
Figure 1. Coil Placement and Primary Outcomes.
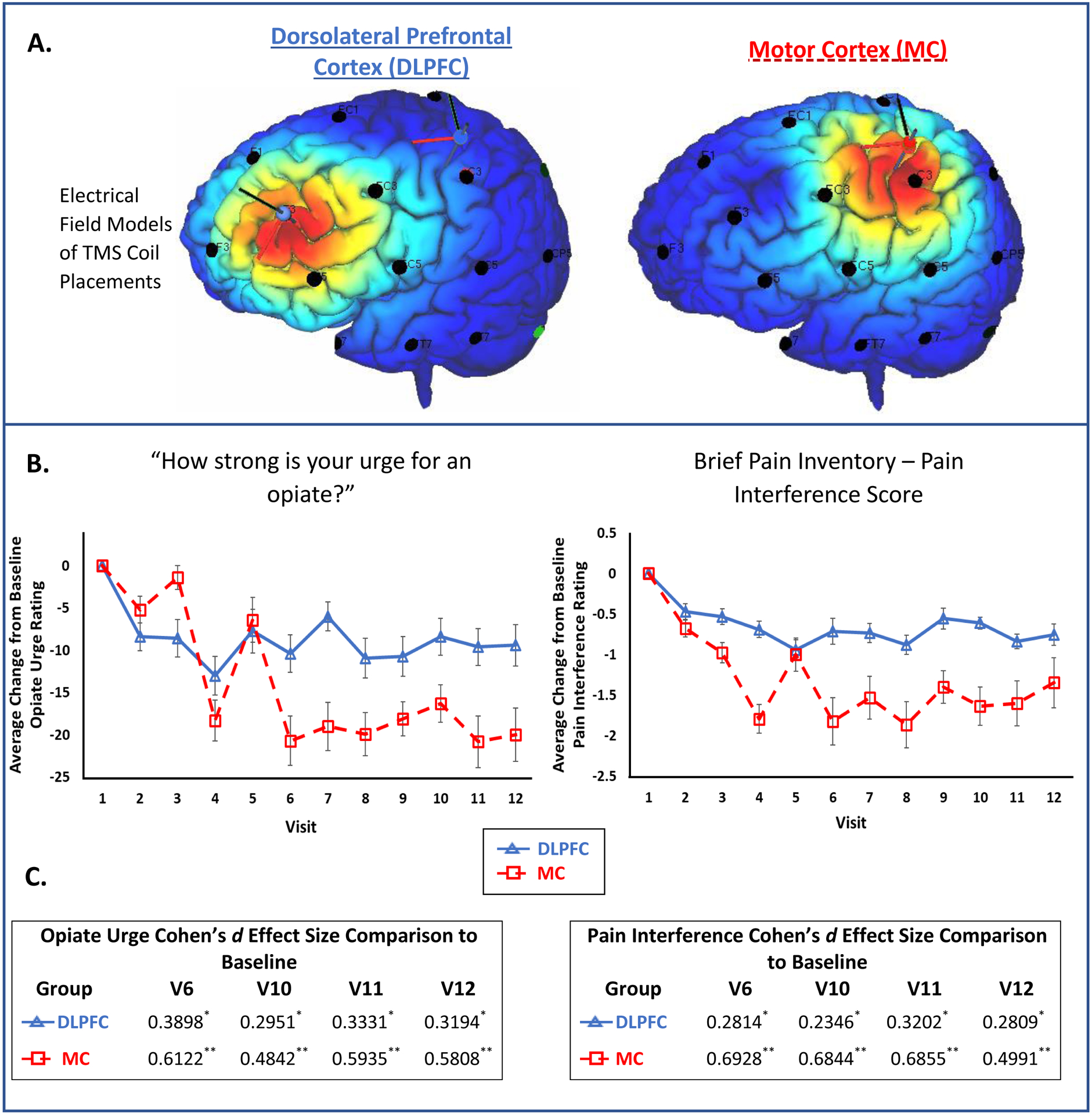
A) These chronic back pain participants currently taking prescription opiates were randomized to receive 10Hz rTMS to the left DLPFC (top left, F3 placement based on prior work in the depression and addiction field) or the left MC (top right, 20% distance from apex-tragus a territory that overlapped the somatotopic representation of the arm and trunk; SimNIBS 3.1). The e-field modeling is based on a standardized MNI template to provide a graphical illustration of the targets used. B) Self-reported assessment of pain and opiate craving was collected (see Supplementary figure 2 for full details). The data represent the average change [± standard error] from visit 1, specifically, for opiate urge (F1,216=3.248, p=0.073) and pain interference score (F1,216=8.447, p=0.004). C) The effect of rTMS on opiate urge and pain interference as defined by effect sizes for visits 6, 10, 11, and 12. Categories of the effect size are indicated (Cohen’s d): * small effect (0.2–0.5), ** moderate effect (0.5–0.8), *** large effect (>0.8).