

Key Points
Question
Is the use of intercostal nerve block (ICNB) analgesia safe and beneficial for adults undergoing thoracic surgery?
Findings
In this systematic review and meta-analysis of 66 studies including 5184 adult patients undergoing thoracic surgery, the use of ICNB was associated with a clinically and statistically relevant analgesic benefit during the first 24 hours after thoracic surgery, with outcomes that were superior to systemic analgesia and noninferior to other techniques. Although ICNB was associated with a reduction in postoperative opioid consumption, the extent of this reduction was inferior to that of thoracic epidural and paravertebral block analgesia.
Meaning
This study found that ICNB was safe and beneficial for adults undergoing thoracic surgery, providing a reduction in pain during the first 24 hours after thoracic surgery; ICNB may be most beneficial for cases in which thoracic epidural or paravertebral block analgesia are not indicated.
Abstract
Importance
The use of intercostal nerve block (ICNB) analgesia with local anesthesia is common in thoracic surgery. However, the benefits and safety of ICNB among adult patients undergoing surgery is unknown.
Objective
To evaluate the analgesic benefits and safety of ICNB among adults undergoing thoracic surgery.
Data Sources
A systematic search was performed in Ovid MEDLINE, Ovid Embase, Scopus, and the Cochrane Library databases using terms for ICNB and thoracic surgery (including thoracic surgery, thoracoscopy, thoracotomy, nerve block, intercostal nerves). The search and results were not limited by date, with the last search conducted on July 24, 2020.
Study Selection
Selected studies were experimental or observational and included adult patients undergoing cardiothoracic surgery in which ICNB was administered with local anesthesia via single injection, continuous infusion, or a combination of both techniques in at least 1 group of patients. For comparison with ICNB, studies that examined systemic analgesia and different forms of regional analgesia (such as thoracic epidural analgesia [TEA], paravertebral block [PVB], and other techniques) were included. These criteria were applied independently by 2 authors, and discrepancies were resolved by consensus. A total of 694 records were selected for screening.
Data Extraction and Synthesis
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline. Data including patient characteristics, type of surgery, intervention analgesia, comparison analgesia, and primary and secondary outcomes were extracted independently by 3 authors. Synthesis was performed using a fixed-effects model.
Main Outcomes and Measures
The coprimary outcomes were postoperative pain intensity (measured as the worst static or dynamic pain using a validated 10-point scale, with 0 indicating no pain and 10 indicating severe pain) and opioid consumption (measured in morphine milligram equivalents [MMEs]) at prespecified intervals (0-6 hours, 7-24 hours, 25-48 hours, 49-72 hours, and >72 hours). Clinically relevant analgesia was defined as a 1-point or greater difference in pain intensity score at any interval. Secondary outcomes included 30-day postoperative complications and pulmonary function.
Results
Of 694 records screened, 608 were excluded based on prespecified exclusion criteria. The remaining 86 full-text articles were assessed for eligibility, and 20 of those articles were excluded. All of the 66 remaining studies (5184 patients; mean [SD] age, 53.9 [10.2] years; approximately 59% men and 41% women) were included in the qualitative analysis, and 59 studies (3325 patients) that provided data for at least 1 outcome were included in the quantitative meta-analysis. Experimental studies had a high risk of bias in multiple domains, including allocation concealment, blinding of participants and personnel, and blinding of outcome assessors. Marked differences (eg, crossover studies, timing of the intervention [intraoperative vs postoperative], blinding, and type of control group) were observed in the design and implementation of studies. The use of ICNB vs systemic analgesia was associated with lower static pain (0-6 hours after surgery: mean score difference, −1.40 points [95% CI, −1.46 to −1.33 points]; 7-24 hours after surgery: mean score difference, −1.27 points [95% CI, −1.40 to −1.13 points]) and lower dynamic pain (0-6 hours after surgery: mean score difference, −1.66 points [95% CI, −1.90 to −1.41 points]; 7-24 hours after surgery: mean score difference, −1.43 points [95% CI, −1.70 to −1.17 points]). Intercostal nerve block analgesia was noninferior to TEA (mean score difference in worst dynamic panic at 7-24 hours after surgery: 0.79 points; 95% CI, 0.28-1.29 points) and marginally inferior to PVB (mean score difference in worst dynamic pain at 7-24 hours after surgery: 1.29 points; 95% CI, 1.16 to 1.41 points). The largest opioid-sparing effect of ICNB vs systemic analgesia occurred at 48 hours after surgery (mean difference, −10.97 MMEs; 95% CI, −12.92 to −9.02 MMEs). The use of ICNB was associated with higher MME values compared with TEA (eg, 48 hours after surgery: mean difference, 48.31 MMEs; 95% CI, 36.11-60.52 MMEs) and PVB (eg, 48 hours after surgery: mean difference, 3.87 MMEs; 95% CI, 2.59-5.15 MMEs).
Conclusions and Relevance
In this study, single-injection ICNB was associated with a reduction in pain during the first 24 hours after thoracic surgery and was clinically noninferior to TEA or PVB. Intercostal nerve block analgesia had opioid-sparing effects; however, TEA and PVB were associated with larger decreases in postoperative MMEs, suggesting that ICNB may be most beneficial for cases in which TEA and PVB are not indicated.
This systematic review and meta-analysis assesses the benefits and safety associated with intercostal nerve block analgesia compared with systemic analgesia and other local analgesia techniques among adults undergoing thoracic surgery.
Introduction
Acute pain after thoracic surgery is common and severe, and can lead to increased morbidity.1,2 In the thorax, nociception travels primarily via the intercostal nerves.3 Therefore, blockade of the intercostal nerve is used to provide analgesia after thoracic surgery.4 Intercostal nerve blocks (ICNBs) are a common component of multimodal analgesia for thoracic surgery.5 Current guidelines suggest that continuous intercostal analgesia is similar to thoracic epidural analgesia (TEA).6 Aside from consideration of technical aspects and costs,7 the selection of any analgesic approach is typically based on its clinical benefits and disadvantages.8,9
In recent years, the use of minimally invasive techniques in thoracic surgery has substantially increased.10 This increase coincided with a decrease in the use of TEA and the emergence of fascial plane blocks.4 Previous reviews have found that ICNB was superior to systemic analgesia and was associated with reductions in opioid consumption.11,12 However, although Joshi et al12 recommended TEA and paravertebral block (PVB) as first-line options, Detterbeck et al11 questioned the superiority of TEA vs continuous extrapleural techniques. Considering the findings of these previous studies,4,10,11,12 we conducted a systematic review and meta-analysis to synthesize the evidence on the benefits and safety of ICNB among adult patients undergoing thoracic surgery.
We hypothesized that the use of ICNB would be associated with superior analgesia and reductions in opioid consumption compared with systemic analgesia alone, while being inferior to PVB and TEA. We also expected ICNB to be superior to systemic analgesia but inferior to PVB or TEA with regard to postoperative complications.
Methods
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guideline.13 The protocol was registered in the PROSPERO database (registration number: CRD42021224783).
Selected sources included observational and experimental studies of adults 18 years and older undergoing any cardiothoracic surgery in which ICNB with local anesthesia was administered via single injection, continuous infusion, or a combination of both techniques in at least 1 group of patients. The use of ICNB was separately compared with both systemic analgesia and different forms of regional analgesia, including TEA and PVB. The coprimary outcomes were acute postoperative pain intensity (dynamic and static) before hospital discharge and opioid consumption. The secondary outcomes were pulmonary function and 30-day postoperative complications.
A systematic literature search was constructed by a medical librarian (R.S.H.). Ovid MEDLINE, Ovid Embase, Scopus, and the Cochrane Library databases were queried using the following natural language and controlled vocabulary terms for ICNB and thoracic surgery: thoracic surgery, thoracic surgical procedures (including cardiac surgical procedures, mediastinoscopy, pulmonary surgical procedures, sternotomy, thoracoplasty, thoracoscopy, thoracostomy, thoracotomy, thymectomy, tracheostomy, tracheotomy, cardiac, heart, pulmonary, and lung), and ICNB-related terms (including nerve block, intercostal nerves, ICNB, nerve, and block). Records included were limited to human studies published in the English language. A sample electronic search is available on the PROSPERO website.14 Case reports, conference abstracts, editorial letters, and pediatric-only studies were excluded. Identification of other unpublished studies was not attempted. The search and results were not limited by date. After deduplication, 694 unique records were identified. The last date of search was July 24, 2020.
Only articles with available full text were included. Records were screened independently by 2 authors (C.E.G.-L. and J.P.C.) based on title and abstract. Discrepancies were resolved by consensus. The 2 authors then obtained full text of the remaining articles to assess eligibility.
Data Collection Process
Three authors (C.E.G.-L., A.P., and J.P.C.) extracted the data independently using Excel spreadsheets (Microsoft Corp) that were subsequently merged after the data were collected. Attempts were made to contact authors for missing data. The following data were extracted: demographic characteristics of participants (age, sex, and body mass index), type of surgery (sternotomy, thoracoscopy, thoracotomy, and not specified), type of intervention (single-injection, continuous administration, dose administered, and type of local anesthetic used), and comparator groups (eg, placebo, systemic analgesia, TEA, PVB, and erector spinae plane block). Pain was extracted as the worst static or dynamic pain on a validated 10-point scale (verbal, numerical, or visual, with 0 indicating no pain and 10 indicating severe pain) within the following postoperative periods: 0 to 6 hours, 7 to 24 hours, 25 to 48 hours, 49 to 72 hours, and more than 72 hours. Clinically relevant analgesia was defined as a 1-point or greater difference in pain intensity score at any interval.15 Opioid consumption was extracted for the same intervals and converted to intravenous morphine milligram equivalents (MMEs).
Nominal data were summarized using proportions, whereas continuous data were reported as means with SDs. Data provided as medians and ranges were converted to means and SDs according to the methods described in Hozo et al.16 Data from figures were digitized using WebPlotDigitizer software, version 4.4 (Ankit Rohatgi).17 Risk of bias in individual studies was assessed according to the criteria described by the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) Working Group18 and was considered for each outcome.
Statistical Analysis
To provide estimates of intervention outcomes, a quantitative fixed-effects meta-analysis was performed using the meta package in R software, version 3.6.3 (R Foundation for Statistical Computing), when data from at least 3 studies were available for each outcome. Summary estimates, including odds ratios (ORs), mean differences, and 95% CIs, were calculated for each outcome. Heterogeneity was assessed using the I2 statistic and, when serious heterogeneity was detected, subgroups were investigated to identify potential differences. Qualitative analysis was followed by quantitative analysis using the GRADE criteria to rate the quality of evidence.19 Results were interpreted in the context of pooled effect estimates; risk of bias, heterogeneity (measured using the I2 statistic), imprecision, and indirectness were assessed for each outcome across the respective informing studies. Publication bias was determined by inspection of funnel plots for each outcome. Synthesis results, including information on the quality of evidence, are shown in Table 1.
Table 1. Summary of Studies Comparing ICNB Analgesia With Other Regional or Systemic Analgesia Techniques.
| Source | Type of study | Blinding, yes/no (type of blinding) | Type of surgery | ICNB analgesia (No. of patients) | Comparison analgesia (No. of patients) | Prespecified outcomes | Postoperative follow-up period |
|---|---|---|---|---|---|---|---|
| de la Rocha and Chambers,20 1984 | RCT | No | Thoracotomy | Single injection (5) | Continuous (5); no block (5); TENS (5) | Spirometry | 5 d |
| Orr et al,21 1981 | RCT | No | Thoracotomy | Single injection (30) | Cryoanalgesia (15) | Pain intensity (VAS); opioid consumption; hemodynamic parameters | ≤8 d |
| Perttunen et al,22 1995 | RCT | No | Thoracotomy | Single injection (15) | Epidural (15); PVB (15) | Pain intensity (VAS and NRS); area of analgesic spread; spirometry; complications; blood-gas analysis; LOS; bupivacaine levels | 2 d |
| Fiorelli et al,23 2020 | RCT | Yes (SB) | Thoracotomy | Single injection (30) | ESPB (30) | Pain intensity (NRS); opioid consumption; spirometry; patient satisfaction | 2 d |
| Shafei et al,24 1990 | RCT | No | Thoracotomy | Single injection (16) | Cryoanalgesia (31); interpleural (16) | Pain intensity (VAS); opioid consumption; complications | 7 d |
| Bergh et al,25 1966 | Prospective | No | Thoracotomy | Single injection (30) | No block (6) | Pain sensitivity; opioid consumption; spirometry; blood-gas analysisa | 7 d |
| Bolotin et al,26 2000 | RCT | No | Thoracoscopy | Single injection (16) | No block (16) | Pain intensity; hemodynamic parameters; opioid consumptionb | 1.5 h |
| Dryden et al,27 1993 | Randomized crossover | Yes (DB) | Thoracotomy | Continuous (10) | No block (10) | Pain intensity (VAS); opioid consumption; complications | 2 d |
| Chan et al,28 1991 | RCT | Yes (DB) | Thoracotomy | Continuous (10) | No block (10) | Pain intensity (VAS); opioid consumption; spirometry; bupivacaine levels | 24 h |
| Toledo-Pereyra and DeMeester,29 1979 | RCT | No | Thoracotomy | Single injection (10) | No block (10) | Opioid consumption; spirometry | 10 d |
| Liu et al,30 1995 | RCT | Yes (DB) | Thoracotomy | Single injection (9) | No block (11) | Pain intensity (VAS); opioid consumption; spirometry; complications | 3 d |
| Kavanagh et al,31 1994 | RCT | Yes (DB) | Not specified | Single injection (15) | No block (15) | Pain intensity (VAS); pain sensitivity; opioid consumption; spirometry; blood-gas analysisa | 3 d |
| Zhan et al,32 2017 | RCT | No | Thoracotomy | Single injection (15) | No block (15) | Pain intensity (VAS); stress biomarkers; complications; LOS | 24 h |
| Joucken et al,33 1987 | RCT | Yes (DB) | Thoracotomy | Single injection (15) | Cryoanalgesia (15); no block (15) | Opioid consumption; blood-gas analysis | 1.5 d |
| Faust and Nauss,34 1976 | RCT | No | Thoracotomy | Single injection (17) | No block (17) | Blood-gas analysis; spirometry | 45 min |
| Dowling et al,35 2003 | RCT | Yes (DB) | Sternotomy | Continuous (16) | No block (19) | Pain intensity (VAS); opioid consumption; spirometry; LOS; complications | 2 d |
| Delilkan et al,36 1973 | Prospective | Yes (DB) | Thoracotomy | Single injection (20) | No block (20) | Opioid consumption; spirometry; physiologic and blood-gas analysis; clinical condition | 24 h |
| Baxter et al,37 1987 | RCT | Yes (SB) | Sternotomy | Continuous (20) | No block (20) | Pain intensity; opioid consumption; spirometry; blood-gas analysis; complicationsb | 5 d |
| Carretta et al,38 1996 | RCT | No | Thoracotomy | Continuous (10) | No block (20) | Pain intensity (VAS); opioid consumption; spirometry; blood-gas analysisb | 2 d |
| Ghafouri et al,39 2008 | RCT | No | Thoracotomy | Single injection (25) | No block (25) | Pain intensity; opioid consumption; spirometryb | 3 d |
| Kolvenbach et al,40 1989 | Prospective | No | Thoracotomy | Continuous (25) | No block (30) | Complications; mortality; bupivacaine levels; patient satisfaction | In-hospital stay |
| Ahmed et al,41 2017 | RCT | Yes (DB) | Thoracoscopy | Single injection (30) | No block (30) | Pain intensity (VAS); opioid consumption | 24 h |
| Barr et al,42 2007 | RCT | Yes (DB) | Sternotomy | Single injection (41) | No block (40) | Pain intensity (VAS and NRS); opioid consumption; complicationsb | 25 h |
| Lee et al,43 2019 | RCT | Yes (DB) | Sternotomy | Single injection (38) | No block (41) | Pain intensity; opioid consumption; LOS; complicationsb | 3 d |
| Zhu et al,44 2018 | RCT | No | Thoracotomy | Single injection (40) | No block (41) | Pain intensity (VAS); opioid consumption; hemodynamic parameters; complications. | 48 h |
| Galway et al,45 1975 | RCT | Yes (DB) | Thoracotomy | Single injection (46) | No block (46) | Pain intensity; opioid consumption; hemodynamic parameters; complicationsb | 24 h |
| Wang et al,46 2019 | RCT | No | Thoracotomy | Single injection (50) | No block (50) | Pain intensity (VAS); cognitive function; inflammatory biomarkers | 24 h |
| Kaplan et al,47 1975 | Prospective | No | Thoracotomy | Single injection (12) | No block (6) | Pain intensity; opioid requirement; spirometry; complications; duration of block; blood-gas analysis; complicationsb | 3 d |
| D’Andrilli et al,48 2006 | RCT | No | Thoracotomy | Single injection (60) | No block (60) | Pain intensity (VAS); patient satisfaction; LOS; complications | In-hospital stay, d |
| Mozell et al,49 1991 | RCT | Yes (DB) | Thoracotomy | Continuous (8) | No block (8) | Pain intensity (VAS); opioid consumption; spirometry | 5 d |
| Yang et al,50 2019 | Retrospective | NA | Thoracoscopy | Single injection (14) | PVB (14) | Pain (VAS); blood-gas analysis; anesthetic requirement | 1 h |
| Xia et al,51 2020 | Retrospective | NA | Thoracoscopy | Single injection (20) | PVB (20) | Pain (VAS); opioid consumption; blood-gas analysis; complications | 2 d |
| Hutchins et al,52 2017 | RCT | No | Thoracoscopy | Single injection (25) | PVB (23) | Pain intensity (NRS); opioid consumption; LOS; patient satisfaction; complications | 2 d |
| Chen et al,53 2020 | RCT | Yes (DB) | Thoracoscopy | Single injection (24) | ESPB (24); PVB (24) | Pain intensity (VAS); opioid consumption; complications | 2 d |
| Kadomatsu et al,54 2018 | RCT | No | Thoracoscopy | Continuous (24) | PVB (26) | Pain intensity (VAS); complications | 2 d |
| Matyal et al,55 2015 | Prospective | No | Thoracoscopy | Single injection (20) | PVB (30) | Pain intensity (VAS); opioid consumption; spirometry; LOS | 2 mo |
| Wu et al,56 2018 | RCT | Yes (SB) | Thoracoscopy | Single injection (32) | PVB (34) | Pain intensity (VAS); opioid consumption; time to ambulation; complications | 2 d |
| Mogahed and Elkahwagy,57 2020 | RCT | No | Thoracoscopy | Single injection (35) | No block (35); PVB (35) | Pain intensity (VAS); spirometry blood-gas analysis; hemodynamic parameters; duration of recovery from anesthesia | 2 h |
| Xiang et al,58 2020 | RCT | No | Thoracoscopy | Single injection (40) | No block (40); PVB (40) | Pain intensity (NRS); hemodynamic parameters; blood-gas analysis; procedural cost; patient satisfaction; LOS; complications | 24 h |
| Zheng et al,59 2020 | RCT | No | Thoracoscopy | Single injection (50) | PVB (50) | Surgical visualization; duration of the technique; complications | Surgery |
| Oksuz et al,60 2018 | Retrospective | NA | Thoracotomy | Single injection (22) | SAPB (20) | Pain (VAS); opioid consumption; complications | 24 h |
| Kim et al,61 2021 | RCT | No | Thoracoscopy | Single injection (25) | SAPB (25) | Pain intensity (NRS); opioid consumption | 1-2 d (until chest tube removal) |
| Hsieh et al,62 2016 | Retrospective | NA | Thoracoscopy | Continuous (39) | Single injection (39) | Pain intensity (VAS and NRS); opioid consumption; pulmonary function; LOS | In-hospital stay |
| Wu et al,63 2016 | Retrospective | NA | Thoracoscopy | Continuous (50) | Single injection (50) | Pain (NRS and VAS); opioid consumption; LOS | In-hospital stay |
| Bachmann-Mennenga et al,64 1993 | RCT | No | Thoracotomy | Single injection (10) | Interpleural (10); no block (10); TEA (10) | Pain intensity; hemodynamic parameters; stress biomarkers; blood-gas analysis; bupivacaine levelsb | 6 h |
| Concha et al,65 2004 | RCT | No | Thoracotomy | Single injection (16) | TEA (15) | Pain intensity (VAS); opioid consumption, spirometry | 2 d |
| Kaiser et al,66 1998 | RCT | No | Thoracotomy | Continuous (15) | TEA (15) | Pain intensity; opioid consumption; spirometry; mortality; complications; bupivacaine levelsb | 5 d |
| Wurnig et al,67 2002 | RCT | No | Thoracotomy | Single injection (15) | TEA (15) | Pain intensity (VAS); opioid consumption; procedural cost; complications | 6 d |
| Scheinin et al,68 1987 | RCT | No | Thoracotomy | Single injection (10) | Preincisional single injection (11); TEA (18) | Pain intensity (VAS); opioid consumption; blood-gas analysis; spirometry; stress biomarkers; bupivacaine levels | 24 h |
| Pompeo et al,69 2013 | Prospective | No | Thoracoscopy | Single injection (10) | TEA (20) | Pain intensity (VAS); technique feasibility; blood-gas analysis; hemodynamic parameters; procedural costs | In-hospital stay |
| Takamori et al,70 2002 | RCT | No | Thoracotomy | Single injection + TEA (20) | TEA (20) | Pain intensity (VAS); analgesic consumption; food intake; stress biomarkersb | 5 d |
| Ueda et al,71 2020 | RCT | No | Thoracoscopy | Single injection (21) | TEA (22) | Pain intensity (VAS); spirometry; 6-min walking distance; duration of technique; opioid consumption; complications | 7 d |
| Mehran et al,72 2017 | Retrospective | NA | Thoracoscopy and Thoracotomy | Single injection (247) | TEA (247) | Complications; LOS; mortality | In-hospital stay |
| Debreceni et al,73 2003 | RCT | Yes (DB) | Thoracotomy | Continuous (22) | TEA (25) | Pain intensity (VAS); opioid consumption; blood-gas analysis; hemodynamic parameters; spirometry | 20 h |
| Vilvanathan et al,74 2020 | RCT | No | Thoracotomy | Single injection (25) | TEA (25) | Pain intensity (NRS); motor blockade scale; opioid consumption; complications | 24 h |
| Chen et al,75 2018 | Retrospective | NA | Thoracoscopy | Single injection (135) | No block (772); TEA (255) | LOS; postoperative cough | 12 mo |
| Ranganathan et al,76 2020 | RCT | Yes (DB) | Thoracotomy | Single injection plus TEA (29) | TEA (30) | Pain intensity (NRS); opioid consumption; spirometry | 24 h |
| Sagiroglu et al,77 2013 | RCT | Yes (DB) | Thoracotomy | Continuous (30) | TEA (30) | Pain intensity (VAS); opioid consumption; hemodynamic parameters; complications | 24 h |
| Asantila et al,78 1986 | RCT | No | Thoracotomy | Single injection (10) | Repeated single injection (10); TEA (31) | Pain intensity (VAS); opioid consumption; blood-gas analysis; spirometry | 24 h |
| Khalil et al,79 2015 | Retrospective | NA | Thoracotomy | Single injection (53) | TEA (32) | Pain (VAS); opioid consumption; LOS; complications | 3 d |
| Dauphin et al,80 1997 | RCT | No | Thoracotomy | Continuous (31) | TEA (41) | Pain intensity (VAS); opioid consumption; bupivacaine levels | 3 d |
| Meierhenrich et al,81 2011 | RCT | No | Thoracotomy | Single injection (42) | TEA (41) | Pain intensity; opioid consumption; spirometry; LOS; complications | In-hospital stay |
| Luketich et al,82 2005 | RCT | No | Thoracotomy | Continuous (47) | TEA (44) | Pain intensity (VAS); opioid consumption; spirometry; technique success rate; LOSb | 6 d |
| Rice et al,83 2015 | Retrospective | NA | Thoracoscopy and Thoracotomy | Single injection (54) | TEA (54) | Pain (NRS); opioid consumption; complications | In-hospital stay |
| Hung et al,84 2015 | Retrospective | NA | Thoracoscopy | Single injection (108) | TEA (130) | Pain (VAS); mortality; conversion to intubation; complications; LOS; duration of anesthesia/surgery; blood-gas analysis; intraoperative hemodynamic parameters | In-hospital stay |
| Ambrogi et al,85 2014 | Retrospective | NA | Thoracoscopy | Single injection (20) | TEA (20) | Pain intensity (VAS); conversion to general anesthesia; spirometry; blood-gas analysis; hemodynamic parameters; complications | In-hospital stay |
Abbreviations: DB, double-blind; ESPB, erector spinae plane block; ICNB, intercostal nerve block; LOS, length of stay; NA, not applicable; NRS, numeric rating scale; PVB, paravertebral block; RCT, randomized clinical trial; SAPB, serratus anterior plane block; SB, single-blind; TEA, thoracic epidural analgesia; TENS, transcutaneous electrical nerve stimulation; VAS, visual analog scale.
Tactile pain thresholds.
Includes the use of a scale other than NRS or VAS.
To synthesize data, the Cochrane criteria86 were used for randomized clinical trials, and the GRADE criteria19 were used for nonrandomized and observational studies. To evaluate the quality of the body of evidence for each individual outcome according to GRADE criteria, the seriousness of risk was assessed across all informing studies to grade the certainty of evidence for each effect estimate.18
Results
Study Selection
Of 694 records screened, 608 were excluded based on the prespecified exclusion criteria discussed in Methods (Figure 1). The remaining 86 full-text articles were assessed for eligibility, and 20 of those articles were excluded (5 were not written in the English language, 4 included interventions that were mislabeled as ICNB, 3 did not include a group of patients who received ICNB with local anesthesia, 3 were systematic reviews, 2 were editorials or short reports, 1 examined outcomes outside the scope of the present study, 1 had insufficient reporting, and 1 examined nonthoracic surgery). All of the remaining 66 studies20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85 (5184 patients; mean [SD] age, 53.9 [10.2] years; approximately 59% men and 41% women) were included in the qualitative analysis; of those, 59 studies20,22,25,26,28,29,30,31,32,33,34,36,37,38,39,40,41,42,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,65,66,67,68,69,71,72,73,74,77,78,79,80,81,83,84 (3325 patients) that provided data for at least 1 outcome were included in the quantitative meta-analysis.
Figure 1. PRISMA Flow Diagram.

Qualitative Synthesis
Among 66 studies20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85 included in the qualitative analysis, 55 studies20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,52,53,54,55,56,57,58,59,61,64,65,66,67,68,69,70,71,73,74,76,77,78,80,81,82 (3024 patients) were experimental, and 11 studies50,51,60,62,63,72,75,79,83,84,85 (2160 patients) were observational. Because analgesic techniques vary based on the type of surgery performed, we divided the populations accordingly. Thirty-nine studies20,21,22,23,24,25,27,28,29,30,32,33,34,36,38,39,40,44,45,46,47,48,49,60,64,65,66,67,68,70,73,74,76,77,78,79,80,81,82 (1805 patients) examined thoracotomy, 20 studies26,41,50,51,52,53,54,55,56,57,58,59,61,62,63,69,71,75,84,85 (2512 patients) examined thoracoscopy, 4 studies35,37,42,43 (235 patients) examined sternotomy, 2 studies72,83 (602 patients) examined both thoracotomy and thoracoscopy, and 1 study31 (30 patients) did not specify the type of thoracic surgery examined (Table 1).
The intervention used was single-injection ICNB in 51 studies20,21,22,23,24,25,26,29,30,31,32,33,34,36,39,41,42,43,44,45,46,47,48,50,51,52,53,55,56,57,58,59,60,61,64,65,67,68,69,70,71,72,74,75,76,78,79,81,83,84,85 (4690 patients) and continuous ICNB in 15 studies27,28,35,37,38,40,49,54,62,63,66,73,77,80,82 (494 patients). The comparison groups received TEA, interpleural analgesia, intercostal cryoanalgesia, transcutaneous electrical stimulation, PVB, erector spinae plane block, or serratus anterior plane block. The systemic analgesia group comprised patients in treatment arms who received any form of systemic analgesia (with or without placebo) and did not receive any form of regional analgesia (eg, TEA, PVB, or ICNB).
The risk of bias assessments across studies and for each of the coprimary outcomes are provided in eFigure 1 and eFigure 2 in the Supplement. Most experimental studies had a high risk of bias for allocation concealment,20,21,22,24,25,26,28,30,32,33,34,35,36,37,38,39,40,42,43,44,45,46,47,48,49,52,54,55,57,58,59,64,65,66,67,68,69,70,71,74,78,82 blinding of outcome assessors,29,32,44,46,58,59,63,67,71,74 blinding of participants and personnel,29,32,44,46,58,59,63,67,71,74 and other sources of bias,29,46,59,67,71 such as study design (eg, crossover studies and studies that used unvalidated pain measures). In 22 experimental studies21,22,24,25,29,33,38,40,45,49,52,55,61,67,68,69,70,71,73,74,80,81 (40.0%), a high risk of incomplete data for all outcomes was detected, primarily because of the lack of an intention-to-treat analysis. Most observational studies had a high risk of bias for inadequate control of confounding51,60,62,75,79,84,85 and a low risk of bias for incomplete follow-up50,51,62,63,72,75,79,83,84 and flawed measurement of exposure.50,51,62,63,72,75,79,83,84,85
Quantitative Synthesis
Among 59 studies20,22,25,26,28,29,30,31,32,33,34,36,37,38,39,40,41,42,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,65,66,67,68,69,71,72,73,74,77,78,79,80,81,83,84 included in the quantitative meta-analysis, 54 studies20,22,25,26,28,29,30,31,32,33,34,36,37,38,39,40,41,42,44,45,46,47,48,49,52,53,54,55,56,57,58,59,65,66,67,68,69,71,73,74,77,78,79,80,81 (2615 patients) were experimental, and 5 studies50,51,72,83,84 (710 patients) were observational. Forest plots summarizing the coprimary outcomes are provided in Figure 2 and eFigure 3 in the Supplement. A summary of findings in Table 2 shows the evidence profile and the specific grading of the level of certainty for each outcome. The certainty of evidence for most outcomes was downgraded for reasons including risk of bias, heterogeneity, and imprecision.
Figure 2. Effect Estimates of Mean Differences in Postoperative MMEs Between Intercostal Nerve Block Analgesia and Other Forms of Analgesia.
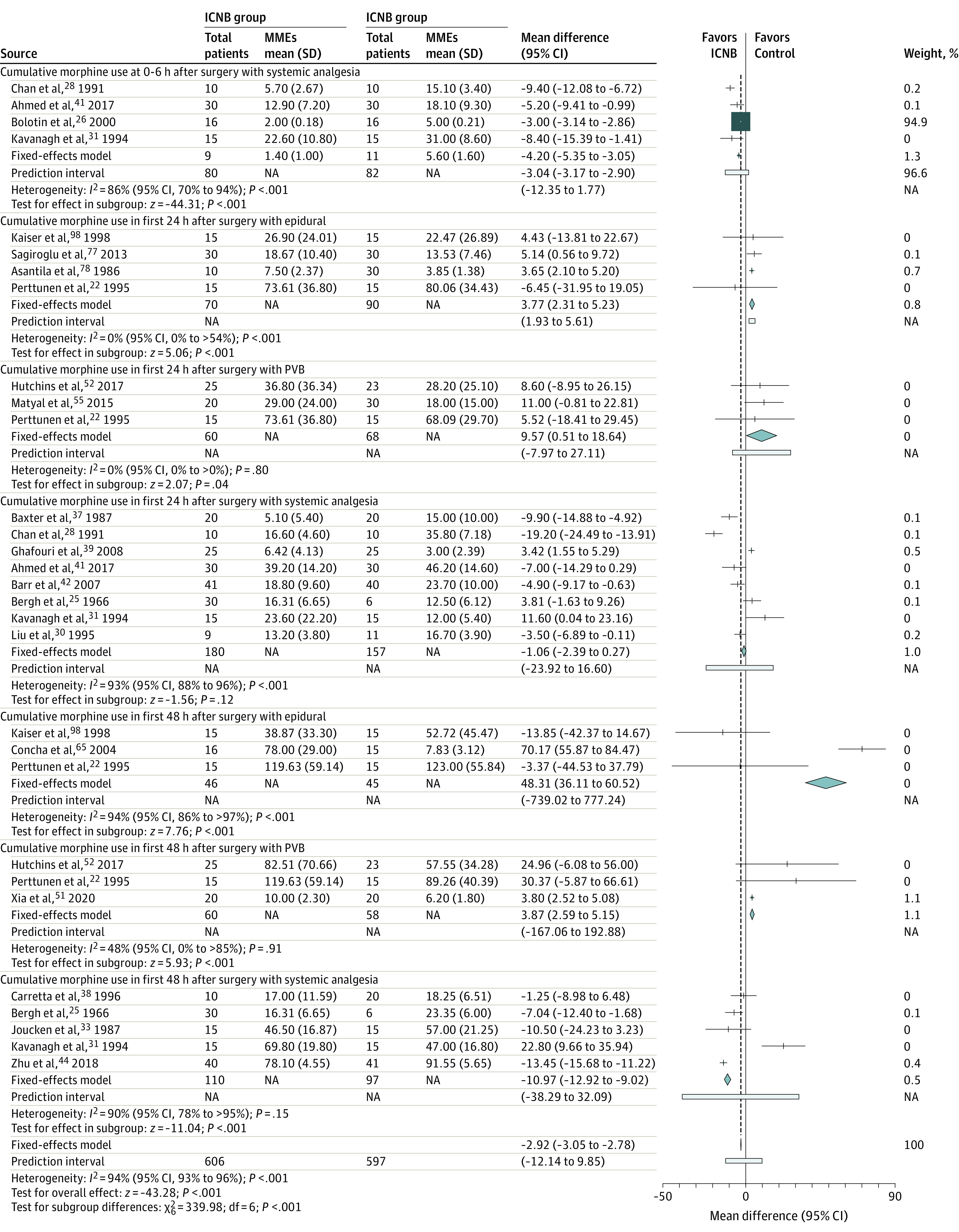
Diamonds represent the results of the fixed-effects model. The size of the squares reflects the weight of each study in the meta-analysis. ICNB indicates intercostal nerve block; MME morphine milligram equivalent; NA, not applicable; and PVB, paravertebral block.
Table 2. Evidence Profile for the Use of Intercostal Nerve Block Analgesia in Adults Undergoing Thoracic Surgery.
| Pain outcomea | Comparison | Limitations | Risk of bias (domains)b | Heterogeneity | Indirectness | Imprecision | Publication bias | Mean difference (95% CI) | No. of participants (No. of studies) | Certainty of evidence (GRADE domains)c | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| I2 (95% CI) | P value | ||||||||||
| Static pain at 0-6 h (11 RCTs28,30,31,32,41,44,46,48,49,57,58) | Systemic analgesia | Larger differences in patients having esophagectomy46 and pleurectomy49 | High (1, 2, and 3) | 97 (95 to 98) | .02 | Not detected | Not detected | Not detected | −1.40 (−1.46 to −1.33) | 627 (11 studies) | Moderate (a) |
| Dynamic pain at 0-6 h (3 RCTs30,44,58) | Systemic analgesia | Small samples | High (1, 2, and 3) | 95 (89 to 98) | <.001 | Not detected | Detected | Detected | −1.66 (−1.90 to −1.41) | 181 (3 studies) | Very low (a, b, d, and e) |
| Static pain at 7-24 h (10 RCTs28,30,31,38,41,44,46,48,49,58) | Systemic analgesia | 7 of 10 studies examined thoracotomy; high heterogeneity in effect estimates | High (1, 2, and 3) | 94 (90 to 96) | <.001 | Not detected | Not detected | Not detected | −1.27 (−1.40 to −1.13) | 557 (10 studies) | Low (a and b) |
| Dynamic pain at 7-24 h (4 RCTs30,31,44,58) | Systemic analgesia | Both groups received systemic analgesia via PCA and a single-injection neuraxial opioid in 1 study30 | High (1, 2, and 3) | 96 (94 to 98) | .34 | Not detected | Detected | Detected | −1.43 (−1.70 to −1.17) | 211 (4 studies) | Low (a, b, d, and e) |
| Static pain at 25-48 h (6 RCTs30,31,38,44,48,49) | Systemic analgesia | Larger differences in patients receiving esophagectomy49 | High (1, 2, and 3) | 64 (13 to 85) | <.001 | Not detected | Detected | Not serious | −0.37 (−0.60 to −0.14) | 297 (6 studies) | Very low (a, b, and d) |
| Dynamic pain at 25-48 h (3 RCTs30,31,44) | Systemic analgesia | Small samples; evidence for thoracotomy | High (1, 2, and 3) | 91 (78 to 97) | .02 | Not detected | Detected | Not detected | 0.51 (0.03 to 0.98) | 131 (3 studies) | Low (a, b, and d) |
| Static pain at 49-72 h (3 RCTs30,31,49) | Systemic analgesia | Small sample; most evidence for thoracotomy | High (1) | 95 (87 to >98) | <.001 | Not detected | Detected | Detected | 1.51 (0.94 to 2.08) | 66 (3 studies) | Very low (a, b, d, and e) |
| Static pain at 0-6 h (9 RCTs22,65,68,69,73,74,77,78,80) | TEA | 8of 9 studies examined thoracotomy | High (1, 2, 3, and 4) | 41 (0 to 73) | .09 | Not detected | Not detected | Not detected | 0.49 (0.18 to 0.79) | 389 (9 studies) | Moderate (a) |
| Dynamic Pain at 0-6 h (4 RCTs22,65,74,77) | TEA | Small sample; inconsistent results; most evidence for thoracotomy | High (1, 2, 3, and 4) | 61 (0 to 87) | .05 | Not detected | Detected | Not detected | 0.13 (−0.27 to 0.52) | 171 (4 studies) | Low (a and d) |
| Static pain at 7-24 h (10 RCTs and 1 NRSI22,65,68,69,71,73,74,77,78,80,84) | TEA | Observational evidence included | High (1, 2, 3, 4, 6, and 7) | 35 (0 to 68) | .34 | Not detected | Not detected | Not serious | 0.41 (0.21 to 0.61) | 672 (11 studies) | Moderate (a) |
| Dynamic pain at 7-24 h (4 RCTs22,65,74,77) | TEA | All studies examined thoracotomy | High (1, 2, 3, and 4) | 34 (0 to 77) | <.001 | Not detected | Detected | Not detected | 0.79 (0.28 to 1.29) | 171 (4 studies) | Low (a and d) |
| Static pain at 25-48 h (4 RCTs and 1 NRSI22,65,71,80,84) | TEA | Observational evidence included | High (1, 2, 3, 4, 6, and 7) | 67 (13 to 87) | .21 | Not detected | Not detected | Detected | 0.16 (−0.04 to 0.37) | 414 (5 studies) | Low (a and e) |
| Static pain at 0-6 h (6 RCTs and 1 NRSI22,50,53,54,56,57,58) | PVB | 1 of 7 studies examined thoracotomy; all others examined thoracoscopy | High (1, 2, and 3) | 97 (95 to 98) | .02 | Not detected | Not detected | Not detected | 0.22 (0.15 to 0.28) | 372 (7 studies) | Moderate (a) |
| Dynamic pain at 0-6 h (3 RCTs22,53,58) | PVB | Few studies; different results for thoracotomy vs thoracoscopy | High (1, 2, and 3) | 6 (0 to 90) | .09 | Not detected | Detected | Detected | 0.89 (0.70 to 1.08) | 158 (3 studies) | Very low (a, d, and e) |
| Static pain at 7-24 h (6 RCTs22,52,54,56,58,75) | PVB | 1 of 6 studies examined thoracotomy | High (1, 2, and 3) | 86 (70 to 93) | <.001 | Not detected | Not serious | Not serious | 0.83 (0.71 to 0.94) | 322 (6 studies) | Low (a and b) |
| Dynamic pain at 7-24 h (3 RCTs22,52,54,56,58,75) | PVB | Few studies; different results for thoracotomy vs thoracoscopy | High (1, 2, and 3) | 91 (76 to 97) | .12 | Not detected | Detected | Detected | 1.29 (1.16 to 1.41) | 158 (3 studies) | Very low (a, b, d, and e) |
| Static pain at 25-48 h (5 RCTs22,52,53,54,56) | PVB | Inconsistent findings, with 1 study using continuous PVB vs single-injection ICNB52 | High (1, 2, and 3) | 80 (52 to 91) | .12 | Not detected | Detected | Not detected | 0.07 (−0.04 to 0.19) | 242 (5 studies) | Very low (a, b, and d) |
| Cumulative opioid consumption (MMEs) at 6 h (5 RCTs26,28,30,31,41) | Systemic analgesia | Small samples | Unclear (1) | 86 (70 to 94) | <.001 | Not detected | Detected | High concern | −3.04 (−3.17 to −2.90) | 162 (5 studies) | Very low (a, d, and e) |
| Cumulative opioid consumption (MMEs) in first 24 h (8 RCTs25,28,30,31,37,39,41,42) | Systemic analgesia | 2 of 8 studies examined sternotomy | High (1, 2, and 3) | 93 (88 to 96) | .80 | Not detected | Not detected | Not detected | −1.06 (−2.39 to 0.27) | 337 (8 studies) | Low (a and b) |
| Cumulative opioid consumption (MMEs) in first 48 h (5 RCTs25,31,33,38,44) | Systemic analgesia | 1 study with additional multimodal regimen in ICNB group31 | High (1, 2, 3, and 4) | 90 (78 to >95) | .91 | Indirectness for thoracoscopy | Detected | Detected | −10.97 (−12.92 to −9.02) | 207 (5 studies) | Very low (a, b, d, and e) |
| Cumulative opioid consumption (MMEs) in first 24 h (4 RCTs22,66,77,78) | TEA | Small samples | High (1, 2, and 3) | 0 (0 to >54) | <.001 | Indirectness for thoracoscopy | Detected | Not serious | 3.77 (2.31 to 5.23) | 160 (4 studies) | Low (a and d) |
| Cumulative opioid consumption (MMEs) at 48 h (3 RCTs22,65,66) | TEA | 1 study with TEA group without supplemental systemic opioids | High (1, 2, and 3) | 94 (86 to >97) | <.001 | Indirectness for thoracoscopy | Detected | Detected | 48.31 (36.11 to 60.52) | 91 (3 studies) | Very low (a, b, d, and e) |
| Cumulative opioid consumption (MMEs) in first 24 h (3 RCTs22,52,55) | PVB | Small samples | High (1, 2, 3, and 4) | 0 (0 to >0) | <.001 | Not detected | Detected | Not serious | 9.57 (0.51 to 18.64) | 128 (3 studies) | Low (a and d) |
| Cumulative opioid consumption (MMEs) in first 48 h (2 RCTs and 1 NRSI22,51,52) | PVB | Small samples | High (1, 2, 3, 4, 6, and 7) | 48 (0 to >85) | .15 | Not detected | Detected | Detected | 3.87 (2.59 to 5.15) | 118 (3 studies) | Very low (a, d, and e) |
Abbreviations: GRADE, Grading of Recommendations, Assessment, Development and Evaluation; ICNB, intercostal nerve block; MME, morphine milligram equivalent; NRSI, nonrandomized study of therapeutic intervention; PCA, patient-controlled analgesia; PVB, paravertebral block; RCT, randomized clinical trial; TEA, thoracic epidural analgesia; VAS, visual analog scale.
Pain intensity was assessed using VAS score (range, 0-10 points, with 0 indicating no pain and 10 indicting severe pain).
Risk of bias domains in RCTs: 1 indicates allocation concealment; 2, blinding of outcome assessors for all outcomes; 3, blinding of participants and personnel for all outcomes; 4, incomplete outcome data for all outcomes; and 5, selective reporting, sequence generation. Risk of bias domains in NRSIs: 6 indicates failure to adequately control for confounding; 7, failure to develop and apply appropriate eligibility criteria; 8, flawed measurement of exposure or outcome; and 9, incomplete follow-up.
GRADE domains for downgrading the evidence: a indicates risk of bias; b, heterogeneity; c, indirectness; d, imprecision; and e, publication bias.
Static and Dynamic Pain Intensity
Overall, ICNB was superior to systemic analgesia with regard to static and dynamic pain during the first 24 hours after surgery (eFigure 3A in the Supplement). The largest pain reduction occurred at 0 to 6 hours after surgery for both static pain (mean score difference, −1.40 points; 95% CI, −1.46 to −1.33 points) and dynamic pain (mean score difference, −1.66; 95% CI, −1.90 to −1.41). The benefit of ICNB analgesia decreased progressively over time. Static pain scores were lower in the ICNB group at 25 to 48 hours after surgery (mean score difference, −0.37 points; 95% CI, −0.60 to −0.14 points) and shifted in favor of systemic analgesia after 48 hours (mean score difference, 1.51 points; 95% CI, 0.94-2.08 points). Dynamic pain scores changed in favor of systemic analgesia at 25 to 48 hours after surgery (mean score difference, 0.51 points; 95% CI, 0.03-0.98 points).
In the thoracotomy subgroup, ICNB was superior to systemic analgesia with respect to static pain at 0 to 6 hours (mean score difference, −1.88 points; 95% CI, −2.07 to −1.69 points), 7 to 24 hours (mean score difference, −1.55 points; 95% CI, −1.81 to −1.29 points), and 25 to 48 hours (mean score difference, −0.38 points; 95% CI, −0.62 to −0.15 points) after surgery (eFigure 4 in the Supplement). In the thoracoscopy subgroup, ICNB was superior to systemic analgesia for static pain during the first 6 hours after surgery (mean score difference, −1.33 points; 95% CI, −1.40 to −1.27 points).
Intercostal nerve block analgesia was marginally inferior to TEA with regard to static pain during the first 24 hours after surgery only (0-6 hours: mean score difference, 0.49 points [95% CI, 0.18-0.79 points]; 7-24 hours: mean score difference, 0.41 points [95% CI, 0.21-0.61 points]) (eFigure 3B in the Supplement). For dynamic pain, ICNB was noninferior to TEA at 7 to 24 hours after surgery only (mean score difference, 0.79 points; 95% CI, 0.28-1.29 points). In the thoracotomy subgroup, no substantial differences in pain intensity between ICNB and TEA were observed (eg, dynamic pain at 0-6 hours: mean score difference, 0.13 points [95% CI, −0.27 to 0.52 points]; static pain at 0-6 hours: mean score difference, 0.64 points [95% CI, 0.27-1.02 points]) (eFigure 4 in the Supplement). Data for the thoracoscopy subgroup were available only for static pain at 7 to 24 hours after surgery, with a marginal difference in pain scores favoring TEA (mean score difference, 0.32 points; 95% CI, 0.04-0.60 points) (eFigure 4 in the Supplement).
Intercostal nerve block analgesia was inferior to PVB with regard to dynamic and static pain (eFigure 3B in the Supplement). The largest difference was noted in dynamic pain between 7 and 24 hours after surgery (mean score difference, 1.29 points; 95% CI, 1.16-1.41 points). In the thoracoscopy subgroup, patients who received ICNB had higher static pain scores between 7 and 24 hours after surgery compared with those who received PVB (mean score difference, 0.84 points; 95% CI, 0.72-0.96 points) (eFigure 4 in the Supplement).
Opioid Consumption
The use of ICNB was associated with an opioid-sparing benefit compared with systemic analgesia. Overall, the reduction in opioid consumption associated with ICNB vs systemic analgesia started within the first 6 hours after surgery (mean difference, −3.04 MMEs; 95% CI, −3.17 to −2.90 MMEs) and peaked at 48 hours after surgery (mean difference, −10.97 MMEs; 95% CI, −12.92 to −9.02 MMEs) (Figure 2). In the thoracotomy subgroup, no difference was noted between ICNB and systemic analgesia during the first 24 hours after surgery (mean difference, 0.26 MMEs; 95% CI, −1.25 to 1.76 MMEs) (eFigure 5 in the Supplement). However, a reduction in opioid consumption was present at 48 hours after surgery (mean difference, −11.73 MMEs; 95% CI, −13.70 to −9.76 MMEs).
Intercostal nerve block analgesia was inferior to TEA with regard to opioid consumption at 24 hours after surgery (mean difference, 3.77 MMEs; 95% CI, 2.31-5.23 MMEs) (Figure 2). This effect was more marked at 48 hours after surgery, during which opioid consumption increased to 48.31 MMEs (95% CI, 36.11-60.52 MMEs). These findings were specific to patients undergoing thoracotomy. The high heterogeneity was explained by the Concha et al65 study, in which patients allocated to the TEA group only received opioids epidurally, which may have overestimated the opioid-sparing benefit of TEA.
Intercostal nerve block analgesia was only inferior to PVB at 48 hours after surgery (mean difference, 3.87 MMEs; 95% CI, 2.59-5.15 MMEs) (Figure 2).
Secondary Outcomes
Nausea and Vomiting
Intercostal nerve block analgesia was associated with a reduction in the risk of nausea and vomiting compared with systemic analgesia (OR, 0.44; 95% CI, 0.20-0.94) (eFigure 6 in the Supplement). The opposite result was observed for ICNB vs TEA (OR, 1.60; 95% CI, 0.96-2.66) and PVB (OR, 1.66; 95% CI, 0.96-2.89). In the thoracotomy subgroup, no significant differences were observed between ICNB and TEA (eFigure 7 in the Supplement). In the thoracoscopy subgroup, no significant differences were observed between ICNB and PVB (eFigure 7 in the Supplement).
The risk of cardiovascular complications was similar between ICNB and systemic analgesia (OR, 1.07; 95% CI, 0.44-2.63) (eFigure 6 in the Supplement). However, ICNB was associated with a reduction in the risk of cardiovascular complications compared with TEA analgesia (OR, 0.66; 95% CI, 0.46-0.93). In the thoracotomy subgroup, ICNB was associated with a reduced risk of cardiovascular complications compared with TEA (OR, 0.68; 95% CI, 0.47-0.98) (eFigure 7 in the Supplement). In the thoracoscopy subgroup, ICNB was inferior to PVB (OR, 3.4; 95% CI, 1.27-9.08) (eFigure 7 in the Supplement).
The use of ICNB was associated with a reduction in the risk of arterial hypotension compared with TEA (OR, 0.20; 95% CI, 0.06-0.74) (eFigure 6 in the Supplement). In the thoracotomy subgroup, ICNB was associated with a reduction in the risk of hypotension compared with TEA (OR, 0.21; 95% CI, 0.05-0.87) (eFigure 7 in the Supplement). No data were available for thoracoscopic surgery.
Intercostal nerve block analgesia was associated with a reduction in the risk of pulmonary complications compared with systemic analgesia (OR, 0.45; 95% CI, 0.26-0.79) (eFigure 6 in the Supplement). No difference was noted between ICNB and TEA (OR, 0.86; 95% CI, 0.63-1.18) or PVB (OR, 1.07; 95% CI, 0.25-4.63). In the thoracotomy subgroup, ICNB was superior to systemic analgesia but noninferior to TEA (eFigure 7 in the Supplement). No data were available for thoracoscopic surgery.
With few adverse events reported, no significant difference in risk was noted between ICNB and TEA with regard to 30-day mortality, neurologic complications, catheter or injection site infection, hematoma, pruritus, or urinary retention (eFigure 6 in the Supplement). In addition, no substantial difference in the risk of urinary retention was found between ICNB and PVB. Results remained similar when stratified by type of surgery (eFigure 7 in the Supplement).
Pulmonary Function
From baseline, ICNB was associated with higher forced expiratory volume in the first second compared with systemic analgesia at 7 to 24 hours (mean difference, 20.19%; 95% CI, 16.45%-23.93%), 25 to 48 hours (mean difference, 15.75%; 95% CI, 12.35%-19.14%), 49 to 72 hours (mean difference, 19.57%; 95% CI, 16.63%-22.52%), and more than 72 hours (mean difference, 19.75%; 95%CI, 16.32%-23.18%) after surgery (eFigure 8 and eFigure 9 in the Supplement). These results were specific to the thoracotomy subgroup.
Intercostal nerve block analgesia was associated with higher forced vital capacity from baseline compared with systemic analgesia at 7 to 24 hours (mean difference, 10.95%; 95% CI, 8.34%-13.57%) and 25 to 48 hours (mean difference, 8.89%; 95% CI, 6.39%-11.38%) after surgery (eFigure 8 and eFigure 9 in the Supplement). These results were specific to the thoracotomy subgroup. When compared with TEA, no difference was observed in the period of 7 to 24 hours after surgery (mean difference, 3.78%; 95% CI, −2.13% to 9.69%).
Length of Stay
Data from 7 studies22,66,69,71,73,77,84 (478 participants) did not reveal differences in hospital length of stay with the use of ICNB vs TEA (mean difference, −3.38 hours; 95% CI, −10.75 to 4.00 hours) (eFigure 10 in the Supplement).
In the thoracotomy subgroup, ICNB was associated with an increased length of stay of approximately 14.3 hours (95% CI, 0.15-28.45 hours) vs TEA (eFigure 11 in the Supplement). In the thoracoscopy subgroup, the use of ICNB was associated with a decreased length of stay of approximately −9.97 hours (95% CI, −18.61 to −1.33 hours) vs TEA (eFigure 11 in the Supplement).
A slight increase in the length of stay occurred when ICNB was compared with PVB (mean difference, 5.27 hours; 95% CI, 1.11-9.42 hours) (eFigure 11 in the Supplement). The results remained similar when limited to thoracoscopic procedures.
Discussion
In this systematic review and meta-analysis, the use of single-injection ICNB among adults undergoing thoracic surgery was associated with a small reduction in pain scores during the first 24 hours after surgery. Intercostal nerve block analgesia was superior to systemic opioid-based analgesia, noninferior to TEA, and marginally inferior to PVB. Because ICNB analgesia was also associated with better pulmonary function and a reduction in the risk of pulmonary complications, these findings were clinically relevant. Although ICNB was associated with reductions in opioid consumption compared with systemic analgesia alone, patients receiving ICNB consumed more opioids than those receiving TEA or PVB. However, caution is warranted when interpreting these findings because the quality of evidence was reduced by the limitations of the included studies.
Unlike previous reviews,11,12 our study provided estimates of the strength and duration of analgesic benefits. These estimates may allow clinicians to balance the benefits and harms of regional analgesia. Notably, both pulmonary and cardiovascular complications have been associated with postoperative mortality among patients undergoing thoracic surgery.10 Our results bring into question the superiority of TEA with regard to analgesia because the differences were minimal and inconsistent.87
The data suggested that the benefit of ICNB analgesia decreases progressively and disappears at 24 to 48 hours after surgery. Reliance on ICNB after this period may result in an abrupt lack of analgesia or rebound pain, represented by higher pain scores at 24 hours after surgery for dynamic pain and 48 hours after surgery for static pain.88 This finding is relevant because the severity of acute pain may be the main measure associated with the occurrence of chronic pain.89 Notably, the fact that ICNB was noninferior to TEA may underscore the known limitations of TEA, which has reported failure rates of up to 30%.90 Nevertheless, the success rate of TEA may be improved by the use of ultrasonography91 or the implementation of a preoperative block area.92 Comparisons between the use of ICNB with liposomal bupivacaine vs other regional analgesia techniques have only been performed in observational studies.72,83 Hussain et al93 recently reported that the use of liposomal bupivacaine in peripheral nerve block analgesia was not superior to plain local anesthetic formulations. Therefore, we do not consider the use of liposomal bupivacaine as indicated to provide sustained and beneficial analgesia after thoracic surgery.
Systemic hypotension is a known adverse event associated with TEA.94 We found that ICNB was associated with a reduction in the risk of hypotension compared with TEA. Whether TEA-associated hypotension is associated with cardiovascular events is unclear given that neuraxial blockade has not been independently associated with worse cardiovascular outcomes.95 Meta-analyses comparing TEA with PVB have also found limited high-quality evidence suggesting that PVB is associated with a lower risk of hypotension than TEA without differences in morbidity or mortality.9,96 However, most studies comparing the impact of TEA with that of other techniques have not investigated the incidence of silent events, such as myocardial injury after surgery, which may be associated with postoperative mortality.97
Limitations
This study has several limitations. First, most studies20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,42,43,44,45,46,47,48,49,51,52,54,55,56,57,58,59,60,61,62,64,65,66,67,68,69,70,71,73,74,75,77,78,79,80,81,82,84,85 included in the meta-analysis had at least 1 domain at a high risk of bias. In addition to small samples, differences in the protocol designs and types of analgesia produced high heterogeneity and imprecision. Differences in opioid consumption associated with different types of analgesia during certain intervals, such as ICNB vs TEA at 48 hours after surgery, may be overestimated. Second, we were unable to perform subgroup analyses incorporating continuous techniques or extended-release formulations. However, the benefits of extended-release medications have recently come into question,93 highlighting the need for pharmacological innovation. Third, the analysis of postoperative complications was limited by the use of observational data and the inadequate outcome definitions provided by the randomized clinical trials included in the meta-analysis. Nevertheless, observational studies can overcome the risk of sampling error associated with small samples.98 Fourth, most studies20,21,23,25,26,28,29,31,33,34,36,38,39,41,46,49,50,55,57,61,62,63,64,65,68,69,70,71,73,76,78,80,82 did not include complications as a primary or secondary outcome, raising concerns about detection bias.
Conclusions
This systematic review and meta-analysis found that single-injection ICNB was associated with a reduction in pain during the first 24 hours after thoracic surgery. Within the limitations of the available evidence, ICNB was superior to systemic opioid-based analgesia, noninferior to TEA, and marginally inferior to PVB. Although a small opioid-sparing benefit was found for ICNB alone, TEA and PVB were more favorable when opioid reduction was a consideration. Therefore, ICNB analgesia may be most beneficial for cases in which TEA or PVB are not indicated. Randomized clinical trials with rigorous methodological approaches and a priori outcomes that include safety end points are needed.
eFigure 1. Risk of Bias Assessment Across Experimental and Observational Studies
eFigure 2. Risk of Bias Assessments Within Each of the Coprimary Outcomes
eFigure 3. Forest Plots With Effect Estimates of Mean Differences in Acute Postoperative Pain Between ICNB and Other Forms of Analgesia
eFigure 4. Forest Plots With Effect Estimates of Mean Differences in Acute Postoperative Pain Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery
eFigure 5. Forest Plots With Effect Estimates of Mean Differences in Postoperative Morphine Milligram Equivalents Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery
eFigure 6. Forest Plots With Effect Estimates of Odds Ratios for Postoperative Complications Between ICNB and Other Forms of Analgesia
eFigure 7. Forest Plots With Effect Estimates of Odds Ratios for Postoperative Complications Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery
eFigure 8. Forest Plots With Effect Estimates of Mean Differences in Postoperative Pulmonary Function Between ICNB and Other Forms of Analgesia
eFigure 9. Forest Plots With Effect Estimates of Mean Differences in Postoperative Pulmonary Function Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery
eFigure 10. Forest Plots With Effect Estimates of Mean Differences in Length of Stay Between ICNB and Other Forms of Analgesia
eFigure 11. Forest Plots With Effect Estimates of Mean Differences in Length of Stay Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery
References
- 1.Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287-2298. doi: 10.2147/JPR.S144066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bendixen M, Jorgensen OD, Kronborg C, Andersen C, Licht PB. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. 2016;17(6):836-844. doi: 10.1016/S1470-2045(16)00173-X [DOI] [PubMed] [Google Scholar]
- 3.Marshall K, McLaughlin K. Pain management in thoracic surgery. Thorac Surg Clin. 2020;30(3):339-346. doi: 10.1016/j.thorsurg.2020.03.001 [DOI] [PubMed] [Google Scholar]
- 4.Marciniak D, Kelava M, Hargrave J. Fascial plane blocks in thoracic surgery: a new era or plain painful? Curr Opin Anaesthesiol. 2020;33(1):1-9. doi: 10.1097/ACO.0000000000000803 [DOI] [PubMed] [Google Scholar]
- 5.Pommerening MJ, Landau A, Hrebinko K, Luketich JD, Dhupar R. An analysis of analgesia and opioid prescribing for veterans after thoracic surgery. Sci Rep. 2020;10(1):11348. doi: 10.1038/s41598-020-68303-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Batchelor TJP, Rasburn NJ, Abdelnour-Berchtold E, et al. Guidelines for enhanced recovery after lung surgery: recommendations of the Enhanced Recovery After Surgery (ERAS) Society and the European Society of Thoracic Surgeons (ESTS). Eur J Cardiothorac Surg. 2019;55(1):91-115. doi: 10.1093/ejcts/ezy301 [DOI] [PubMed] [Google Scholar]
- 7.Schuster M, Gottschalk A, Freitag M, Standl T. Cost drivers in patient-controlled epidural analgesia for postoperative pain management after major surgery. Anesth Analg. 2004;98(3):708-713. doi: 10.1213/01.ANE.0000096040.02725.74 [DOI] [PubMed] [Google Scholar]
- 8.Gramigni E, Bracco D, Carli F. Epidural analgesia and postoperative orthostatic haemodynamic changes: observational study. Eur J Anaesthesiol. 2013;30(7):398-404. doi: 10.1097/EJA.0b013e32835b162c [DOI] [PubMed] [Google Scholar]
- 9.Baidya DK, Khanna P, Maitra S. Analgesic efficacy and safety of thoracic paravertebral and epidural analgesia for thoracic surgery: a systematic review and meta-analysis. Interact Cardiovasc Thorac Surg. 2014;18(5):626-635. doi: 10.1093/icvts/ivt551 [DOI] [PubMed] [Google Scholar]
- 10.Servais EL, Towe CW, Brown LM, et al. The Society of Thoracic Surgeons general thoracic surgery database: 2020 update on outcomes and research. Ann Thorac Surg. 2020;110(3):768-775. doi: 10.1016/j.athoracsur.2020.06.006 [DOI] [PubMed] [Google Scholar]
- 11.Detterbeck FC. Efficacy of methods of intercostal nerve blockade for pain relief after thoracotomy. Ann Thorac Surg. 2005;80(4):1550-1559. doi: 10.1016/j.athoracsur.2004.11.051 [DOI] [PubMed] [Google Scholar]
- 12.Joshi GP, Bonnet F, Shah R, et al. A systematic review of randomized trials evaluating regional techniques for postthoracotomy analgesia. Anesth Analg. 2008;107(3):1026-1040. doi: 10.1213/01.ane.0000333274.63501.ff [DOI] [PubMed] [Google Scholar]
- 13.Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group . Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi: 10.1371/journal.pmed.1000097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Intercostal nerve block analgesia for thoracic surgery. PROSPERO identifier: CRD42021224783. January 15, 2021. Accessed October 15, 2021. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42021224783
- 15.Myles PS, Myles DB, Galagher W, et al. Measuring acute postoperative pain using the visual analog scale: the minimal clinically important difference and patient acceptable symptom state. Br J Anaesth. 2017;118(3):424-429. doi: 10.1093/bja/aew466 [DOI] [PubMed] [Google Scholar]
- 16.Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5(1):13. doi: 10.1186/1471-2288-5-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rohatgi A. WebPlotDigitizer. Accessed December 2020. https://automeris.io/WebPlotDigitizer/images/wpd.png
- 18.Guyatt GH, Oxman AD, Vist G, et al. GRADE guidelines: 4. rating the quality of evidence—study limitations (risk of bias). J Clin Epidemiol. 2011;64(4):407-415. doi: 10.1016/j.jclinepi.2010.07.017 [DOI] [PubMed] [Google Scholar]
- 19.Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-406. doi: 10.1016/j.jclinepi.2010.07.015 [DOI] [PubMed] [Google Scholar]
- 20.de la Rocha AG, Chambers K. Pain amelioration after thoracotomy: a prospective, randomized study. Ann Thorac Surg. 1984;37(3):239-242. doi: 10.1016/S0003-4975(10)60332-3 [DOI] [PubMed] [Google Scholar]
- 21.Orr IA, Keenan DJ, Dundee JW. Improved pain relief after thoracotomy: use of cryoprobe and morphine infusion. BMJ (Clin Res Ed). 1981;283(6297):945-948. doi: 10.1136/bmj.283.6297.945 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Perttunen K, Nilsson E, Heinonen J, Hirvisalo EL, Salo JA, Kalso E. Extradural, paravertebral and intercostal nerve blocks for post-thoracotomy pain. Br J Anaesth. 1995;75(5):541-547. doi: 10.1093/bja/75.5.541 [DOI] [PubMed] [Google Scholar]
- 23.Fiorelli S, Leopizzi G, Menna C, et al. Ultrasound-guided erector spinae plane block versus intercostal nerve block for post-minithoracotomy acute pain management: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2020;34(9):2421-2429. doi: 10.1053/j.jvca.2020.01.026 [DOI] [PubMed] [Google Scholar]
- 24.Shafei H, Chamberlain M, Natrajan KN, Khan MA, Gandhi RG. Intrapleural bupivacaine for early post-thoracotomy analgesia—comparison with bupivacaine intercostal block and cryofreezing. Thorac Cardiovasc Surg. 1990;38(1):38-41. doi: 10.1055/s-2007-1013989 [DOI] [PubMed] [Google Scholar]
- 25.Bergh NP, Dottori O, Lof BA, Simonsson BG, Ygge H. Effect of intercostal block on lung function after thoracotomy. Acta Anaesthesiol Scand Suppl. 1966;24:85-95. doi: 10.1111/j.1399-6576.1966.tb01107.x [DOI] [PubMed] [Google Scholar]
- 26.Bolotin G, Lazarovici H, Uretzky G, Zlotnick AY, Tamir A, Saute M. The efficacy of intraoperative internal intercostal nerve block during video-assisted thoracic surgery on postoperative pain. Ann Thorac Surg. 2000;70(6):1872-1875. doi: 10.1016/S0003-4975(00)01757-4 [DOI] [PubMed] [Google Scholar]
- 27.Dryden CM, McMenemin I, Duthie DJ. Efficacy of continuous intercostal bupivacaine for pain relief after thoracotomy. Br J Anaesth. 1993;70(5):508-510. doi: 10.1093/bja/70.5.508 [DOI] [PubMed] [Google Scholar]
- 28.Chan VW, Chung F, Cheng DC, Seyone C, Chung A, Kirby TJ. Analgesic and pulmonary effects of continuous intercostal nerve block following thoracotomy. Can J Anaesth. 1991;38(6):733-739. doi: 10.1007/BF03008451 [DOI] [PubMed] [Google Scholar]
- 29.Toledo-Pereyra LH, DeMeester TR. Prospective randomized evaluation of intrathoracic intercostal nerve block with bupivacaine on postoperative ventilatory function. Ann Thorac Surg. 1979;27(3):203-205. doi: 10.1016/S0003-4975(10)63275-4 [DOI] [PubMed] [Google Scholar]
- 30.Liu M, Rock P, Grass JA, et al. Double-blind randomized evaluation of intercostal nerve blocks as an adjuvant to subarachnoid administered morphine for post-thoracotomy analgesia. Reg Anesth. 1995;20(5):418-425. [PubMed] [Google Scholar]
- 31.Kavanagh BP, Katz J, Sandler AN, et al. Multimodal analgesia before thoracic surgery does not reduce postoperative pain. Br J Anaesth. 1994;73(2):184-189. doi: 10.1093/bja/73.2.184 [DOI] [PubMed] [Google Scholar]
- 32.Zhan Y, Chen G, Huang J, Hou B, Liu W, Chen S. Effect of intercostal nerve block combined with general anesthesia on the stress response in patients undergoing minimally invasive mitral valve surgery. Exp Ther Med. 2017;14(4):3259-3264. doi: 10.3892/etm.2017.4868 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Joucken K, Michel L, Schoevaerdts JC, Mayne A, Randour P. Cryoanalgesia for post-thoracotomy pain relief. Acta Anaesthesiol Belg. 1987;38(2):179-183. [PubMed] [Google Scholar]
- 34.Faust RJ, Nauss LA. Post-thoracotomy intercostal block: comparison of its effects on pulmonary function with those of intramuscular meperidine. Anesth Analg. 1976;55(4):542-546. doi: 10.1213/00000539-197607000-00019 [DOI] [PubMed] [Google Scholar]
- 35.Dowling R, Thielmeier K, Ghaly A, Barber D, Boice T, Dine A. Improved pain control after cardiac surgery: results of a randomized, double-blind, clinical trial. J Thorac Cardiovasc Surg. 2003;126(5):1271-1278. doi: 10.1016/S0022-5223(03)00585-3 [DOI] [PubMed] [Google Scholar]
- 36.Delilkan AE, Lee CK, Yong NK, Ganendran A. Post-operative local analgesia for thoracotomy with direct bupivacaine intercostal blocks. Anaesthesia. 1973;28(5):561-567. doi: 10.1111/j.1365-2044.1973.tb00527.x [DOI] [PubMed] [Google Scholar]
- 37.Baxter AD, Jennings FO, Harris RS, Flynn JF, Way J. Continuous intercostal blockade after cardiac surgery. Br J Anaesth. 1987;59(2):162-166. doi: 10.1093/bja/59.2.162 [DOI] [PubMed] [Google Scholar]
- 38.Carretta A, Zannini P, Chiesa G, Altese R, Melloni G, Grossi A. Efficacy of ketorolac tromethamine and extrapleural intercostal nerve block on post-thoracotomy pain. a prospective, randomized study. Int Surg. 1996;81(3):224-228. [PubMed] [Google Scholar]
- 39.Ghafouri A, Movafegh A, Nasr-Esfahani M, Gholamrezanezhad A, Madhkhan S. Post-thoracotomy pain and pulmonary function—comparison of intermittent intercostal bupivacaine vs intravenous pethidine. Middle East J Anaesthesiol. 2008;19(4):767-780. [PubMed] [Google Scholar]
- 40.Kolvenbach H, Lauven PM, Schneider B, Kunath U. Repetitive intercostal nerve block via catheter for postoperative pain relief after thoracotomy. Thorac Cardiovasc Surg. 1989;37(5):273-276. doi: 10.1055/s-2007-1020331 [DOI] [PubMed] [Google Scholar]
- 41.Ahmed Z, Samad K, Ullah H. Role of intercostal nerve block in reducing postoperative pain following video-assisted thoracoscopy: a randomized controlled trial. Saudi J Anaesth. 2017;11(1):54-57. doi: 10.4103/1658-354X.197342 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Barr AM, Tutungi E, Almeida AA. Parasternal intercostal block with ropivacaine for pain management after cardiac surgery: a double-blind, randomized, controlled trial. J Cardiothorac Vasc Anesth. 2007;21(4):547-553. doi: 10.1053/j.jvca.2006.09.003 [DOI] [PubMed] [Google Scholar]
- 43.Lee CY, Robinson DA, Johnson CA Jr, et al. A randomized controlled trial of liposomal bupivacaine parasternal intercostal block for sternotomy. Ann Thorac Surg. 2019;107(1):128-134. doi: 10.1016/j.athoracsur.2018.06.081 [DOI] [PubMed] [Google Scholar]
- 44.Zhu M, Gu Y, Sun X, Liu X, Chen W, Miao C. Ultrasound-guided intercostal nerve block following esophagectomy for acute postoperative pain relief in the postanesthesia care unit. Pain Pract. 2018;18(7):879-883. doi: 10.1111/papr.12689 [DOI] [PubMed] [Google Scholar]
- 45.Galway JE, Caves PK, Dundee JW. Effect of intercostal nerve blockade during operation on lung function and the relief of pain following thoracotomy. Br J Anaesth. 1975;47(6):730-735. doi: 10.1093/bja/47.6.730 [DOI] [PubMed] [Google Scholar]
- 46.Wang Y, Cheng J, Yang L, Wang J, Liu H, Lv Z. Ropivacaine for intercostal nerve block improves early postoperative cognitive dysfunction in patients following thoracotomy for esophageal cancer. Med Sci Monit. 2019;25:460-465. doi: 10.12659/MSM.912328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kaplan JA, Miller ED Jr, Gallagher EG Jr. Postoperative analgesia for thoracotomy patients. Anesth Analg. 1975;54(6):773-777. doi: 10.1213/00000539-197511000-00025 [DOI] [PubMed] [Google Scholar]
- 48.D’Andrilli A, Ibrahim M, Ciccone AM, et al. Intrapleural intercostal nerve block associated with mini-thoracotomy improves pain control after major lung resection. Eur J Cardiothorac Surg. 2006;29(5):790-794. doi: 10.1016/j.ejcts.2006.01.002 [DOI] [PubMed] [Google Scholar]
- 49.Mozell EJ, Sabanathan S, Mearns AJ, Bickford-Smith PJ, Majid MR, Zografos G. Continuous extrapleural intercostal nerve block after pleurectomy. Thorax. 1991;46(1):21-24. doi: 10.1136/thx.46.1.21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Yang H, Dong Q, Liang L, et al. The comparison of ultrasound-guided thoracic paravertebral blockade and internal intercostal nerve block for non-intubated video-assisted thoracic surgery. J Thorac Dis. 2019;11(8):3476-3481. doi: 10.21037/jtd.2019.07.77 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Xia Z, Depypere L, Song Y, et al. Uniportal thoracoscopic wedge resection of lung nodules: paravertebral blocks are better than intercostal blocks. Surg Innov. 2020;27(4):358-365. doi: 10.1177/1553350620921753 [DOI] [PubMed] [Google Scholar]
- 52.Hutchins J, Sanchez J, Andrade R, Podgaetz E, Wang Q, Sikka R. Ultrasound-guided paravertebral catheter versus intercostal blocks for postoperative pain control in video-assisted thoracoscopic surgery: a prospective randomized trial. J Cardiothorac Vasc Anesth. 2017;31(2):458-463. doi: 10.1053/j.jvca.2016.08.010 [DOI] [PubMed] [Google Scholar]
- 53.Chen N, Qiao Q, Chen R, Xu Q, Zhang Y, Tian Y. The effect of ultrasound-guided intercostal nerve block, single-injection erector spinae plane block and multiple-injection paravertebral block on postoperative analgesia in thoracoscopic surgery: a randomized, double-blinded, clinical trial. J Clin Anesth. 2020;59:106-111. doi: 10.1016/j.jclinane.2019.07.002 [DOI] [PubMed] [Google Scholar]
- 54.Kadomatsu Y, Mori S, Ueno H, Uchiyama M, Wakai K. Comparison of the analgesic effects of modified continuous intercostal block and paravertebral block under surgeon’s direct vision after video-assisted thoracic surgery: a randomized clinical trial. Gen Thorac Cardiovasc Surg. 2018;66(7):425-431. doi: 10.1007/s11748-018-0936-8 [DOI] [PubMed] [Google Scholar]
- 55.Matyal R, Montealegre-Gallegos M, Shnider M, et al. Preemptive ultrasound-guided paravertebral block and immediate postoperative lung function. Gen Thorac Cardiovasc Surg. 2015;63(1):43-48. doi: 10.1007/s11748-014-0442-6 [DOI] [PubMed] [Google Scholar]
- 56.Wu C, Ma W, Cen Q, Cai Q, Wang J, Cao Y. A comparison of the incidence of supraventricular arrhythmias between thoracic paravertebral and intercostal nerve blocks in patients undergoing thoracoscopic surgery: a randomised trial. Eur J Anaesthesiol. 2018;35(10):792-798. doi: 10.1097/EJA.0000000000000837 [DOI] [PubMed] [Google Scholar]
- 57.Mogahed MM, Elkahwagy MS. Paravertebral block versus intercostal nerve block in non-intubated uniportal video-assisted thoracoscopic surgery: a randomised controlled trial. Heart Lung Circ. 2020;29(5):800-807. doi: 10.1016/j.hlc.2019.04.013 [DOI] [PubMed] [Google Scholar]
- 58.Xiang X, Zhou H, Wu Y, Fang J, Lian Y. Impact of supraglottic device with assist ventilation under general anesthesia combined with nerve block in uniportal video-assisted thoracoscopic surgery. Medicine (Baltimore). 2020;99(10):e19240. doi: 10.1097/MD.0000000000019240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Zheng Y, Wang H, Ma X, Cheng Z, Cao W, Shao D. Comparison of the effect of ultrasound-guided thoracic paravertebral nerve block and intercostal nerve block for video-assisted thoracic surgery under spontaneous-ventilating anesthesia. Rev Assoc Med Bras (1992). 2020;66(4):452-457. doi: 10.1590/1806-9282.66.4.452 [DOI] [PubMed] [Google Scholar]
- 60.Oksuz G, Sayan M, Arslan M, et al. The comparison of serratus anterior plane block versus intercostal block for postoperative analgesia following thoracotomy surgery. Anestezi Dergisi. 2018;26(4):223-228. [Google Scholar]
- 61.Kim S, Bae CM, Do YW, Moon S, Baek SI, Lee DH. Serratus anterior plane block and intercostal nerve block after thoracoscopic surgery. Thorac Cardiovasc Surg. 2021;69(6):564-569. [DOI] [PubMed] [Google Scholar]
- 62.Hsieh MJ, Wang KC, Liu HP, et al. Management of acute postoperative pain with continuous intercostal nerve block after single port video-assisted thoracoscopic anatomic resection. J Thorac Dis. 2016;8(12):3563-3571. doi: 10.21037/jtd.2016.12.30 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Wu CF, Hsieh MJ, Liu HP, et al. Management of post-operative pain by placement of an intraoperative intercostal catheter after single port video-assisted thoracoscopic surgery: a propensity-score matched study. J Thorac Dis. 2016;8(6):1087-1093. doi: 10.21037/jtd.2016.04.01 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Bachmann-Mennenga B, Biscoping J, Kuhn DF, et al. Intercostal nerve block, interpleural analgesia, thoracic epidural block or systemic opioid application for pain relief after thoracotomy? Eur J Cardiothorac Surg. 1993;7(1):12-18. doi: 10.1016/1010-7940(93)90141-W [DOI] [PubMed] [Google Scholar]
- 65.Concha M, Dagnino J, Cariaga M, Aguilera J, Aparicio R, Guerrero M. Analgesia after thoracotomy: epidural fentanyl/bupivacaine compared with intercostal nerve block plus intravenous morphine. J Cardiothorac Vasc Anesth. 2004;18(3):322-326. doi: 10.1053/j.jvca.2004.03.013 [DOI] [PubMed] [Google Scholar]
- 66.Kaiser AM, Zollinger A, De Lorenzi D, Largiader F, Weder W. Prospective, randomized comparison of extrapleural versus epidural analgesia for postthoracotomy pain. Ann Thorac Surg. 1998;66(2):367-372. doi: 10.1016/S0003-4975(98)00448-2 [DOI] [PubMed] [Google Scholar]
- 67.Wurnig PN, Lackner H, Teiner C, et al. Is intercostal block for pain management in thoracic surgery more successful than epidural anaesthesia? Eur J Cardiothorac Surg. 2002;21(6):1115-1119. doi: 10.1016/S1010-7940(02)00117-3 [DOI] [PubMed] [Google Scholar]
- 68.Scheinin B, Scheinin M, Asantila R, Lindberg R, Viinamaki O. Sympatho-adrenal and pituitary hormone responses during and immediately after thoracic surgery—modulation by four different pain treatments. Acta Anaesthesiol Scand. 1987;31(8):762-767. doi: 10.1111/j.1399-6576.1987.tb02660.x [DOI] [PubMed] [Google Scholar]
- 69.Pompeo E, Rogliani P, Cristino B, Schillaci O, Novelli G, Saltini C. Awake thoracoscopic biopsy of interstitial lung disease. Ann Thorac Surg. 2013;95(2):445-452. doi: 10.1016/j.athoracsur.2012.10.043 [DOI] [PubMed] [Google Scholar]
- 70.Takamori S, Yoshida S, Hayashi A, Matsuo T, Mitsuoka M, Shirouzu K. Intraoperative intercostal nerve blockade for postthoracotomy pain. Ann Thorac Surg. 2002;74(2):338-341. doi: 10.1016/S0003-4975(02)03710-4 [DOI] [PubMed] [Google Scholar]
- 71.Ueda K, Hayashi M, Murakami J, Tanaka T, Utada K, Hamano K. Intercostal block vs. epidural analgesia in thoracoscopic lung cancer surgery: a randomized trial. Gen Thorac Cardiovasc Surg. 2020;68(3):254-260. doi: 10.1007/s11748-019-01197-1 [DOI] [PubMed] [Google Scholar]
- 72.Mehran RJ, Walsh GL, Zalpour A, et al. Intercostal nerve blocks with liposomal bupivacaine: demonstration of safety, and potential benefits. Semin Thorac Cardiovasc Surg. 2017;29(4):531-537. doi: 10.1053/j.semtcvs.2017.06.004 [DOI] [PubMed] [Google Scholar]
- 73.Debreceni G, Molnar Z, Szelig L, Molnar TF. Continuous epidural or intercostal analgesia following thoracotomy: a prospective randomized double-blind clinical trial. Acta Anaesthesiol Scand. 2003;47(9):1091-1095. doi: 10.1034/j.1399-6576.2003.00208.x [DOI] [PubMed] [Google Scholar]
- 74.Vilvanathan S, Kuppuswamy B, Sahajanandan R. A randomized control trial to compare thoracic epidural with intercostal block plus intravenous morphine infusion for postoperative analgesia in patients undergoing elective thoracotomy. Ann Card Anaesth. 2020;23(2):127-133. doi: 10.4103/aca.ACA_167_18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Chen Z, Dong Q, Liang L. Effect of different thoracic anesthesia on postoperative cough. J Thorac Dis. 2018;10(6):3539-3547. doi: 10.21037/jtd.2018.05.126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Ranganathan P, Tadvi A, Jiwnani S, Karimundackal G, Pramesh CS. A randomised evaluation of intercostal block as an adjunct to epidural analgesia for post-thoracotomy pain. Indian J Anaesth. 2020;64(4):280-285. doi: 10.4103/ija.IJA_714_19 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Sagiroglu G, Baysal A, Kiraz OG, Meydan B, Tasçi AE, Iskender I. Comparison of continuous use of thoracic epidural analgesia and intercostal block for pain management after thoracotomy. Kardiochir Torakochirurgia Pol. 2013;10(3):244-250. [Google Scholar]
- 78.Asantila R, Rosenberg PH, Scheinin B. Comparison of different methods of postoperative analgesia after thoracotomy. Acta Anaesthesiol Scand. 1986;30(6):421-425. doi: 10.1111/j.1399-6576.1986.tb02445.x [DOI] [PubMed] [Google Scholar]
- 79.Khalil KG, Boutrous ML, Irani AD, et al. Operative intercostal nerve blocks with long-acting bupivacaine liposome for pain control after thoracotomy. Ann Thorac Surg. 2015;100(6):2013-2018. doi: 10.1016/j.athoracsur.2015.08.017 [DOI] [PubMed] [Google Scholar]
- 80.Dauphin A, Lubanska-Hubert E, Young JE, Miller JD, Bennett WF, Fuller HD. Comparative study of continuous extrapleural intercostal nerve block and lumbar epidural morphine in post-thoracotomy pain. Can J Surg. 1997;40(6):431-436. [PMC free article] [PubMed] [Google Scholar]
- 81.Meierhenrich R, Hock D, Kuhn S, et al. Analgesia and pulmonary function after lung surgery: is a single intercostal nerve block plus patient-controlled intravenous morphine as effective as patient-controlled epidural anaesthesia? a randomized non-inferiority clinical trial. Br J Anaesth. 2011;106(4):580-589. doi: 10.1093/bja/aeq418 [DOI] [PubMed] [Google Scholar]
- 82.Luketich JD, Land SR, Sullivan EA, et al. Thoracic epidural versus intercostal nerve catheter plus patient-controlled analgesia: a randomized study. Ann Thorac Surg. 2005;79(6):1845-1849. doi: 10.1016/j.athoracsur.2004.10.055 [DOI] [PubMed] [Google Scholar]
- 83.Rice DC, Cata JP, Mena GE, Rodriguez-Restrepo A, Correa AM, Mehran RJ. Posterior intercostal nerve block with liposomal bupivacaine: an alternative to thoracic epidural analgesia. Ann Thorac Surg. 2015;99(6):1953-1960. doi: 10.1016/j.athoracsur.2015.02.074 [DOI] [PubMed] [Google Scholar]
- 84.Hung MH, Chan KC, Liu YJ, et al. Nonintubated thoracoscopic lobectomy for lung cancer using epidural anesthesia and intercostal blockade: a retrospective cohort study of 238 cases. Medicine (Baltimore). 2015;94(13):e727. doi: 10.1097/MD.0000000000000727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Ambrogi V, Mineo TC. VATS biopsy for undetermined interstitial lung disease under non-general anesthesia: comparison between uniportal approach under intercostal block vs. three-ports in epidural anesthesia. J Thorac Dis. 2014;6(7):888-895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Higgins JPT, Thomas J, Chandler J, et al, eds. Cochrane Handbook for Systematic Reviews of Interventions. Version 6.2. Cochrane; 2021. Updated February 2021. Accessed August 2020. https://training.cochrane.org/handbook
- 87.Kopacz DJ, Emanuelsson BM, Thompson GE, Carpenter RL, Stephenson CA. Pharmacokinetics of ropivacaine and bupivacaine for bilateral intercostal blockade in healthy male volunteers. Anesthesiology. 1994;81(5):1139-1148. doi: 10.1097/00000542-199411000-00007 [DOI] [PubMed] [Google Scholar]
- 88.Barry GS, Bailey JG, Sardinha J, Brousseau P, Uppal V. Factors associated with rebound pain after peripheral nerve block for ambulatory surgery. Br J Anaesth. 2021;126(4):862-871. doi: 10.1016/j.bja.2020.10.035 [DOI] [PubMed] [Google Scholar]
- 89.Bayman EO, Parekh KR, Keech J, Selte A, Brennan TJ. A prospective study of chronic pain after thoracic surgery. Anesthesiology. 2017;126(5):938-951. doi: 10.1097/ALN.0000000000001576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Hermanides J, Hollmann MW, Stevens MF, Lirk P. Failed epidural: causes and management. Br J Anaesth. 2012;109(2):144-154. doi: 10.1093/bja/aes214 [DOI] [PubMed] [Google Scholar]
- 91.Shaikh F, Brzezinski J, Alexander S, et al. Ultrasound imaging for lumbar punctures and epidural catheterisations: systematic review and meta-analysis. BMJ. 2013;346:f1720. doi: 10.1136/bmj.f1720 [DOI] [PubMed] [Google Scholar]
- 92.Gleicher Y, Singer O, Choi S, McHardy P. Thoracic epidural catheter placement in a preoperative block area improves operating room efficiency and decreases epidural failure rate. Reg Anesth Pain Med. 2017;42(5):649-651. doi: 10.1097/AAP.0000000000000637 [DOI] [PubMed] [Google Scholar]
- 93.Hussain N, Brull R, Sheehy B, et al. Perineural liposomal bupivacaine is not superior to nonliposomal bupivacaine for peripheral nerve block analgesia. Anesthesiology. 2021;134(2):147-164. doi: 10.1097/ALN.0000000000003651 [DOI] [PubMed] [Google Scholar]
- 94.Leslie K, McIlroy D, Kasza J, et al. Neuraxial block and postoperative epidural analgesia: effects on outcomes in the POISE-2 trial. Br J Anaesth. 2016;116(1):100-112. doi: 10.1093/bja/aev255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Leslie K, McIlroy D, Kasza J, et al. Neuraxial block and postoperative epidural analgesia: effects on outcomes in the POISE-2 trial. Br J Anaesth. 2016;116(1):100-112. doi: 10.1093/bja/aev255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Yeung JHY, Gates S, Naidu BV, Wilson MJ, Smith FG. Paravertebral block versus thoracic epidural for patients undergoing thoracotomy. Cochrane Database Syst Rev. 2016;2(2):CD009121. doi: 10.1002/14651858.CD009121.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Botto F, Alonso-Coello P, Chan MTV, et al. ; Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION) Writing Group on behalf of the Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION) Investigators; Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators Writing Group; Vascular Events in Noncardiac Surgery Patients Cohort Evaluation Operations Committee; Vascular Events in Noncardiac Surgery Patients Cohort Evaluation (VISION) Study Investigators . Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120(3):564-578. doi: 10.1097/ALN.0000000000000113 [DOI] [PubMed] [Google Scholar]
- 98.Lin L. Bias caused by sampling error in meta-analysis with small sample sizes. PLoS One. 2018;13(9):e0204056. doi: 10.1371/journal.pone.0204056 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eFigure 1. Risk of Bias Assessment Across Experimental and Observational Studies
eFigure 2. Risk of Bias Assessments Within Each of the Coprimary Outcomes
eFigure 3. Forest Plots With Effect Estimates of Mean Differences in Acute Postoperative Pain Between ICNB and Other Forms of Analgesia
eFigure 4. Forest Plots With Effect Estimates of Mean Differences in Acute Postoperative Pain Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery
eFigure 5. Forest Plots With Effect Estimates of Mean Differences in Postoperative Morphine Milligram Equivalents Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery
eFigure 6. Forest Plots With Effect Estimates of Odds Ratios for Postoperative Complications Between ICNB and Other Forms of Analgesia
eFigure 7. Forest Plots With Effect Estimates of Odds Ratios for Postoperative Complications Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery
eFigure 8. Forest Plots With Effect Estimates of Mean Differences in Postoperative Pulmonary Function Between ICNB and Other Forms of Analgesia
eFigure 9. Forest Plots With Effect Estimates of Mean Differences in Postoperative Pulmonary Function Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery
eFigure 10. Forest Plots With Effect Estimates of Mean Differences in Length of Stay Between ICNB and Other Forms of Analgesia
eFigure 11. Forest Plots With Effect Estimates of Mean Differences in Length of Stay Between ICNB and Other Forms of Analgesia: Subgroup Analysis by Type of Surgery