

Abstract
Objective:
Only a minority of drug and alcohol users develops a substance use disorder. Previous studies suggest that this differential vulnerability commonly reflects a developmental trajectory characterized by diverse externalizing behaviors. In this study, we examined the relation between child and adolescent externalizing behaviors and adolescent substance use in a prospectively followed Canadian birth cohort, accounting for the temporal sequence of a wide variety of contributing factors.
Methods:
Two hundred and forty-two adolescents followed since birth (date range: 1996 to 2012) were assessed on externalizing behavior (age 17 months to 16 years), alcohol and cannabis use at age 16, age of alcohol use onset, family history of substance use problems, family functioning (age 11 to 15), sensation seeking (age 16), prenatal substance exposure, socioeconomic status (age 1 to 9), and sex.
Results:
Age of alcohol use onset was predicted by a family history of substance use problems, externalizing traits from ages 6 to 10 and 11 to 16, sensation seeking at age 16, prenatal alcohol and tobacco exposure and family functioning at ages 11 to 15. High frequencies of alcohol and cannabis use at age 16 were both predicted by externalizing traits from ages 11 to 16, a family history of substance use problems and sensation seeking after controlling for other individual, environmental and familial variables. The association between familial substance use problems and substance use during adolescence was partially mediated by externalizing traits from age 11 to 16.
Conclusions:
The present findings provide prospective evidence for a developmental risk pathway for adolescent substance use, potentially identifying those who could benefit from early interventions.
Keywords: externalizing traits, alcohol, cannabis, familial risk, sensation seeking
Abstract
Objectif:
Seule une minorité d’utilisateurs de drogues et d’alcool développe un trouble d’utilisation de substances. Les études précédentes suggèrent que cette vulnérabilité différentielle reflète communément une trajectoire développementale caractérisée par divers comportements extériorisés. Dans la présente étude, nous avons examiné la relation entre les comportements extériorisés des enfants et des adolescents et l’utilisation de substances des adolescents dans une cohorte de naissance canadienne suivie prospectivement, représentant la séquence temporelle d’une vaste variété de facteurs contributifs.
Méthodes:
Deux cent quarante-deux adolescents suivis depuis la naissance (période : 1996-2012) ont été évalués quant aux comportements extériorisés (âge 17 mois -16 ans), à l’utilisation d’alcool et de cannabis à 16 ans, âge d’initiation à la consommation d’alcool, aux antécédents familiaux de problèmes d’utilisation de substances, au fonctionnement familial (11-15 ans), à la recherche de sensations (16 ans), à l’exposition prénatale aux substances, au statut socio-économique (1-9 ans), et au sexe.
Résultats:
L’âge du début de l’utilisation d’alcool était prédit par les antécédents familiaux de problèmes d’utilisation de substances, les traits extériorisés de 6-10 ans et de 11-16 ans, la recherche de sensations à 16 ans, l’exposition prénatale à l’alcool et au tabac, et le fonctionnement familial de 11-15 ans. Des fréquences élevées d’utilisation d’alcool et de cannabis à 16 ans étaient toutes deux prédites par les traits extériorisés de 11 à 16 ans, des antécédents familiaux de problèmes d’utilisation de substances et la recherche de sensations après contrôle d’autres variables individuelles, environnementales et familiales. L’association entre les problèmes familiaux d’utilisation de substances et l’utilisation de substances durant l’adolescence était expliquée partiellement par les traits extériorisés de 11 à 16 ans.
Conclusions:
Ces résultats offrent des données probantes prospectives pour une trajectoire de risque développemental de l’utilisation de substances à l’adolescence, identifiant potentiellement ceux qui pourraient bénéficier d’interventions précoces.
Introduction
Adolescent drug and alcohol use is normative behavior in Europe, the United States, and Canada, 1 yet only a minority develops a substance use disorder (SUD). This differential vulnerability is thought to reflect a developmental trajectory characterized by diverse externalizing traits (EXT) including impulsivity, risk-taking, and oppositional and aggressive behaviors. 2 –6 For example, longitudinal studies, by us and others, have demonstrated that EXT during late childhood and adolescence predict alcohol and cannabis consumption and alcohol use problems later in life. 7 –14 These studies did not, however, have data from early childhood (0 to 6 years). The potential importance of these missing data is underscored by evidence from a small number of studies that an early childhood (age 3 to 5) EXT-related feature (low reactive control) predicts alcohol use and substance use problems later in life. 5,6,15 Together, these findings raise the possibility that the EXT pathway to SUDs begins earlier than previously thought.
The general liability to EXT is largely explained by genetic factors (up to 80%), 16 with the exact expression seeming to reflect a combination of genetic, environmental, and individual factors. 17,18 Similarly, substance use and SUDs have been associated with family functioning (FF), 6,19 socioeconomic status, 20 impulsivity and sensation seeking, 18,21 –23 prenatal substance exposure, 24,25 and stressful life events. 26 Although internalizing traits have also been linked to substance use and related disorders, 27 recent evidence suggests that the primary effect of these traits on early onset substance use is either protective or, when aggravating, a function of their overlap with EXT. 28,29 Since the magnitude of these associations can vary at different stages throughout the lifetime and may depend on the presence of other genetic or environmental risk factors, 30 –32 obtaining an integrated understanding of developmental risk factors for substance use and SUDs will require prospective longitudinal designs.
In the current study, we used a prospective design to assess the links between EXT from early childhood to adolescence and adolescent alcohol and cannabis use. Participants recruited from a community sample were assessed annually from the age of 17 months, allowing us to prospectively observe time-specific developmental changes with a markedly decreased risk of recall bias. The assessment of a range of hypothesized risk factors across key developmental periods allowed us to identify the specific contribution of individual, familial, and environmental variables, including family history of substance use problems (FH+), FF (age 11 to 15), sensation seeking (age 16), 28 prenatal substance exposure, and socioeconomic status in predicting adolescent substance use (see Supplementary Information for more details on the selection of risk factors). With this design, we aimed to replicate evidence for an externalizing risk pathway to adolescent substance use in a Canadian birth cohort using a consistent measure of EXT from early childhood to adolescence. We further extend previous findings by identifying the contribution of sensation seeking. Sensation seeking has been proposed as an independent pathway from impulsive traits (a subcomponent of EXT) in predicting adolescent substance use. 18,33,34 Whereas sensation seeking is generally defined as a strong need for stimulation and a willingness to take risks for the sake of having novel experiences, impulsivity reflects the inability to control or regulate emotions and behaviors. 35 These distinct traits have been linked to different motivational pathways to substance use, a drive to seek out enhanced positive stimulation versus the inability to control behavior in order to avoid negative consequences. 34
In this context, we tested the following hypotheses. First, if a liability to EXT is an enduring risk trait, we expected externalizing features to be fairly stable from early childhood to adolescence. 36 Second, we hypothesized that high EXT from early childhood to adolescence would predict alcohol and cannabis use frequency at age 16 and an earlier age of alcohol use onset (AAO), 37,38 controlling for FH+, sensation seeking, FF, socioeconomic status, and prenatal substance exposure. Third, in line with previous research, we predicted a significant association between FH+, a reflection of both genetic risk and familial–environmental risk, and adolescent substance use. 39 It has been proposed that this familial risk to substance use problems could reflect the transmission of a general liability that increases the risk of a broad spectrum of externalizing disorders in offspring rather than a specific disease (such as SUD). 16 In this regard, we predicted that EXT during childhood and/or adolescence would mediate the association between parental substance use problems and offspring adolescent substance use. 5,6,13,40,41 Finally, since sensation seeking has been proposed as being separable from other impulsive traits, 18,33,34 we predicted that it would provide a unique and independent contribution to the model after controlling for EXT and other individual, familial and environmental variables.
Methods
Participants
Participants were recruited from the first wave of the ongoing Quebec Longitudinal Study of Child Development. At inception, this sample included 572 Francophone (90%) and Anglophone (10%) families from all socioeconomic backgrounds who were part of 1,000 randomly selected families from urban areas in the 1996 Quebec birth registry. 42 Out of 1,000 selected families, 71 were not eligible because they moved to a different region or because they did not speak French or English. Three hundred and fifty-seven households declined to participate (n = 51 because of illness or death in the family, n = 221 for other reasons) or could not be reached because of unknown contact information (n = 70) or prolonged absence (n = 15). The remaining 572 participants were first assessed at 5 months old, in 1996, and have been subsequently followed annually. Thus, data described here range from year 1996 to 2012. Only individuals who were seen at least once between age 11 and 16 years were included. As a result of attrition or nonresponse during this period, data from 242 adolescents (128 males), aged 16 years, were available for this study. The final subsample did not differ significantly from the remainder of the initial sample with respect to sex (P = 0.50, n = 572), EXT from age 17 months to 5 years (P = 0.7, n = 509), family income at age 5 months (P = 0.15, n = 538) or FH+ (P = 0.89, n = 454). The study was approved by the ethics committees of University of Montreal, the Hôpital Louis Hippolyte Lafontaine, and the CHU Sainte-Justine Research Center.
Measures
EXT
EXT were assessed yearly using the Social Behavior Questionnaire. 43,44 Mean scores were calculated for 3 developmental periods for the following subscales: hyperactivity, impulsivity, oppositional behavior, nonaggressive behavioral problems, physical aggression, proactive aggression, indirect aggression, and reactive aggression. Individual items were scored using a 3-point scale (“never/not true,” “sometimes/a little true,” “often/very true”). Composite scores of EXT were aggregated within 3 time periods using a minimum of 2 data points per time period: (1) preschool years (EXT 17m-5y; data collected at 17, 30, 42, and 60 months), (2) early school years (EXT 6-10; data collected at 72, 84, 108, and 120 months), and (3) adolescence (EXT 11-16; data collected at age 11, 12, 13, 14, 15, and 16 years). Preschool data (EXT 17m-5y) were acquired through mother ratings and included only 1 type of aggressive behavior, physical aggression. Early school data (EXT 6-10) were acquired through teacher ratings, 45 and adolescent scores (EXT 11-16) were obtained through self-report measures.
Substance use
Frequencies of alcohol and drug use, including cannabis, cocaine, amphetamine, hallucinogens, heroin, and other nonprescription drugs, were measured through self-report questionnaires at 16 years (Table 1). 46 All substance use measures assessed age of first use (Table 2) and frequency of consumption during the past 12 months, via a 7-point scale (1 = “have not consumed during the past 12 months” to 7 = “consumed every day”). Since illicit substance use was minimal (< 10% of participants, see Table 1), we only included measures on alcohol and cannabis use in our analyses. Self-report age of onset of substance use was only available for alcohol and for all substances combined.
Table 1.
Substance Use at Age 16 Years (%).
| Substance Use: Age 16 Years | Alcohol | Cannabis | Cocaine | Hallucinogens | Amphetamines | Heroin | Other Nonprescription Drugs |
|---|---|---|---|---|---|---|---|
| Never consumed | 17.3 | 56.3 | 95.8 | 90.4 | 91.6 | 99.4 | 99.4 |
| Not in the past year | 3 | 7.8 | |||||
| Just once | 4.8 | 8.4 | 2.4 | 5.4 | 3.0 | 0.6 | |
| Less than once per month | 32.7 | 13.2 | 1.2 | 2.4 | 1.8 | 0.6 | |
| Once per month | 26.2 | 5.4 | 1.2 | ||||
| Weekends only | 14.3 | 2.4 | 1.2 | 1.8 | |||
| 3 Times or more per week | 1.2 | 1.8 | 0.6 | 0.6 | 0.6 | 0.6 | |
| Every day | 0.5 | 4.7 | 0.6 | ||||
| Total | 100 | 100 | 100 | 100 | 100 | 100 |
Table 2.
Age of First use of Alcohol and Drugs (%).
| Alcohol | Recreational Drugsa | |||
|---|---|---|---|---|
| Age of First Use | % | Cumulative | % | Cumulative |
| 10 Years or younger | 3.2 | 3.2 | 1.2 | 1.2 |
| 11 Years | 0 | 3.2 | 1.2 | 2.4 |
| 12 Years | 8.2 | 11.4 | 1.8 | 4.2 |
| 13 Years | 12.6 | 24 | 3.6 | 7.8 |
| 14 Years | 22 | 46 | 11.4 | 19.2 |
| 15 Years | 32 | 78 | 13.8 | 33 |
| 16 Years | 3.8 | 81.8 | 4.2 | 37.2 |
| Never used | 18.2 | 62.8 | ||
a Includes cannabis, cocaine, amphetamine, heroin, hallucinogens and other nonprescription drugs.
Family history of substance use problems (FH+)
A subset of DSM-IV criteria for drug and alcohol use disorders was evaluated in both parents using a self-report questionnaire (Supplementary Table 1) when participants were 17 months (for father) and 30 months (for mother). FH+ was defined as having at least 1 parent meeting at least 1 DSM-IV criterion for either alcohol or drug dependence.
Sensation seeking
The Substance Use Risk Profile Scale (SURPS) 47 was administered at 16 years to assess sensation seeking (SS). The SURPS possesses good internal consistency, test–retest reliability, and both concurrent and predictive validity of substance use and SUDs during adolescence 33,48,28 and adulthood. 22
Socioeconomic variables
Family income was assessed annually from age 5 months to 9 years. Income was scored on a scale from 1 to 8 (1= < CAD 10,000, 8 = > CAD 80,000). Mean scores were calculated per individual.
Prenatal substance exposure
Maternal substance use was obtained from prenatal medical records. Maternal cigarette use was defined as the number of cigarettes smoked per day, and alcohol and drug use frequency were assessed on 7-point scales (from 1= “never” to 7 = “every day”). 49 Two mothers reported drug use other than alcohol or tobacco during pregnancy—these families were excluded from the analyses.
FF
FF was assessed annually using the McMaster Family Assessment Device. 50 The General Functioning (GF) subscale of the McMaster Family Assessment Device is a 12-item self-report measure of FF in 6 domains, including problem-solving, communication, parenting roles, affective responsiveness, affective involvement, and behavioral control. Responses were scored using a 4-point scale (“strongly disagree,” “disagree,” “strongly agree,” and “agree”). The GF subscale possesses good internal consistency, reliability, and construct validity. 51 Average summed scores were included for age 11 to 15 years. 19 Given the absence of a validated and objective measure of stressful life events in the dataset, FF along with FH+ were considered proxies since both are strongly associated with childhood stress exposure and contribute to the risk of environmental stressors. 52
Data Analysis
Multiple regression analyses were conducted in SPSS version 21 to identify predictors of (i) AAO, (ii) alcohol use frequency at 16 years, and (iii) cannabis use frequency at 16 years. Independent measures included EXT at 3 time points (EXT 17m-5y, EXT 6-10, and EXT 11-16), FH+, SS, FF, socioeconomic status, sex, and prenatal alcohol and tobacco exposure. An expectation maximization algorithm, using maximum likelihood estimation, was applied to impute missing values (Supplementary Table 2). Logistic regression analysis demonstrated that the absence of data, which was largely a result of loss to follow up, was not predicted by EXT scores during any period, sex, family income, FH+, prenatal substance use, or FF (P > 0.1).
For each substance use measure, a statistical regression was conducted including all independent variables using a backward elimination method to remove those independent variables that do not contribute significantly to the model. Then, significant predictors identified by Step 1 were entered in a sequential regression to determine the unique and overlapping contribution to the explained variance of the dependent variables.
Mediation effects were assessed using the product of coefficients method, which directly assessed whether the mediation or indirect effect was significant. Significance and confidence intervals for testing mediation effects were calculated using the RMediation package, 53 which is based on MacKinnon’s distribution of the product method. This method has been shown to have more accurate Type I error rates and more power than other tests. 54,55
Results
Zero-order Correlations
As shown in Table 3, many of the variables of interest co-varied. EXT during the first 5 years of life (EXT 17m-5y) were positively associated with scores later in life. EXT at all ages correlated positively with prenatal tobacco exposure and FF at ages 11 to 15 years and negatively with family income. EXT 11-16 also correlated positively with SS scores at 16 years and with having FH+. In turn, having FH+ correlated positively with prenatal tobacco exposure and negatively with family income. Finally, EXT 17m-5y and EXT 6-10 were higher in boys than girls, as reflected by negative correlations between sex and EXT at these ages.
Table 3.
Correlations between Substance use Measures, Externalizing Traits, Family History of Substance use Problems, Sensation Seeking, Demographic Information, Prenatal Substance Exposure, and Family Functioning.
| FH+ | EXT 17m-5y | EXT 6-10 | EXT 11-16 | SS 16 | Sex | Prenatal Smoking | Prenatal Alcohol | Family Income | FF 11-15 | |
|---|---|---|---|---|---|---|---|---|---|---|
| AAO | −0.23** | 0.04 | −0.22** | −0.32** | −0.33** | −0.03 | −0.19** | −0.19** | 0.05 | 0.11 |
| Alc Use 16 | 0.18** | −0.06 | 0.11 | 0.23** | 0.35** | 0.05 | 0.11 | 0.03 | −0.05 | 0.03 |
| Can Use 16 | 0.17* | 0.01 | 0.08 | 0.32** | 0.28** | −0.07 | 0.11 | −0.04 | −0.09 | 0.02 |
| FH+ | 0.07 | −0.01 | 0.20** | 0.05 | −0.01 | 0.23** | −0.01 | −0.24** | −0.07 | |
| EXT 17m-5y | 0.34** | 0.22** | −0.01 | −0.20** | 0.16* | 0.07 | −0.19** | 0.29** | ||
| EXT 6-10 | 0.33** | 0.1 | −0.27** | 0.16* | −0.02 | −0.17** | 0.17** | |||
| EXT 11-16 | 0.21** | −0.11 | 0.17** | −0.07 | −0.22** | 0.14* | ||||
| SS 16 years | −0.07 | −0.00 | 0.03 | −0.03 | −0.12 | |||||
Note. AAO = age of alcohol use onset; Alc Use 16 = alcohol use frequency at age 16; Can Use 16: cannabis use frequency at age 16; EXT = externalizing traits; FF = family functioning; FH+ = family history of substance use problems; SS = sensation seeking.
* Significant at P < 0.05. **Significant at P < 0.01.
FH+, EXT 11-16, and SS scores were all associated positively with alcohol and cannabis use frequency at 16 years and negatively with AAO. Earlier AAO was also associated with EXT 6-10, and prenatal tobacco and alcohol exposure (Table 3).
Multiple Regressions—Direct and Indirect Effects
Statistical regressions using backward elimination demonstrated that only EXT 11-16, FH+, and SS remained statistically significant predictors of alcohol, R 2 = 0.183, F(3, 221) = 16.31, P < 0.001, and cannabis use, R 2 = 0.169, F(3, 221) = 14.8, P < 0.001, at 16 years, after controlling for potential confounds (sex, family income, prenatal substance exposure and FF). In addition to EXT 11-16, FH+, and SS, AAO was predicted by EXT 6-10, prenatal alcohol and tobacco exposure, and FF, R 2 = 0.291, F(7, 221) = 14.37, P < 0.001.
Sequential regressions that included the significant predictors as determined by the backward elimination method were conducted to assess the unique and overlapping contribution of each predictor (Table 4). The results show that the effect of FH+ on each measure of substance use was significantly reduced when EXT 11-16 was added to the model, with a reduction of 22%, 35%, and 24% in β coefficients for alcohol use frequency, cannabis use frequency, and AAO, respectively. Despite the extent of this shared variance between FH+ and EXT 11-16 explaining substance use, both contributed independently to the model.
Table 4.
Hierarchical Regression Evaluating the Relationship between Substance Use. Measures, FH+, Externalizing Traits, and Sensation Seeking (SS).
| Substance Use Measure | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Alc. Freq (R 2 = 0.18) | Can. Freq (R 2 = 0.18) | AAO (R 2 = 0.29) | ||||||||
| Modela | β | t | P | β | t | P | β | t | P | |
| 1 | FH | 0.182 | 2.74 | 0.007 | 0.166 | 2.49 | 0.014 | −0.173 | −2.64 | 0.009 |
| 2 | FH | −0.178 | −2.83 | 0.065 | ||||||
| EXT 6-10 | −0.270 | −4.37 | 0.000 | |||||||
| 3 | FH | 0.142 | 2.14 | 0.033 | 0.108 | 1.67 | 0.097 | −0.132 | −2.12 | 0.035 |
| EXT 6-10 | −0.191 | −3.01 | 0.003 | |||||||
| EXT 11-16 | 0.202 | 3.04 | 0.003 | 0.290 | 4.46 | 0.000 | −0.245 | −3.77 | 0.000 | |
| 4 | FH | 0.138 | 2.21 | 0.028 | 0.106 | 1.68 | 0.095 | −0.130 | −2.19 | 0.029 |
| EXT 6-10 | −0.184 | −3.03 | 0.003 | |||||||
| EXT 11-16 | 0.135 | 2.12 | 0.035 | 0.241 | 3.75 | 0.000 | −0.185 | −2.93 | 0.004 | |
| SS | 0.340 | 5.45 | 0.000 | 0.252 | 3.99 | 0.000 | −0.275 | −4.71 | 0.000 | |
Note. AAO = age of alcohol use onset; Alc. Freq = alcohol use frequency at age 16; Can. Freq = cannabis use frequency at age 16.
a Controlled for those variables that were significant as determined by the backward elimination regression. For AAO, the model was controlled for prenatal alcohol and tobacco exposure and family functioning. For Alc. Freq. and Can. Freq., no other variables predicted alcohol and cannabis use frequencies and thus no covariates were included here.
Shared explanatory variance was also observed between EXT 11-16 and SS in predicting all outcomes. The β coefficient explaining the effect of EXT 11-16 on alcohol use frequency, cannabis use frequency, and AAO was reduced by 33%, 17%, and 25%, respectively, when SS was added to the model. However, both EXT 11-16 and SS contributed significantly and independently to the model. Finally, although the effect of EXT 6-10 on AAO was considerably reduced (29% reduction in β coefficient) when EXT 11-16 was added to the model, both variables contributed significantly to the model independently.
Mediation Analysis
We next tested whether the effect of FH+ on substance use was partially mediated by adolescent EXT, which was also associated with FH+ in this sample. These analyses indicated that indirect effects of FH+ through EXT 11-16 were significant on all substance use measures (alcohol frequency: ab = 0.109; SE = 0.053; CI, 0.024 to 0.228; AAO: ab = −0.215; SE = 0.087; CI, −0.404 to −0.065; cannabis frequency: ab = 0.192; SE = 0.079; CI, 0.057 to 0.365). These results suggest that EXT 11-16 partially mediates the association between FH+ and substance use outcomes during adolescence (see Figure 1).
Figure 1.
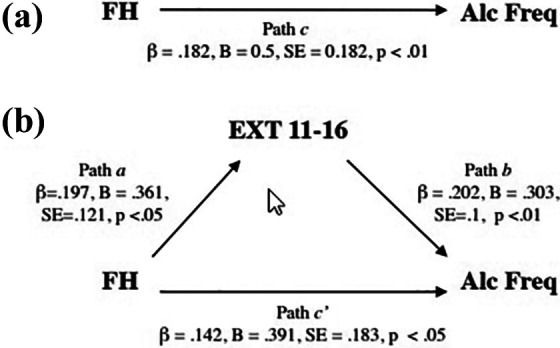
Schematic representation of the relation between FH+ and Alcohol Use Frequency at age 16 years with (b) and without (a) controlling for EXT 11-16 years. The indirect effect from FH+ to alcohol use frequency through EXT 11-16 (reflected by the difference between path c [a] and c’ [b]) was significant (ab = 0.109; SE = 0.053, CI, 0.024 to 0.228). The same associations were seen for alcohol use onset and cannabis use frequency at age 16 years. See details in the Results section.
As associations between substance use and other EXT during adolescence have been found to be bidirectional, post hoc analyses were conducted to clarify the direction of effects. Supplementary Table 3 presents correlations between EXT and alcohol and cannabis use broken down per year during adolescence, illustrating that substance use and EXT were associated across time, suggesting bidirectional associations.
In order to investigate whether the relationship between FH+ and EXT 11-16 may be driven or mediated by substance use, we assessed the association between FH+ and EXT at each year (before and after substance use onset). Supplementary Table 3 illustrates a significant correlation between FH+ and EXT at 11 and 12 years (P < 0.05), when substance use was minimal (alcohol use: 3.2% of sample; drugs: 2.4% of participants, see Table 2), suggesting that the link between FH+ and EXT during these years is not due to substance use.
Discussion
The present prospective birth cohort study found that (1) high EXT scores early in life (ages 1 to 5) predict high scores later in childhood (ages 6 to 10) and adolescence (ages 11 to 16); 2) early AAO was predicted by high EXT scores at ages 6 to 10 and 11 to 16, FH+, and high levels of sensation seeking at age 16; (3) alcohol and cannabis use frequency at age 16 were predicted by high EXT scores at 11 to 16 years, FH+, and high sensation seeking; and (4) the association between FH+ and all 3 measures of substance use (AAO, alcohol and cannabis use frequency at 16 years) was partially mediated by EXT scores at ages 11 to 16. These findings strengthen the conclusions of previous reports showing a link between early EXT and future substance use 2 –4,8,56,57 and extend them by (1) replicating these findings in another Canadian community sample, (2) controlling for demographic features and a variety of environmental influences measured prospectively over a 17-year life span in both parents and offspring, (3) providing evidence that the association between a family history of substance use problems and adolescent substance use is mediated by EXT at ages 11 to 16, and (4) providing support for potentially separate pathways for EXT and sensation seeking predicting adolescent substance use.
The overlap in variance between EXT at ages 6 to 10 and 11 to 16 explaining AAO suggests that EXT remain relatively stable from childhood to adolescence. The consistency of EXT over a lifetime is further supported by the moderate correlations between EXT for each time period (ages 17m-5y, 6-10 and 11-16) and is in line with previous studies. 36 These associations prevail despite the use of cross-informant ratings from one developmental period to the other.
We further demonstrated that the relationship between FH+ and adolescent substance use was partially mediated by EXT at ages 11 to 16. This observation adds to previous findings suggesting that the influence of FH+ on substance use and subsequent problems during adolescence is partially explained by the transmission of EXT. 16,41,58 Notably, a significant relationship between FH+ and EXT was present during adolescence but not earlier in life. This observation underscores the importance of a prospective longitudinal approach and may suggest that the determinants of EXT earlier in life are more heterogeneous than those later in life. 59,60 Those who persist with high levels of EXT throughout adolescence may carry stronger familial risks that predict later development of substance use problems. 16,31
In addition to EXT and having FH+, individual differences in sensation seeking at age 16 significantly predicted concurrent substance use frequency and AAO. Conceptually, sensation seeking shows some overlap with our measure of EXT, which may be reflected by the common variance between these constructs explaining adolescent substance use. 23 However, sensation seeking also provided unique explanatory power to all measures of adolescent substance use after controlling for EXT, suggesting that these 2 constructs may—at least in part—influence substance use via different pathways. This is consistent with previous studies suggesting that sensation seeking may be related to increased substance use through a drive for increased stimulation and positive emotional experiences, whereas impulsivity, a subcomponent of our measure of EXT, may be related to substance use through deficits in self-regulation and inhibitory control. 18,33,34,61
The findings here should be interpreted in light of the following considerations. First, we need to be cautious about the developmental sequence when interpreting the effects on AAO since the age of first drink may have preceded some of the independent variables such as EXT at ages 11 to 16 and sensation seeking at age 16. Thus, the relationship between AAO and EXT at ages 11 to 16 and sensation seeking at 16 years might reflect concurrent associations, where an early AAO increases EXT at ages 11 to 16 and sensation seeking at 16 years and vice versa. This noted, the findings clearly indicate that high childhood EXT precede an early AAO as reflected by a significant additional effect of EXT at ages 6 to 10 on alcohol use onset, controlled for EXT at ages 11 to 16 and age 16 sensation seeking. Second, substance use during early adolescence may have mediated or at least contributed to the relationship between FH+ and EXT at ages 11 to 16. Those who have an FH+ might use more alcohol and drugs during adolescence, which in turn could lead to higher EXT scores, rather than FH+ having a direct effect on EXT at ages 11 to 16. Although a partial indirect effect of FH+ on EXT at ages 11 to 16 via substance use cannot be fully ruled out, additional analyses demonstrated that a significant relationship between FH+ and EXT scores was present at 11 and 12 years, prior to the onset of substance use in most of our sample, suggesting the existence of a direct link between FH+ and EXT at ages 11 to 16. Third, it is important to point out that there was a difference in informants of EXT, varying from mother ratings from ages 17m-5y, to teacher ratings during ages 6 to 10, and self-report during adolescence. This could have also contributed to the selective relationship between FH+ and EXT in adolescence despite the moderate correlations between EXT measures and informants across development. Finally, the inclusion of participants was relatively homogeneous and limited by the availability of variables at different ages, which led to a reduced sample and insufficient power for latent growth curve and trajectory analyses. However, the study sample of Francophone and Anglophone individuals from urban settings did not differ from the original sample at age 5 months with respect to the variables of interest, providing confidence that the results should be generalizable to the original sample.
Conclusion
This longitudinal birth cohort study suggests that in our analysis, the strongest predictors of adolescent substance use include proximal EXT during adolescence, concurrent sensation seeking traits, and an FH+ of substance use problems. However, of importance, EXT as young as ages 6 to 10 provide additional predictive power for early alcohol use onset, a key risk factor for chronic alcohol use. These EXT scores at ages 6 to 10 and 11 to 16 were predicted by EXT scores earlier in life (ages 1 to 5). Thus, risk behaviors related to substance use problems emerge early in childhood, emphasizing the importance of early interventions that target these problems. 56,62,63
Supplemental Material
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720982429 for Externalizing Risk Pathways for Adolescent Substance Use and Its Developmental Onset: A Canadian Birth Cohort Study: Trajectoires de comportements extériorisés et le risque pour l’initiation et l’usage de substances des adolescents : Une étude de cohorte de naissance canadienne by Sylvia Maria Leonarda Cox, Natalie Castellanos-Ryan, Sophie Parent, Chawki Benkelfat, Frank Vitaro, Robert O. Pihl, Michel Boivin, Richard E. Tremblay, Marco Leyton and Jean Richard Séguin in The Canadian Journal of Psychiatry
Acknowledgments
The authors wish to thank the Institut de la Statistique du Québec and its partners, and the children and their families for participation in the longitudinal study.
Authors’ Note: Data may be available by completing a request on our website http://gripinfo.ca/grip/public/www/etudes/en/dadprocedures.asp?langue=en. All data requests are subject to current privacy laws guiding their ethical use in Québec, Canada, and examined by the CHU Ste-Justine Research Ethics committee.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research via Grants MOP-44072, MOP-97910, and MOP-133537; the Fonds de Recherche en Santé du Québec via fellowships and Grants 22530, 981055 and 991027; Ministère de l’Éducation, du Loisir et du Sport du Québec (No. 149169); the Social Sciences and Humanities Research Council of Canada via Grants 839-2000-1008 and 410-99-1048; and the Fonds Québécois pour la Recherche sur la Société et la Culture Grants 2002-RS-79238 and 2009-RG-124779. These Funding agencies had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
ORCID iD: Sylvia Maria Leonarda Cox, PhD https://orcid.org/0000-0001-6507-4973
Supplemental Material: The supplemental material for this article is available online.
References
- 1. Johnston LD, O’Malley PM, Miech RA, et al. Monitoring the Future National Survey Results on Drug Use 1975-2015: overview, key findings on adolescent drug use. Ann Harbor (MI): Institute for Social Research, the University of Michigan; 2016. [Google Scholar]
- 2. Moffitt TE, Arseneault L, Belsky D, et al. A gradient of childhood self-control predicts health, wealth, and public safety. Proceed Nat Acad Sci United States of America. 2011;108(7):2693–2698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Edwards AC, Gardner CO, Hickman M, et al. A prospective longitudinal model predicting early adult alcohol problems: evidence for a robust externalizing pathway. Psychol Med. 2016;46(5):957–968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Pingault JB, Cote SM, Galera C, et al. Childhood trajectories of inattention, hyperactivity and oppositional behaviors and prediction of substance abuse/dependence: a 15-year longitudinal population-based study. Mol Psychiatry. 2013;18(7):806–812. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Martel MM, Pierce L, Nigg JT, et al. Temperament pathways to childhood disruptive behavior and adolescent substance abuse: testing a cascade model. J Abnorm Child Psychol. 2009;37(3):363–373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Eiden RD, Lessard J, Colder CR, et al. Developmental cascade model for adolescent substance use from infancy to late adolescence. Dev Psychol. 2016;52(10):1619–1633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Rioux C, Castellanos-Ryan N, Parent S, et al. Age of cannabis use onset and adult drug abuse symptoms: a prospective study of common risk factors and indirect effects. Can J Psychiatry. 2018;63(7):457–464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Englund MM, Egeland B, Oliva EM, et al. Childhood and adolescent predictors of heavy drinking and alcohol use disorders in early adulthood: a longitudinal developmental analysis. Addiction. 2008;103(suppl 1):23–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Maggs JL, Patrick ME, Feinstein L. Childhood and adolescent predictors of alcohol use and problems in adolescence and adulthood in the national child development study. Addiction. 2008;103(suppl 1):7–22. [DOI] [PubMed] [Google Scholar]
- 10. Masse LC, Tremblay RE. Behavior of boys in kindergarten and the onset of substance use during adolescence. Arch General Psychiatry. 1997;54(1):62–68. [DOI] [PubMed] [Google Scholar]
- 11. Pitkanen T, Kokko K, Lyyra AL, et al. A developmental approach to alcohol drinking behaviour in adulthood: a follow-up study from age 8 to age 42. Addiction. 2008;103(suppl 1):48–68. [DOI] [PubMed] [Google Scholar]
- 12. Brook JS, Lee JY, Brown EN, et al. Developmental trajectories of marijuana use from adolescence to adulthood: personality and social role outcomes. Psychol Rep. 2011;108(2):339–357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Chassin L, Fora DB, King KM. Trajectories of alcohol and drug use and dependence from adolescence to adulthood: the effects of familial alcoholism and personality. J Abnorm Psychol. 2004;113(4):483–498. [DOI] [PubMed] [Google Scholar]
- 14. Stephenson M, Barr P, Ksinan A, et al. Which adolescent factors predict alcohol misuse in young adulthood? A co-twin comparisons study. Addiction. 2019;115(5):877–887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Dick DM, Aliev F, Latendresse SJ, et al. Adolescent alcohol use is predicted by childhood temperament factors before age 5, with mediation through personality and peers. Alcohol, Clin Exper Res. 2013;37(12):2108–2117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Hicks BM, Foster KT, Iacono WG, et al. Genetic and environmental influences on the familial transmission of externalizing disorders in adoptive and twin offspring. JAMA Psychiatry. 2013;70(10):1076–1083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Kendler KS, Sundquist K, Ohlsson H, et al. Genetic and familial environmental influences on the risk for drug abuse: a national Swedish adoption study. Arch Gen Psychiatry. 2012;69(7):690–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Castellanos-Ryan N, Conrod PJ. Personality correlates of the common and unique variance across conduct disorder and substance misuse symptoms in adolescence. J Abnorm Child Psychol. 2011;39(4):563–576. [DOI] [PubMed] [Google Scholar]
- 19. Cordova D, Heinze J, Mistry R, et al. Family functioning and parent support trajectories and substance use and misuse among minority urban adolescents: a latent class growth analysis. Subst Use Misuse. 2014;49(14):1908–1919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. McLaughlin KA, Breslau J, Green JG, et al. Childhood socio-economic status and the onset, persistence, and severity of DSM-IV mental disorders in a US national sample. Soc Sci Med. 2011;73(7):1088–1096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Castellanos-Ryan N, Struve M, Whelan R, et al. Neural and cognitive correlates of the common and specific variance across externalizing problems in young adolescence. Am J Psychiatry. 2014;171(12):1310–1319. [DOI] [PubMed] [Google Scholar]
- 22. Woicik PA, Stewart SH, Pihl RO, et al. The substance use risk profile scale: a scale measuring traits linked to reinforcement-specific substance use profiles. Add Behav. 2009;34(12):1042–1055. [DOI] [PubMed] [Google Scholar]
- 23. Kendler KS, Gardner CO, Edwards AC, et al. Childhood risk factors for heavy episodic alcohol use and alcohol problems in late adolescence: a marginal structural model analysis. J Stud Alcohol Drugs. 2018;79(3):370–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Kendler KS, Gardner CO, Edwards A, et al. Dimensions of parental alcohol use/problems and offspring temperament, externalizing behaviors, and alcohol use/problems. Alcohol, Clin Exper Res. 2013;37(12):2118–2127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Minnes S, Min MO, Kim JY, et al. The association of prenatal cocaine exposure, externalizing behavior and adolescent substance use. Drug Alcohol Depend. 2017;176:33–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Green JG, McLaughlin KA, Berglund PA, et al. Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: associations with first onset of DSM-IV disorders. Arch Gen Psychiatry. 2010;67(2):113–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Hussong AM, Jones DJ, Stein GL, et al. An internalizing pathway to alcohol use and disorder. Psychol Addict Behav. 2011;25(3):390–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Afzali MH, Stewart SH, Seguin JR, et al. The network constellation of personality and substance use: evolution from early to late adolescence. Eur J Pers. 2020. [Google Scholar]
- 29. Foster KT, Hicks BM, Zucker RA. Positive and negative effects of internalizing on alcohol use problems from childhood to young adulthood: the mediating and suppressing role of externalizing. J Abnorm Psychol. 2018;127(4):394–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Bergen SE, Gardner CO, Kendler KS. Age-related changes in heritability of behavioral phenotypes over adolescence and young adulthood: a meta-analysis. Twin Res Human. 2007;10(3):423–433. [DOI] [PubMed] [Google Scholar]
- 31. Vrieze SI, Hicks BM, Iacono WG, et al. Decline in genetic influence on the co-occurrence of alcohol, marijuana, and nicotine dependence symptoms from age 14 to 29. Am J Psychiatry. 2012;169(10):1073–1081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Jones DJ, Lewis T, Litrownik A, et al. Linking childhood sexual abuse and early adolescent risk behavior: the intervening role of internalizing and externalizing problems. J Abnorm Child Psychol. 2013;41(1):139–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Castellanos-Ryan N, O’Leary-Barrett M, Sully L, et al. Sensitivity and specificity of a brief personality screening instrument in predicting future substance use, emotional, and behavioral problems: 18-month predictive validity of the substance use risk profile scale. Alcohol, Clin Exper Res. 2013;37(suppl 1):E281–290. [DOI] [PubMed] [Google Scholar]
- 34. Castellanos-Ryan N, Rubia K, Conrod PJ. Response inhibition and reward response bias mediate the predictive relationships between impulsivity and sensation seeking and common and unique variance in conduct disorder and substance misuse. Alcohol, Clin Exper Res. 2011;35(1):140–155. [DOI] [PubMed] [Google Scholar]
- 35. Crews FT, Boettiger CA. Impulsivity, frontal lobes and risk for addiction. Pharmacol Biochem Behav. 2009;93(3):237–247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Wichers M, Gardner C, Maes HH, et al. Genetic innovation and stability in externalizing problem behavior across development: a multi-informant twin study. Behav Genetics. 2013;43(3):191–201. [DOI] [PubMed] [Google Scholar]
- 37. Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: results from the national longitudinal alcohol epidemiologic survey. J Substance Abuse. 1997;9:103–110. [DOI] [PubMed] [Google Scholar]
- 38. Grant BF, Dawson DA. Age of onset of drug use and its association with DSM-IV drug abuse and dependence: results from the national longitudinal alcohol epidemiologic survey. J Substance Abuse. 1998;10(2):163–173. [DOI] [PubMed] [Google Scholar]
- 39. Merikangas KR, Stolar M, Stevens DE, et al. Familial transmission of substance use disorders. Arch General Psychiatry. 1998;55(11):973–979. [DOI] [PubMed] [Google Scholar]
- 40. Hicks BM, Krueger RF, Iacono WG, et al. Family transmission and heritability of externalizing disorders: a twin-family study. Arch General Psychiatry. 2004;61(9):922–928. [DOI] [PubMed] [Google Scholar]
- 41. Acheson A, Vincent AS, Cohoon AJ, et al. Defining the phenotype of young adults with family histories of alcohol and other substance use disorders: studies from the family health patterns project. Add Behav. 2018;77:247–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Jetté M, Desrosiers H, Tremblay RE. “In 2001…I’ll be 5 years old”. Survey of 5 months old infants: preliminary report from the Québec longitudinal study of childhood development (QLSCD). Ministère de la Santé et des Services Sociaux. Gouvernement du Québec, Montreal, Quebec, Canada 1998. [Google Scholar]
- 43. Behar L, Stringfield S. A behavior rating scale for the preschool child. Dev Psychol. 1974;10(5):601–610. [Google Scholar]
- 44. Tremblay RE, Vitaro F, Gagnon C, et al. A prosocial scale for the preschool behaviour questionnaire: concurrent and predictive correlates. Int J Behav Develop. 1992;15(2):227–245. [Google Scholar]
- 45. Papageorgiou V, Kalyva E, Dafoulis V, et al. Differences in parents’ and teachers’ ratings of ADHD symptoms and other mental health problems. Eur J Psychiat 2008;22(4):200–210. [Google Scholar]
- 46. Clark DB, Winters KC. Measuring risks and outcomes in substance use disorders prevention research. J Consult Clin Psychol. 2002;70(6):1207–1223. [DOI] [PubMed] [Google Scholar]
- 47. Castonguay-Jolin L, Perrier-Menard E, Castellanos-Ryan N, et al. SURPS French version validation in a Quebec adolescent population. Can J Psychiatry. 2013;58(9):538–545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Krank M, Stewart SH, O’Connor R, et al. Structural, concurrent, and predictive validity of the substance use risk profile scale in early adolescence. Add Behav. 2011;36(1-2):37–46. [DOI] [PubMed] [Google Scholar]
- 49. Huijbregts SC, Séguin JR, Zoccolillo M, et al. Associations of maternal prenatal smoking with early childhood physical aggression, hyperactivity-impulsivity, and their co-occurrence. J Abnorm Child Psychol. 2007;35(2):203–215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Epstein NB, Baldwin LM, Bishop DS. The McMaster family assessment device. J Marital Family Ther. 1983;9(2):171–180. [Google Scholar]
- 51. Byles J, Byrne C, Boyle MH, et al. Ontario child health study: reliability and validity of the general functioning subscale of the McMaster family assessment device. Family Process. 1988;27(1):97–104. [DOI] [PubMed] [Google Scholar]
- 52. Charles NE, Ryan SR, Acheson A, et al. Childhood stress exposure among preadolescents with and without family histories of substance use disorders. Psychol Addict Behav. 2015;29(1):192–200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Tofighi D, MacKinnon DP. RMediation: an R package for mediation analysis confidence intervals. Behav Res Methods. 2011;43(3):692–700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. MacKinnon DP, Fairchild AJ, Fritz MS. Mediation analysis. Annu Rev Psychol. 2007;58:593–614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. MacKinnon DP, Lockwood CM, Hoffman JM, et al. A comparison of methods to test mediation and other intervening variable effects. Psychol Method. 2002;7(1):83–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Castellanos-Ryan N, Séguin JR, Vitaro F, et al. Impact of a 2-year multimodal intervention for disruptive 6-year-olds on substance use in adolescence: randomised controlled trial. Br J Psychiatry. 2013;203(3):188–195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Zohsel K, Baldus C, Schmidt MH, et al. Predicting later problematic cannabis use from psychopathological symptoms during childhood and adolescence: results of a 25-year longitudinal study. Drug Alcohol Depend. 2016;163:251–255. [DOI] [PubMed] [Google Scholar]
- 58. Ystrom E, Kendler KS, Reichborn-Kjennerud T. Early age of alcohol initiation is not the cause of alcohol use disorders in adulthood, but is a major indicator of genetic risk. A population-based twin study. Addiction. 2014;109(11):1824–1832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Coté SM, Vaillancourt T, Barker ED, et al. The joint development of physical and indirect aggression: predictors of continuity and change during childhood. Develop Psychopathol. 2007;19(1):37–55. [DOI] [PubMed] [Google Scholar]
- 60. Tremblay RE. Developmental origins of disruptive behaviour problems: the “original sin” hypothesis, epigenetics and their consequences for prevention. J Child Psychol Psychiatry, Allied Disciplines. 2010;51(4):341–367. [DOI] [PubMed] [Google Scholar]
- 61. Castellanos-Ryan N, Parent S, Vitaro F, et al. Pubertal development, personality, and substance use: a 10-year longitudinal study from childhood to adolescence. Journal of Abnorm Psychol. 2013;122(3):782–796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Conrod PJ, Castellanos-Ryan N, Mackie C. Long-term effects of a personality-targeted intervention to reduce alcohol use in adolescents. J Consult Clin Psychol. 2011;79(3):296–306. [DOI] [PubMed] [Google Scholar]
- 63. Edalati H, Conrod PJ. A review of personality-targeted interventions for prevention of substance misuse and related harm in community samples of adolescents. Front Psychiatry. 2018;9:770. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Material, sj-docx-1-cpa-10.1177_0706743720982429 for Externalizing Risk Pathways for Adolescent Substance Use and Its Developmental Onset: A Canadian Birth Cohort Study: Trajectoires de comportements extériorisés et le risque pour l’initiation et l’usage de substances des adolescents : Une étude de cohorte de naissance canadienne by Sylvia Maria Leonarda Cox, Natalie Castellanos-Ryan, Sophie Parent, Chawki Benkelfat, Frank Vitaro, Robert O. Pihl, Michel Boivin, Richard E. Tremblay, Marco Leyton and Jean Richard Séguin in The Canadian Journal of Psychiatry