating control, given the single item measuring PBC. Using additional items addressing specific barriers may elicit different results in the future. It is also possible, given that PBC was assessed before participants viewed the list of restrictions and behavior was assessed as actions performed before participating in the study, participants may have acquired an improved understanding of the restrictions before responding to the vignettes which they did not possess when contemplating their behavior before survey completion. This would provide further support for the notion that understanding of social distancing restrictions is important for promoting compliance with them.
In addition to the TPB variables, this study examined understanding of COVID-19 restrictions. Although previous research has examined knowledge of COVID-19 [17], limited research has examined understanding of restrictions aimed to reduce transmission. As social distancing restrictions frequently change, individuals are likely to have varied knowledge and understanding of current restrictions. This is important as one’s understanding is likely to influence their ATT, SN and PBC. For example, if an individual believes the restrictions are more restricting than they actually are, they might hold more negative ATT, be more likely to perceive others as violating the restrictions when they are not and might perceive lower control over their behavior. Consequently, the inclusion of understanding in this study enabled more accurate predictions of intentions and behaviors than prior studies that did not examine understanding.
That this study found a significant positive relationship between understanding and ATT is congruent with prior research [18]. Individuals might be presumed to hold positive ATT about the importance of social distancing restrictions if they have a greater understanding of them. The relationships between understanding and SN and understanding and PBC were very weak and non-significant. Although this has been found previously, it is possible that for participants to accurately evaluate whether others are complying with restrictions, they require a level of understanding of the restrictions and poor understanding might result in unreliable evaluations of whether others are complying. This could be examined by assessing actual adherence of participants’ families, friends and colleagues, reducing reliance on self-reports of others’ compliance.
Additionally, understanding was not related to PBC, and prior research has also identified a weaker association between understanding and PBC than ATT. It is likely that to perceive having the ability to comply with social distancing restrictions, people require a level of understanding, and poor understanding of restrictions might be a barrier to compliance. It is possible that individuals with poor understanding of restrictions misevaluate their ability to adhere, and this represents an error in their judgment as they perceive the ability to perform behaviors that really violate the restrictions. In future, additional items might be used to measure PBC by asking participants to what extent they perceive they could avoid specific activities.
It is also possible that some individuals had reduced control over their ability to adhere to restrictions, e.g. if pressured by someone who they feel obligated to comply with, such as a person in an authority position at work or a family member who they are unable to move away from. This may explain the non-significant relationship between understanding and PBC, as although understanding could act as a barrier to adhering to social distancing restrictions, factors such as the others’ behavior may also influence people’s perceived control over their behavior.
Theoretical and practical implications
This study identified a positive correlation between understanding of social distancing restrictions and ATT toward restrictions. In addition, having a greater understanding of restrictions predicted intentions to adhere to them. Prior research has suggested that understanding of COVID-19 and recommended protocols indirectly influence intentions to adhere to recommendations through perceived vulnerability and severity of COVID-19 [18]. In a different study using an Australian sample, increased knowledge of pandemic influenza was associated with higher reported willingness to quarantine, avoid public events and postpone social gatherings [22], and people’s willingness to comply increased further following a short explanation about pandemic disease. This might be due to the explanations increasing individuals’ perceived severity and vulnerability, as reported earlier [18].
Overall, participants demonstrated the greatest understanding of violating behaviors when the protagonists hugged another person, remained at work when exhibiting symptoms of sickness and completing non-essential shopping with people from another household. These scenarios described actions that violated the ‘In public’ restrictions. Conversely, the lowest understanding was on scenarios whereby the protagonist ate in the lunchroom with a colleague and exercised with more than one other person. It might be valuable to provide examples of actions that are allowed by the restrictions compared with actions that are prohibited, as it is possible participants who perceived these were allowed did so due to the activities being permitted, while failing to account for finer details such as group size. The use of examples in public messaging might increase the understanding of the restrictions and therefore intentions to comply.
The results of this study provide support for increased education of the public regarding the COVID-19 pandemic to maximize understanding of the restrictions and subsequently compliance. It is possible that conflicting information or frequent changes to social distancing restrictions might result in confusion, and this may lead to intentions to inadvertently violate the restrictions imposed to reduce transmission. To promote understanding of restrictions, communication from authorities regarding restrictions should be clear and consistent, should use simple language, might include a short video and might be tested on a subset of the population before releasing the messaging more widely to ensure understanding [23]. It may also be advantageous to provide examples such as those used in the vignettes from this study, to explain the relevance of restrictions for individuals’ day-to-day lives, link information to previous knowledge (such as previous stages of restrictions) and to repeat the restrictions to maximize understanding [24]. When releasing written information, limiting the amount of text used, using only essential information and using bullet points might enhance understanding, particularly for individuals with poorer reading skills [24].
In addition, that PBC directly influenced behavior demonstrates the importance of barriers to adhering to restrictions. Policy makers should identify concerns held by the public regarding social distancing (e.g. fear of financial insecurity [16], access to groceries and other essential supplies [15]) and should implement strategies to minimize these. This is likely to enhance compliance with the restrictions in individuals with intentions to otherwise adhere.
Strengths
A strength of this study is the use of vignettes to assess intentions and understanding of restrictions. Previous research has shown that people are poor at predicting their own behavior, e.g. when exposed to racism [25] and when presented with the opportunity to perform prosocial behaviors [26]. This poses challenges to the utility of self-report measures that ask participants about their intentions directly. The use of vignettes aimed to improve on this as participants were asked about their anticipated actions within specific scenarios where the desired action was concealed. This method of examining intentions is also likely to be more accurate than asking participants about their intentions to adhere to restrictions generally as it did not rely on them having accurate understanding of the restrictions. The vignettes also provided the standardization of contextual information and the presentation of the restrictions before the vignettes controlled for differences in participants’ prior knowledge of the restrictions.
This study also measured self-reported behavior, as much previous research has failed to assess behavior [13]. Although intentions have been shown to predict behavior [18], individuals’ ability to adhere to restrictions is thought to directly influence adherence, particularly for behaviors under low volitional control [9]. By assessing behavior, this allowed for the direct effect of PBC on behavior to be examined, and it highlighted the importance of individuals’ perceiving the resources and opportunity to adhere to the restrictions on compliance.
Limitations and future directions
A limitation of this study is the sample that was used, including the use of participants between 18 and 63 years at the time of participation. It is likely older individuals face different challenges with accessing up-to-date information regarding social distancing restrictions (e.g. due to familiarity with news outlets and other information sources), and they may experience different challenges with adhering to the restrictions due to having less work or social commitments than younger adults. Age has been identified as a factor associated with knowledge of the COVID-19 virus, where older age is often associated with higher knowledge [27]. One study has shown people aged 51–65 years to have higher knowledge of transmission modes and preventative practices than people 35–50 years old, and the lowest knowledge in people aged 20–35 years [28]. Therefore, it would be valuable to examine the predictors of intention and behavior in adults older than 63 years.
There was also a greater proportion of female participants than male, and employment within primary education and health fields were overrepresented. Given the overrepresentation of the education and allied health fields, it is possible that understanding was higher in the sample used than in the general population and ATT and SN of social distancing may have also been more positive. However, statistical analyses revealed no major differences in results for males and females and found no differences in relationships based on education. Nevertheless, future research should examine whether these relationships remain consistent in larger samples that are more representative of the broader population. Additionally, the results of this study should not be generalized to people without internet access, as this was a requirement to participate in the study.
Due to the relatively small sample size, it is likely that there was insufficient statistical power to identify weaker relationships in the model. Due to changes in the national COVID-19 social distancing restrictions being implemented on 1 June 2020, data collection was ceased on 30 May 2020. Replication of this research using a larger sample size would provide greater statistical power and a more stable model, providing further support for the findings. This would be valuable to further examine the relationships between SN and PBC on intentions, which have been shown to be weaker predictors of intentions than ATT [13].
The method of assessing behavior using self-reports also poses a limitation to the current study. As discussed, this method of data collection can increase the risk of socially desirable responding when obtaining information with potential negative public health or legal consequences [29]. Due to socially desirable responding, it should be noted that actual violations may have been higher than the number reported. In future, observations of behavior might produce additional valuable findings regarding compliance with social distancing.
Another potential limitation of this study relates to order effects. Participants completed the ATT, SN and PBC scales before reading the list of government restrictions, and they responded to the understanding, intentions and behavior scales after viewing the restrictions. It is possible that participants’ understanding of the restrictions increased as a result of their exposure to the restrictions, and this could have resulted in different ATT, SN or PBC being reported to those held when responding to the vignettes. However, due to the restrictions being applicable nationally for a minimum of 6 weeks before data collection commenced, it is unlikely that participants had no or very limited knowledge of restrictions when completing the earlier scales, as it is expected that they had some knowledge of the restrictions from earlier exposure to televised press conferences and other media sources. While provision of the restrictions may have influenced understanding and intentions, this was also deemed necessary to standardize exposure to the current restrictions, given frequent changes to them. To minimize the influence of new knowledge of the restrictions on behavior, participants were also asked to report on specific behaviors over the past month rather than indicating to what extent they believed they violated restrictions. Future research should aim to address this, however, to determine if viewing the list of restrictions after completing the ATT, SN and PBC scales caused a change in the assessment of these factors compared with intentions.
In future, this research could be replicated using a longitudinal design, whereby behavior is assessed at a later timepoint. This would enable causal assumptions to be made, where intentions precede the performance of reported or observed behaviors. It was assumed that participants held comparable ATT, SN and PBC at the time of completion compared with the month prior due to the short time period participants were asked to consider when indicating past behavior. It was not possible within this study to collect data from several timepoints due to scheduled changes to restrictions, but it would be an important point for clarification in future research.
Another avenue for further work includes research into predictors of compliance with social distancing at varying stages of restrictions. This would be particularly beneficial as transmission has been shown to increase after the easing of restrictions, and continued compliance during subsequent waves of infectious disease outbreaks would further reduce the overall morbidity and mortality [3]. Further research might be undertaken during subsequent waves of the COVID-19 pandemic within Australia, should they occur.
Conclusion
This study used a modified version of the TPB as a framework to identify predictors of social distancing compliance in an Australian sample, and it additionally assessed the understanding of social distancing restrictions. Understanding of restrictions and ATT toward them were important predictors of intentions to adhere to restrictions. These intentions, with PBC, significantly predicted participants’ past behavior during the COVID-19 pandemic. Future research should examine the predictors of social distancing compliance during subsequent stages of social distancing restrictions, utilizing a longitudinal design to allow for causal relationships to be examined and using a larger and more diverse sample for greater generalizability of results.
Acknowledgements
We would like to thank the individuals who took the time to participate in this study.
Contributor Information
J Thacker, School of Psychology, University of Adelaide, 259 North Terrace, Adelaide, South Australia 5000, Australia.
D Sturman, School of Psychology, University of Adelaide, 259 North Terrace, Adelaide, South Australia 5000, Australia.
J Auton, School of Psychology, University of Adelaide, 259 North Terrace, Adelaide, South Australia 5000, Australia.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
None declared.
References
- 1. Ahmad M, Iram K, Jabeen G. Perception-based influence factors of intention to adopt COVID-19 epidemic prevention in China. Environ Res 2020; 190: 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Wilder-Smith A, Freedman DO. Isolation, quarantine, social distancing and community containment: pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J Travel Med 2020; 27: 1–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Hatchett RJ, Mecher CE, Lipsitch M. Public health interventions and epidemic intensity during the 1918 influenza pandemic. Proc Natl Acad Sci USA 2007; 104: 7582–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Chang SL, Harding N, Zachreson C et al. Modelling transmission and control of the COVID-19 pandemic in Australia. Nat Commun 2020; 11: 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Armitage CJ, Conner M. Social cognition models and health behaviour: a structured review. Psychol Health 2000; 15: 173–89. [Google Scholar]
- 6. Rutter D, Quine L. Social cognition models and changing health behaviours. In: Rutter D, Quine L (eds). Changing Health Behaviour: Intervention and Research with Social Cognition Models. Buckingham, England: Open University Press, 2002, 1–27. [Google Scholar]
- 7. McEachan RRC, Conner M, Taylor NJ et al. Prospective prediction of health-related behaviours with the Theory of Planned Behaviour: a meta-analysis. Health Psychol Rev 2011; 5: 97–144. [Google Scholar]
- 8. Armitage CJ, Conner M. Efficacy of the Theory of Planned Behaviour: a meta‐analytic review. Br J Social Psychol 2001; 40: 471–99. [DOI] [PubMed] [Google Scholar]
- 9. Ajzen I. The Theory of Planned Behavior. Organ Behav Hum Decis Process 1991; 50: 179–211. [Google Scholar]
- 10. Tang CS, Wong CY. An outbreak of the severe acute respiratory syndrome: predictors of health behaviors and effect of community prevention measures in Hong Kong, China. Am J Public Health 2003; 93: 1887–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Vaughan E, Tinker T. Effective health risk communication about pandemic influenza for vulnerable populations. Am J Public Health 2009; 99: S324–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Coroiu A, Moran C, Campbell T et al. Barriers and facilitators of adherence to social distancing recommendations among a large international sample of adults. PLoS One 2020; 15: e0239795.doi: 10.31219/osf.io/62g7z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Zhang X, Wang F, Zhu C et al. Willingness to self-isolate when facing a pandemic risk: model, empirical test, and policy recommendations. Int J Environ Res Public Health 2020; 17: 197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Jiang X, Elam G, Yuen C et al. The perceived threat of SARS and its impact on precautionary actions and adverse consequences: a qualitative study among Chinese communities in the United Kingdom and the Netherlands. Int J Behav Med 2009; 16: 58–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Webster RK, Brooks SK, Smith LE et al. How to improve adherence with quarantine: rapid review of the evidence. Public Health 2020; 182: 163–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Bodas M, Peleg K. Self-isolation compliance in the COVID-19 era influenced by compensation: findings from a recent survey in Israel. Health Aff 2020; 39: 936–94. [DOI] [PubMed] [Google Scholar]
- 17. Zhong BL, Luo W, Li HM et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci 2020; 16: 1745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Prasetyo YT, Castillo AM, Salonga LJ et al. Factors affecting perceived effectiveness of COVID-19 prevention measures among Filipino during enhanced community quarantine in Luzon, Philippines: integrating Protection Motivation Theory and Extended Theory of Planned Behavior. Int J Infect Dis 2020; 99: 312–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Wason KD, Polonsky MJ, Hyman MR. Designing vignette studies in marketing. Australas Marketing J 2002; 10: 41–58. [Google Scholar]
- 20. Georgiou N, Delfabbro P, Balzan R. COVID-19-related conspiracy beliefs and their relationship with perceived stress and pre-existing conspiracy beliefs. Pers Individ Dif 2020; 166: 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Godin G, Kok G. The theory of planned behavior: a review of its applications to health-related behaviors. Am J Health Promot 1996; 11: 87–98. [DOI] [PubMed] [Google Scholar]
- 22. Eastwood K, Durrheim D, Francis JL et al. Knowledge about pandemic influenza and compliance with containment measures among Australians. Bull World Health Organ 2009; 87: 588–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Raynor DK. Health literacy. Br Med J 2012; 344: e2188. [DOI] [PubMed] [Google Scholar]
- 24. Andrus MR, Roth MT. Health literacy: a review. Pharmacotherapy 2002; 22: 282–302. [DOI] [PubMed] [Google Scholar]
- 25. Kawakami K, Dunn E, Karmali F et al. Mispredicting affective and behavioral responses to racism. Science 2009; 323: 276–8. [DOI] [PubMed] [Google Scholar]
- 26. Balcetis E, Dunning D. Considering the situation: why people are better social psychologists than self-psychologists. Self Identity 2013; 12: 1–15. [Google Scholar]
- 27. Defar A, Molla G, Abdella S et al. Knowledge, practice and associated factors towards the prevention of COVID-19 among high-risk groups: a cross-sectional study in Addis Ababa, Ethiopia. PLoS One 2021; 16: e0248420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Labban L, Thallaj N, Labban A. Assessing the level of awareness and knowledge of COVID 19 pandemic among Syrians. Arch Med 2020; 12: 8. [Google Scholar]
- 29. Walzenbach S. Hiding sensitive topics by design? An experiment on the reduction of social desirability bias in factorial surveys. Surv Res Methods 2019; 13: 103–21. [Google Scholar]