

Abstract
Background:
Anterior cruciate ligament (ACL) injuries represent a significant burden to rugby players. Improving our understanding of the patterns and biomechanics that result in ACL injury may aid in the design of effective prevention programs.
Purpose:
To describe, using video analysis, the mechanisms, situational patterns, and biomechanics of ACL injuries in professional rugby matches. Further aims were to document injuries according to pitch location and timing within the match.
Study Design:
Case series; Level of evidence, 4.
Methods:
A total of 62 ACL injuries were identified in players of the 4 most important rugby leagues across 4 consecutive seasons. We analyzed 57 (92%) injury videos for injury mechanism and situational patterns; biomechanical analysis was performed on indirect and noncontact ACL injuries only (38 cases available). Three reviewers independently evaluated each video.
Results:
More injuries occurred while attacking than defending (41 [72%] vs 16 [28%]; P < .01). Regarding mechanism, 18 (32%) injuries were direct contact; 15 (26%), indirect contact; and 24 (42%), noncontact. Most direct contact injuries involved being tackled directly to the knee (n = 10). Three situational patterns were identified for players who had a noncontact or indirect contact injury: offensive change of direction (COD) (n = 18), being tackled (n = 10), and pressing/tackling (n = 8). Injuries generally involved a knee-loading strategy in the sagittal plane, which was accompanied by knee valgus loading in most cases (94%). Overall, 73% of injuries occurred during the first 40 minutes of effective playing time.
Conclusion:
Most ACL injuries in professional male rugby players happened through a noncontact or indirect contact mechanism (68%). Three situational patterns were described, including offensive change of direction, being tackled, and pressing/tackling. Biomechanical analysis confirmed a multiplanar mechanism, with a knee-loading pattern in the sagittal plane accompanied by dynamic valgus. As most injuries occurred in the first 40 minutes, accumulated fatigue appears not to be a major risk factor for ACL injury.
Keywords: injury prevention, ACL injury, injury mechanism, biomechanics
Anterior cruciate ligament (ACL) injury is a severe and concerning health issue for the professional rugby player, causing long layoff time. 12 Knee injuries constitute the highest injury burden within professional rugby, 12 with ACL injuries accounting for 29% of days missed. 12 Although most players (∼90%) return to play after ACL reconstruction, 33 the high injury burden and the risk of subsequent injury 33 are serious concerns, emphasizing the importance of reducing ACL injury incidence.
Understanding the mechanisms and situations that lead to ACL injuries is essential for the effective design of specific exercise programs to reduce ACL injury incidence. 34 Although many approaches are available to support an increased understanding of ACL injury mechanisms (ie, cadaveric studies, laboratory investigations, mathematical modeling studies), 5 video analysis can offer a valid tool to investigate playing situations preceding and during injuries. Several video analysis studies have been undertaken across different sports. ¶ Regarding rugby, just one study has been published to date. 27 Despite a well-designed study, there is a need to reproduce these findings in a larger cohort of injured players. Furthermore, there are inconsistencies concerning the timing of ACL injuries, in which the higher incidence late in the match is contrary to existing evidence for ACL injuries. 2,7,13,15,18,38 Additionally, there is a need to describe the situational patterns that lead to ACL injuries in a larger cohort and a greater need to clarify the biomechanics with consistent methodology during these situational patterns.
The purpose of this study was to describe, in a larger cohort of professional rugby players, the mechanisms, situational patterns, and biomechanics related to ACL injury. An additional purpose was to document the distribution of ACL injuries across the match and pitch location. 27
Methods
Injury Identification
A systematic search of online database resources was performed across 4 seasons (between 2015-2016 and 2018-2019 [until December 2018]) to identify ACL injuries occurring during matches in players of Super Rugby, Premiership, Top 14, and Pro 12/14. A total of 2163 matches were played in the considered time frame. To identify ACL injuries, each season and team roster were extracted from online databases and single-team websites, according to a previously adopted methodology 27 in the other existing study on rugby players. Second, the same systematic single-player approach was used for additional data sources, including national and local media, to look for injuries that may have been missed. Finally, an injury was included only when we were able to track an official communication of the medical staff of the team stating the nature of the ACL injury incurred by the player.
Video Extraction and Processing
Match videos were obtained from an online digital platform (Stats Perform). Videos were then downloaded and cut using Windows Movie Maker (Microsoft Corp). Each ACL injury video was cut to approximately 12 to 15 seconds before and 3 to 5 seconds after the estimated injury frame to accurately evaluate the playing situation that preceded the injury and injury mechanism.
Video Evaluation
Videos were reviewed and evaluated independently by 3 reviewers: 1 orthopaedic surgeon (A.G.) and 2 sports medicine physicians (F.D.V. and R.F.). Evaluation was performed according to 2 predetermined checklists (see Supplemental Tables S1 and S2). Each ACL injury video was downloaded on a personal computer, opened using an online software (Kinovea; KinoveaInk), and analyzed using an evaluation flow adapted from another sport. 13,35 Each reviewer evaluated the original video to define the injurious situation, defensive or offensive, which was categorized by ball possession and specific playing situation.
A series of views was then used to determine the injury mechanism and situational pattern, which were defined according to previous work. 13 Injury mechanism was used to define ACL injury causation, referring to the player-to-player interaction that led to the injury. Three categories of injury mechanism were used: noncontact, defined as an injury occurring without any contact before or at the injury frame; indirect contact, defined as an injury resulting from an external force applied to the footballer but not directly to the injured knee; and direct contact, defined as external force directly applied to the injured knee. 25 The player’s speed was categorized as high, low, and zero on the horizontal and vertical directions, as suggested by Waldén et al. 35 Running and suddenly cutting or decelerating were categorized as high horizontal speed, whereas landing from a clear jump was categorized as high vertical speed.
Situational patterns were used to describe the events that led to the ACL injuries. A pattern can be divided into a defensive or offensive situation, and this was done in the case of a noncontact or indirect contact mechanism. A defensive injury was defined as pressing when a player got injured during an attempt to tackle an opponent, though a few steps beforehand and through a purely noncontact mechanism. Initial contact and injury frame were independently assessed, given previous research indicating that ACL injuries typically occur within 40 milliseconds of initial contact. 13,21,22 Time between initial contact and injury frame in our analysis was 45 ± 3 milliseconds (mean ± standard deviation). Among the 3 reviewers, the mean difference in estimation between initial contact and injury frame was 3 milliseconds. The intraclass correlation coefficients among reviewers for initial contact and injury frame estimations were 1 and 0.81, respectively, indicating very good to excellent reliability.
After independent analysis, all 3 reviewers met for a 1-day comprehensive discussion about the main injury mechanism and situational patterns. In the absence of complete agreement among reviewers, problems were solved by consensus, as in previous research. 27,35
Biomechanical Analysis
Biomechanical analysis (referring to kinematic or intersegmental relationships) was performed on noncontact and indirect contact injuries if good-quality views of the frontal and/or sagittal planes were available. Biomechanical analysis was performed at initial contact and injury frame. When >1 view was available, composite videos were created via manual synchronization using visual clues (eg, initial ground contact). 27 One video had 4 camera views, 6 had 3 views, 23 had 2 views, and 27 had 1 view.
Sagittal and frontal plane (trunk tilt) angles were estimated using a custom-made software program (GPEM Screen Editor; GPEM srl) to the nearest 5° at initial contact and estimated injury frame. The remaining estimated joint positions for the frontal and coronal planes were recorded according to the appearance at initial contact and injury frame. Foot strike at or after contact with the ground at initial contact and injury frame was evaluated according to previous methodology. 13,35 A checklist of items that were evaluated is available in Supplemental Table S2.
Injuries Distributed by Match Time and Field Location
For each available injury video, a list of data regarding the match time and field distribution was gathered via systematic web revision and video analysis (eg, pitch location of injury). The following ACL injury information was considered: time when the ACL injury occurred (minute of the match and match half), number of minutes played by the ACL-injured athlete, and field location. The field location was determined by zones with dimension calculated (square meters) per the rugby field dimensions stated in the official regulation (https://laws.worldrugby.org). The pitch was divided into 12 zones (see Supplemental Table S4 and Figure S1).
Statistical Analysis
Continuous variables are presented as mean and standard deviation or median (range) as appropriate according to distribution. Discrete variables are presented as absolute number and percentage of the total observations. The proportion test was used to explore differences in the distribution of ACL injuries between match halves, and an a priori statistically significant level of P < .05 was used. Microsoft Excel 2016 and Stata 12 (StataCorp) were used for these analyses.
Results
A total of 62 ACL injuries were tracked and included during matches of the Super Rugby (n = 12), Six Nations (n = 9), Premiership (n = 10), Top 14 (n = 7), Pro12/Pro14 (n = 12), and Champions Cup (n = 8), as well as other international matches (n = 4). There were 36 (60%) injuries to the right ACL and 24 (39%) injuries to the left ACL (2 were unidentifiable), with 57 primary and 5 secondary ACL injuries (4 contralateral ACL injuries in previous ACL reconstruction cases and 1 ipsilateral reinjury). A detailed study flow is presented in Figure 1.
Figure 1.
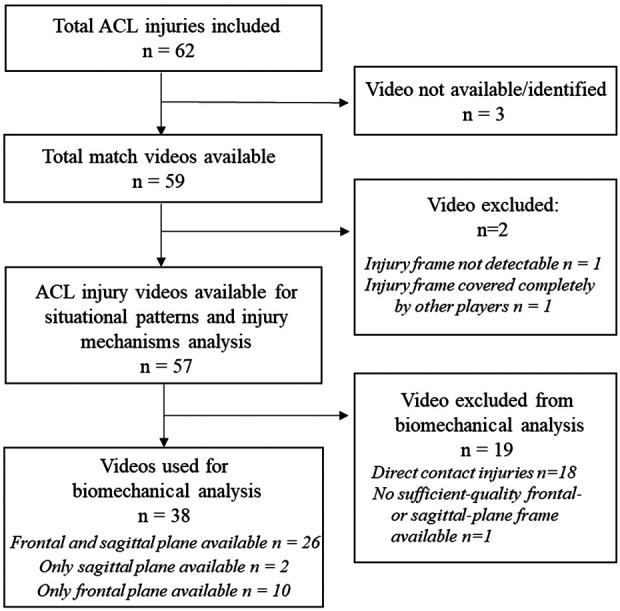
Flowchart of the study. ACL, anterior cruciate ligament.
Injury Mechanism Analysis
Video footage was available and identifiable for injury mechanism and situational pattern analysis in 57 cases (92%). More injuries occurred while attacking (n = 41; 72%) than defending (n = 16; 28% [P < .01]). We categorized 18 (32%) direct contact, 15 (26%) indirect contact, and 24 (42%) noncontact injuries (Table 1).
Table 1.
Analysis of Injury Mechanism (N = 57 injuries) a
| Variable | Results (No.) |
|---|---|
| Weather conditions | Raining: yes (3), no (54); Sunny: yes (18), no (16); Night (23) |
| Playing phase before injury | Offensive (41), defensive (16) |
| Field location of injury | |
| Long axis of the field | Zone: defensive (4), middefensive (16), midoffensive (27), offensive (10) |
| Short axis of the field | Corridor: left (11), middle (32), right (14) |
| Player contact preceding injury | No (28), yes (27) |
| If contact, where? | Upper body (16), injured leg (5), pelvis (4), pelvis + upper body (3), pelvis + injured leg (1) |
| Player contact at injury frame | Yes (32), no (25) |
| If indirect contact, where? | Upper body (9), pelvis (3), pelvis + upper body (1), uninjured leg (1) |
| Injury classification | Direct contact (18), indirect contact (15), noncontact (24) |
| How many feet on ground | 1 foot (35), both feet (4) |
| Leg loading at injury frame | Injured leg (39) |
| Speed | |
| Horizontal | Zero (1), low (11), high (27) |
| Vertical | Zero (29), low (7), high (3) |
a See Supplemental Table S1 for video evaluation checklist.
Direct Contact Injuries
Direct contact injuries (n = 18) occurred in defensive (n = 7) and offensive (n = 11) playing situations, with the pattern of 10 injuries classified as being tackled, 5 as tackling, and 3 as rucking. Biomechanically, most direct contact ACL injuries resulted from an external force, with valgus loading of the knee (n = 9). Other injuries occurred because of hyperextension (n = 4) or significant posterior tibial force application (n = 3) likely resulting in anterior tibial translation (2 injuries were unclear).
Situational Pattern of Indirect and Noncontact Injuries
Indirect and noncontact injuries occurred more in offensive (n = 30) than defensive (n = 9) situations. We identified 3 main situational patterns for the injuries:
Offensive change of direction (COD; n = 18) (Figure 2)
Being tackled (n = 10) (Figure 3)
Pressing/tackling (n = 8) (Figure 4)
Figure 2.

Offensive change-of-direction injuries. Anterior and posterior views: (A, E) sidestep to deceive the player, (B, F) wide cut with initial foot contact to the ground, (C, G) injury frame, and (D, H) loss of balance after injury.
Figure 3.

Injuries while being tackled. Indirect contact with perturbation to the upper body and lower limb: (A, E) player contact while in possession of the ball, (B, F) initial contact of injured leg to the ground with continued contact, (C, G) injury frame, and (D, H) loss of balance after injury.
Figure 4.

Pressing injuries. Noncontact pressing injury: (A) tracking the player, (B) initial contact with the ground to press the player with a change-of-direction movement, (C) injury frame, and (D) loss of balance after injury. Indirect contact pressing injury: (E) tracking the player with opponent contact to the upper body, (F) initial contact of the injured leg to the ground with continued contact, (G) injury frame, and (H) loss of balance after injury .
The other 3 injuries did not constitute a situational pattern and were classified as landing from a jump.
Offensive COD was the most common situational pattern (Figure 2), accounting for nearly half of injuries without direct knee contact (46%), and was an offensive-type injury. Being tackled, the second-most common situational pattern (Figure 3), accounted for nearly a quarter of injuries (26%). Contact most commonly occurred to the upper body (n = 5), pelvis (n = 3), or both simultaneously (n = 1). One injury involved contact to the injured leg to a part other than the knee.
Pressing/tackling injuries (Figure 4) accounted for just over one-fifth (21%) of injuries, with 6 pressing-type and 2 tackling-type injuries. These injuries were defensive in nature. In pressing, the player was injured during noncontact deceleration or cutting (1 injury involved indirect contact to the upper body). In tackling injuries, there was opponent contact before or at the estimated injury frame.
Biomechanical Analysis
Biomechanical analysis was possible in 38 cases, with 26 having both images of the frontal and sagittal planes, 2 with images in only the sagittal plane, and 10 with images in just the frontal plane. The most common intersegmental body positions are shown in Figure 5.
Figure 5.

Common intersegmental body relationships at initial contact and injury frame in offensive change-of-direction anterior cruciate ligament injuries. IC, initial contact; IF, injury frame.
All angle data are reported as median values. All in all, in the sagittal plane at initial contact, players displayed a relatively upright trunk (15°), an early flexed hip (40°), shallow knee flexion (15°), and early plantarflexed ankle (10°), with heel strike in over half (51%) of cases. In the frontal plane at initial contact, the trunk was on slightly tilted ipsilaterally (5°), with most cases having an ipsilateral tilt to the injured side (67%), with a slightly higher tendency to be rotated toward the uninjured side (39%) than the injured side (22%). In one-third of cases, initial contact occurred with the trunk in neutral rotation (39%). The hip was abducted in most cases (91%) and in neutral (63%) or valgus (37%) knee appearance.
Regarding the injury frame, in the sagittal plane, the trunk remained upright (10°) with the hip similarly flexed (37.5°). The knee was more flexed than at initial contact but still relatively straight (30°). The ankle remained plantarflexed (10°), and the foot was planted flat in all cases (100%). On the frontal plane at injury frame, the trunk was slightly more tilted ipsilaterally (10°), with the majority of cases tilted to the injured leg (80%), and in most cases, the trunk was rotated toward the uninjured side (78%). The hip remained abducted in most cases (86%), and in nearly all cases, we detected a knee valgus appearance (94%). A significant increase in hip internal rotation and/or adduction from initial contact to injury frame was seen in the majority of cases (83%). A complete knee valgus collapse occurred in 12 (34%) cases, with no collapse in 23 cases (66%). Additional details are presented in Tables 2 and 3.
Table 2.
Sagittal Plane Metrics of Indirect and Noncontact Anterior Cruciate Ligament Injuries (n = 28) a
| Variable | Total | Offensive COD | Being Tackled | Pressing/Tackling | Other |
|---|---|---|---|---|---|
| Flexion angle, deg b | |||||
| Trunk at IC | 15 (50 to –25) | 15 (20 to –5) | 20 (30 to –25) | 17.5 (20 to 5) | 27.5 (50 to 5) |
| Trunk at IF | 10 (95 to –20) | 10 (25 to 0) | 17.5 (40 to –20) | 10 (10 to 5) | 52.5 (95 to 10) |
| Hip at IC | 40 (65 to 20) | 45 (55 to 20) | 37.5 (50 to 5) | 55 (65 to 40) | 35 (40 to 30) |
| Hip at IF | 37.5 (70 to 5) | 45 (55 to 15) | 25 (60 to 20) | 45 (70 to 20) | 27.5 (50 to 5) |
| Knee at IC | 15 (50 to 0) | 15 (35 to 0) | 7.5 (50 to 0) | 20 (30 to 0) | 15 (20 to 10) |
| Knee at IF | 30 (65 to –20) | 35 (55 to 15) | 7.5 (60 to –20) | 32.5 (65 to 5) | 10 (40 to –20) |
| Ankle at IC | –10 (10 to –40) | –10 (0 to –40) | –10 (10 to –25) | –12.5 (0 to –15) | –22.5 (–15 to –30) |
| Ankle at IF | –10 (15 to –50) | –5 (15 to –30) | –32.5 (15 to –50) | –15 (–10 to –25) | –15 (0 to –30) |
| Foot strike at IC | |||||
| Heel | 18 (51) | 8 (53) | 4 (40) | 5 (71) | 1 (33) |
| Flat | 15 (43) | 7 (47) | 5 (50) | 2 (29) | 1 (33) |
| Toe | 2 (6) | 0 (0) | 1 (10) | 0 (0) | 1 (33) |
| Foot strike at IF | |||||
| Heel | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Flat | 34 (100) | 15 (100) | 10 (100) | 6 (100) | 9 (100) |
| Toe | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
a Data are reported as median (range) or n (%). COD, change of direction; IC, initial contact; IF, injury frame.
b Positive values indicate flexion; negative values indicate extension.
Table 3.
Frontal and Transverse Plane Metrics of Noncontact or Indirect Contact Anterior Cruciate Ligament Injuries, Stratified by Situational Patterns (Data on 35 Cases) a
| Variable | Total | Offensive COD | Being Tackled | Pressing/Tackling | Other |
|---|---|---|---|---|---|
| Trunk tilt at IC | |||||
| Angle, deg b | 5 (30 to –15) | 5 (30 to 0) | 5 (15 to –10) | 5 (20 to –15) | 0 (10 to –5) |
| Toward injured | 20 (67) | 9 (69) | 4 (57) | 6 (86) | 1 (33) |
| Neutral | 6 (20) | 4 (31) | 1 (14) | 0 (0) | 1 (33) |
| Toward uninjured | 4 (13) | 0 (0) | 2 (29) | 1 (14) | 1 (33) |
| Trunk tilt at IF | |||||
| Angle, deg b | 10 (25 to –20) | 10 (15 to 0) | 15 (25 to –10) | 10 (25 to –20) | 10 (25 to –5) |
| Toward injured | 24 (80) | 10 (77) | 6 (86) | 6 (86) | 2 (67) |
| Neutral | 3 (10) | 3 (23) | 0 (0) | 0 (0) | 0 (0) |
| Toward uninjured | 3 (10) | 0 (0) | 1 (14) | 1 (14) | 1 (33) |
| Trunk rotation at IC | |||||
| Toward injured | 8 (22) | 7 (41) | 1 (11) | 0 (0) | 0 (0) |
| Neutral | 14 (39) | 6 (35) | 3 (33) | 2 (29) | 3 (100) |
| Toward uninjured | 14 (39) | 4 (24) | 5 (56) | 5 (71) | 0 (0) |
| Trunk rotation at IF | |||||
| Toward injured | 3 (8) | 1 (6) | 2 (22) | 0 (0) | 0 (0) |
| Neutral | 5 (14) | 3 (18) | 1 (11) | 0 (0) | 1 (33) |
| Toward uninjured | 28 (78) | 13 (76) | 6 (67) | 7 (100) | 2 (67) |
| Frontal plane hip alignment at IC | |||||
| Abduction | 32 (91) | 17 (100) | 7 (87) | 6 (86) | 2 (67) |
| Neutral | 3 (9) | 0 (0) | 1 (13) | 1 (14) | 1 (33) |
| Adduction | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Frontal plane hip alignment at IF | |||||
| Abduction | 30 (86) | 16 (94) | 5 (63) | 7 (100) | 2 (67) |
| Neutral | 5 (14) | 1 (6) | 3 (37) | 0 (0) | 1 (33) |
| Adduction | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Frontal plane knee alignment at IC | |||||
| Valgus | 13 (37) | 5 (29) | 3 (37) | 4 (57) | 1 (33) |
| Neutral | 22 (63) | 12 (71) | 5 (63) | 3 (43) | 2 (67) |
| Varus | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Frontal plane knee alignment at IF | |||||
| Valgus | 33 (94) | 17 (100) | 7 (87) | 7 (100) | 2 (67) |
| Neutral | 1 (3) | 0 (0) | 0 (0) | 0 (0) | 1 (33) |
| Varus | 1 (3) | 0 (0) | 1 (13) | 0 (0) | 0 (0) |
| Foot position at IC | |||||
| External | 15 (49) | 6 (43) | 4 (57) | 2 (29) | 3 (100) |
| Neutral | 11 (35) | 5 (36) | 2 (29) | 4 (57) | 0 (0) |
| Internal | 5 (16) | 3 (21) | 1 (14) | 1 (14) | 0 (0) |
| Foot position at IF | |||||
| External | 17 (53) | 7 (50) | 5 (63) | 3 (43) | 2 (67) |
| Neutral | 6 (19) | 3 (21) | 2 (25) | 1 (14) | 0 (0) |
| Internal | 9 (28) | 4 (29) | 1 (12) | 3 (43) | 1 (33) |
| Significant hip IR/ADD from IC to IF | |||||
| Yes | 29 (83) | 15 (88) | 6 (75) | 6 (86) | 2 (67) |
| No | 6 (17) | 2 (12) | 2 (25) | 1 (14) | 1 (33) |
| Valgus collapse | |||||
| Yes | 12 (34) | 5 (29) | 3 (38) | 3 (29) | 1 (33) |
| No | 23 (66) | 12 (71) | 5 (62) | 4 (71) | 2 (67) |
a Eight injuries had incomplete biomechanical data on the frontal plane. Data are reported as n (%) or median (range). ADD, adduction; COD, change of direction; IC, initial contact; IF, injury frame; IR, internal rotation.
b Positive values indicate ipsilateral (injured); negative values indicate contralateral.
Match and Field Distribution
There was no significant difference in the number of injuries that occurred during the first half of a match (n = 32; 57%) and second half (n = 24; 43%) (Figure 6A). Regarding effective minutes played, there was a general trend for a decrease in ACL injuries for number of minutes played during the match. The mean time when ACL injuries occurred was 37 minutes into the game. For the minutes effectively played (correcting for substitutions), 73% of ACL injuries (n = 41) occurred within the first 40 minutes of effective time (P < .05) (Figure 6B). The mean length of time played before the ACL injury was 28 ± 21 minutes (median, 23 minutes). Finally, it should be noted that as many as 36% of ACL injuries (n = 20) happened within the first 15 minutes of gameplay. A further specification of the distribution of ACL injuries during the match according to the injury mechanism is presented in Supplemental Figures S7 and S8 . Injuries according to pitch location are provided in Supplemental Tables S3 to S4 and Figures S1 to S6.
Figure 6.

Distribution of ACL injuries through the match for 56 cases (minutes of gameplay were unable to be determined for 1 player). A decrease in the number of ACL injuries was noted as the game progressed. Dotted lines represent the linear tendency. Distribution of injuries according to (A) match minute/zone and (B) effective playing time (number of minutes of effective gameplay before ACL injury). ACL, anterior cruciate ligament.
Discussion
The most important finding of the present study is that most ACL injuries in elite-level rugby occur without direct contact mechanism at injury frame (68%) but a large proportion do occur by some form of indirect contact. For indirect and noncontact ACL injuries, 3 main situational patterns were identified. Furthermore, ACL injuries do not appear to be due to accumulated fatigue during match play.
Most ACL injuries occurred while attacking (72%), a slightly higher proportion than the 63% reported by Montgomery et al 27 and much higher than that in other research in soccer, which typically has noted more injuries while defending than attacking. 8,13,18,35 The higher proportion of offensive injuries signifies an increased risk for the ball carrier, and is also attributed to an increased risk of contact-type injuries. The proportion of injuries according to contact mechanism was almost identical to that in the other existing rugby study. 27 One-third (32%) of injuries in our study were direct contact, one-fourth (26%) were indirect contact, and 42% were noncontact. Montgomery et al 27 cited 56% contact- and 42% noncontact-type injuries, with the contact type broken down to 29% direct and 23% indirect (with 2 cases unsure). The near identical nature of injuries implies these data as likely being highly representative of ACL injury mechanisms in elite male rugby. The proportion of direct contact ACL injuries in this study (32%) is similar to that in Australian football (32%) 11 but much higher than that in soccer (12%-15%), 13,35 basketball (10%), 23 and handball (5%). 28 The proportion of these direct contact ACL injuries likely relates to the level of contact associated with rugby, classified as a collision sport.
We identified 3 main situational patterns for indirect contact and noncontact ACL injuries: offensive COD, being tackled, and pressing/tackling. Montgomery et al 27 noted only 1 type of noncontact ACL injury, defined as offensive running, with the other mechanism being a contact-based mechanism defined as tackled, which was partially aligned to our findings. The offensive COD pattern that we reported is in line with Montgomery et al, 27 as 8 of 11 (73%) of their offensive running injuries involved a sidestep cut maneuver. Our proportion of offensive COD injuries (30%) was also similar to that in their study (28%). As such, it appears that offensive COD is a high-risk situation for ACL injury in rugby. This is particularly relevant, as the injuries were all noncontact in nature and thus potentially preventable. The COD technique may be effectively trained to reduce external knee abduction moment, 14 and screening for the COD technique was recently proven to be associated to ACL injury risk in another cohort of athletes. 10 As such, an appropriate COD training technique is warranted in rugby players, ideally starting at the academy level.
We reported an indirect contact mechanism of being tackled but without contact to the knee. In this injury scenario, contact occurred predominantly to the upper body and/or pelvis, while the player was attacking. We identified a similar mechanism in soccer, accounting for 20% of all injuries. 13 Furthermore, studies in other sports have noted a perturbation-type injury. For example, in basketball 23 and more recently American football, a “perturbation-like scenario” accounted for half of ACL injuries. 20 This mechanical perturbation in other sports is typically coupled with a distraction immediately before injury.
Finally, we identified another situational pattern, pressing/tackling, which accounted for one-fifth of noncontact and indirect injuries. This pressing-type mechanism is common in soccer 13,35 and could be seen as being similar to defensive running as indicated by Montgomery et al. 27 Pressing injuries often involve a neurocognitive perturbation where the player has to change direction to attempt to tackle a player. Most of these injuries were noncontact or involved mechanical perturbation and may also be preventable.
Our data support the current evidence that ACL injuries generally occur in early knee flexion. 13,22,23,27,28,35 Similar to another study in rugby, 27 as well as research from other sports, 13,21,22,35 we reported a high knee-loading pattern, with limited motion at joints other than the knee. From initial contact to injury frame, there was no change in hip or ankle flexion but a small change in knee flexion (15º increase from 15º to 30º). A 30º knee angle corresponds to high ACL loading and a vulnerable position. 9,36 Collectively, the movement strategy in the sagittal plane would be expected to result in excessive loading via the knee joint in a compromised position. Tackling-based injuries with an indirect mechanism involved considerably less knee flexion, with some hyperextension injuries.
Similar to other studies, we showed that this preferential knee-loading movement strategy that led to ACL injury was accompanied by altered frontal and transverse plane motions. This combined triplanar motion is also thought to lead to ACL injury. 26,30 Knee valgus and valgus-type loading from initial contact to injury frame was found, as in previous research. 13,21,34 Similarly, hip abduction was common at initial contact, 13,21,35 with a significant increase in hip internal rotation and/or adduction (medial thigh motion) from initial contact to injury frame in most cases (83%), as in other studies. 13,35 ACL injuries are thought to be multiplanar, 26,30 and these findings supports that notion within this rugby cohort, especially for the offensive COD situational pattern and pressing.
Similar to previous research, we noted a lateral trunk lean on the injury frame (10º). 13,19 A lateral trunk lean may increase ACL loading attributed to a lateral shift of center mass, achieving a vector line lateral to the knee joint and causing a knee abduction moment. 29 This alteration in frontal plane motion is likely due to the high external knee abduction moment determined by hip abduction 14,29 on a laterally oriented and planted foot position outside the base of support. 14,31
Being tackled involved larger lateral trunk excursion from initial contact to the injury frame, while offensive COD appeared to involve an initial lateral trunk lean at initial contact, with a small reduction from initial contact to the injury frame. This likely indicated an attempt to deceive the player before COD, highlighting the performance injury risk conundrum in noncontact ACL injuries. 16
We noted that a valgus collapse occurred in one-third of cases (34%). This is higher than that in elite soccer players (8%-13%) 13,35 but less than in female athletes (∼50%), 23 who are known to have a much higher incidence of knee valgus collapse than are males. 23 Given the similar kinematics of rugby ACL injuries reported in this study and another 27 to those in soccer players during match play, 13,35 it is possible that a higher level of absolute loading (potentially attributed to higher body mass) led to a higher rate of collapse in this rugby cohort. A higher degree of contact in rugby could also be thought to explain this, but we did note a similar percentage of valgus collapse–type mechanisms during noncontact type COD (29%) and indirect contact–type “tackled” (38%) situational patterns.
Virtually all ACL injuries occurred in dry conditions in our study (95%), similar to previous findings (94%-97%). 13,18,27,35 It is thought that dry conditions increase the risk of ACL injury likely because of the increased ground friction affecting shoe-to-surface interactions. 1,37
Regarding the distribution during gameplay, previous research 27 has reported that nearly half of injuries (47% of noncontact injuries and 42% of all injuries) occurred during the last 20 minutes of the rugby match. Our data contradict these findings and indicate that accumulating fatigue throughout the match is not a key risk factor for injury, in agreement with research from other sports. 2,7,13,15,18,38 Although other authors have discussed fatigue as a risk factor for ACL within a complex web of determinants of risk, 4 it is likely that factors other than fatigue may be more relevant to ACL injuries.
Montgomery et al 27 described a heel strike pattern as being important in ACL injury in their cohort, which was prevalent and appeared to be highly common in later stages of the match. This heel strike pattern seemed to differentiate between those injured in matches and the same movements not resulting in injury within the laboratory setting, similar to research in other sports. 6
Regarding the minutes of effective gameplay (correcting for substitutions), we found that over one-third of ACL injuries happened in the first 15 minutes of play, and most ACL injuries took place after a mean of 28 ± 21 minutes of play. A recent systematic review revealed that the mean playing time for rugby players was almost 69 minutes, 17 much longer than the mean time frame to ACL injuries in our cohort. Our data suggest that high-speed actions at the beginning of match play are the trigger of an important quota of ACL injuries in rugby.
The main strengths of our study are as follows: (1) the sample size, the largest to date in systematic video analysis study of ACL injuries in rugby players; (2) the consecutive nature of the injuries analyzed; (3) the consistent biomechanical analysis with the use of measurement tools of 3 independent viewers; and (4) the field and match distribution data, never presented before in a consecutive series.
The results of this study should be interpreted in light of different limitations. First is the methodology used to identify ACL injuries, which was different from the gold standard of prospective studies with frequent contact with the teams. Second is the use of video analysis with assessment of biomechanics (kinematics) using video and tools, as opposed to the gold standard model-based image-matching technique, 24 which would have allowed a precise analysis of tibial rotations (that was not possible). However, the video analysis method is valid 23 and has been consistently adopted in many studies. # Third, we looked at male professional rugby players only, and the injury mechanism could be different in a lower level of sports or women’s rugby. Last, we did not have access to detailed data on concomitant injuries, which would have allowed coupling the injury mechanism to the knee injury pattern.
Conclusion
Almost 70% of ACL injuries in rugby occurred without a direct contact at knee level, predominantly during offensive situations, and through 3 main patterns: offensive COD, being tackled, and pressing/tackling. Biomechanically, most injuries involved a knee-dominant loading strategy accompanied by dynamic knee valgus. Improving the ability to maintain frontal and transverse plane control during COD tasks may aid in reducing ACL injury incidence in elite rugby. Accumulated fatigue does not appear to be a major risk factor for ACL injury in rugby players, as we found that the majority (>70%) of ACL injuries happened within 40 minutes of gameplay.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211048182.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211048182 for Systematic Video Analysis of Anterior Cruciate Ligament Injuries in Professional Male Rugby Players: Pattern, Injury Mechanism, and Biomechanics in 57 Consecutive Cases by Francesco Della Villa, Filippo Tosarelli, Rocco Ferrari, Alberto Grassi, Luca Ciampone, Gianni Nanni, Stefano Zaffagnini and Matthew Buckthorpe in Orthopaedic Journal of Sports Medicine
Acknowledgment
The authors acknowledge Simona Lucarno for the creation of Figure 5 and Niccolò Gaetaniello for the help with the collection of ACL injury videos.
Footnotes
Final revision submitted June 8, 2021; accepted June 16, 2021.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
- 1. Azubuike SO, Okojie OH. An epidemiological study of football (soccer) injuries in Benin City, Nigeria. Br J Sports Med. 2009;43(5):382–386. [DOI] [PubMed] [Google Scholar]
- 2. Benjaminse A, Webster KE, Kimp A, Meijer M, Gokeler A. Revised approach to the role of fatigue in anterior cruciate ligament injury prevention: a systematic review with meta-analyses. Sports Med. 2019;49(4):565–586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Bere T, Mok KM, Koga H, Krosshaug T, Nordsletten L, Bahr R. Kinematics of anterior cruciate ligament ruptures in World Cup alpine skiing: 2 case reports of the slip-catch mechanism. Am J Sports Med. 2013;41(5):1067–1073. [DOI] [PubMed] [Google Scholar]
- 4. Bittencourt NFN, Meeuwisse WH, Mendonça LD, Nettel-Aguirre A, Ocarino JM, Fonseca ST. Complex systems approach for sports injuries: moving from risk factor identification to injury pattern recognition—narrative review and new concept. Br J Sports Med. 2016;50:1309–1314. [DOI] [PubMed] [Google Scholar]
- 5. Boden BP, Sheehan FT, Torg JS, Hewett TE. Noncontact anterior cruciate ligament injuries: mechanisms and risk factors. J Am Acad Orthop Surg. 2010;18:520–527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Boden BP, Torg JS, Knowles SB, Hewett TE. Video analysis of anterior cruciate ligament injury: abnormalities in hip and ankle kinematics. Am J Sports Med. 2009;37:252–259. [DOI] [PubMed] [Google Scholar]
- 7. Bourne MN, Webster KE, Hewett TE. Is fatigue a risk factor for anterior cruciate ligament rupture? Sports Med. 2019;49:1629–1635. [DOI] [PubMed] [Google Scholar]
- 8. Brophy RH, Stepan JG, Silvers HJ, Mandelbaum BR. Defending puts the anterior cruciate ligament at risk during soccer: a gender-based analysis. Sports Health. 2015;7:244–249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Butler DL, Noyes FR, Grood ES. Ligamentous restraints to anteriorposterior drawer in the human knee: a biomechanical study. J Bone Joint Surg Am. 1980;62:259–270. [PubMed] [Google Scholar]
- 10. Dix C, Arundale A, Silvers-Granelli H, Marmon A, Zarzycki R, Snyder-Mackler L. Biomechanical measures during two sport-specific tasks differentiate between soccer players who go on to anterior cruciate ligament injury and those who do not: a prospective cohort analysis. Int J Sports Phys Ther. 2020;15(6):928–935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Cochrane JL, Lloyd DG, Buttfield A, Seward H, McGivern J. Characteristics of anterior cruciate ligament injuries in Australian football. J Sci Med Sport. 2007;10:96–104. [DOI] [PubMed] [Google Scholar]
- 12. Dallalana RJ, Brooks JH, Kemp SP, Willams AM. The epidemiology of knee injuries in English professional rugby union. Am J Sports Med. 2007;35:818–830. [DOI] [PubMed] [Google Scholar]
- 13. Della Villa F, Buckthorpe M, Grassi A, et al. Systematic video analysis of ACL injuries in professional male football (soccer): injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. Br J Sports Med. 2020;54(23):1423–1432. [DOI] [PubMed] [Google Scholar]
- 14. Dempsey AR, Lloyd DG, Elliot BC, Steele JR, Munro BJ. Changing sidestep cutting technique reduces knee valgus loading. Am J Sports Med. 2009;37:2194–2200. [DOI] [PubMed] [Google Scholar]
- 15. Doyle TLA, Schilaty ND, Webster KE, Hewett TE. Time of season and game segment is not related to likelihood of lower-limb injuries: a meta-analysis. Clin J Sport Med. 2021;31(3):304–312. [DOI] [PubMed] [Google Scholar]
- 16. Fox AS. Change-of-direction biomechanics: is what’s best for anterior cruciate ligament injury prevention also best for performance? Sports Med. 2018;48(8):1799–1807. [DOI] [PubMed] [Google Scholar]
- 17. Glassbrook DJ, Doyle TLA, Alderson JA, Fuller JT. The demands of professional rugby league match-play: a meta-analysis. Sports Med Open. 2019;5(1):24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Grassi A, Smiley SP, Roberti di Sarsina T, et al. Mechanisms and situations of anterior cruciate ligament injuries in professional male soccer players: a YouTube-based video analysis. Eur J Orthop Surg Traumatol. 2017;27:967–981. [DOI] [PubMed] [Google Scholar]
- 19. Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. Br J Sports Med. 2009;43:417–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Johnston JT, Mandelbaum BR, Schub D, Rodeo SA, Matava MJ, Silvers-Granelli HJ. Video analysis of anterior cruciate ligament tears in professional American football athletes. Am J Sports Med. 2018;46:862–868. [DOI] [PubMed] [Google Scholar]
- 21. Koga H, Nakamae A, Shima Y, Bahr R, Krosshaug T. Hip and ankle kinematics in noncontact anterior cruciate ligament injury situations: video analysis using model-based image matching. Am J Sports Med. 2018;46:333–340. [DOI] [PubMed] [Google Scholar]
- 22. Koga H, Nakamae A, Shima Y, et al. Mechanisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. Am J Sports Med. 2010;38:2218–2225. [DOI] [PubMed] [Google Scholar]
- 23. Krosshaug T, Nakamae A, Boden BP, et al. Mechanisms of anterior cruciate ligament injury in basketball: video analysis of 39 cases. Am J Sports Med. 2007;35:359–357. [DOI] [PubMed] [Google Scholar]
- 24. Krosshaug T, Nakamae A, Boden BP, et al. Estimating 3D joint kinematics from video sequences of running and cutting maneuvers—assessing the accuracy of simple visual inspection. Gait Posture. 2007;26:378–385. [DOI] [PubMed] [Google Scholar]
- 25. Marshall SW, Padua D, McGrath M. Incidence of ACL injury. In: American Orthopaedic Society for Sports Medicine; Hewett TE, Schultz SJ, Griffin LY, eds. Understanding and Preventing Noncontact ACL Injuries. Human Kinetics; 2007:5–29. [Google Scholar]
- 26. McLean SG, Huang X, Su A, Van Den Bogert AJ. Sagittal plane biomechanics cannot injure the ACL during sidestep cutting. Clin Biomech (Bristol, Avon). 2004;19:828–838. [DOI] [PubMed] [Google Scholar]
- 27. Montgomery C, Blackburn J, Withers D, Tierney G, Moran C, Simms C. Mechanisms of ACL injury in professional rugby union: a systematic video analysis of 36 cases. Br J Sports Med. 2018;52:994–1001. [DOI] [PubMed] [Google Scholar]
- 28. Olsen OE, Myklebust G, Engebretsen L, Bahr R. Injury mechanisms for anterior cruciate ligament injuries in team handball: a systematic video analysis. Am J Sports Med. 2004;32:1002–1012. [DOI] [PubMed] [Google Scholar]
- 29. Powers CM. The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther. 2010;40(2):42–51. [DOI] [PubMed] [Google Scholar]
- 30. Quatman CE, Quatman-Yates CC, Hewett TE. A “plane” explanation of anterior cruciate ligament injury mechanisms: a systematic review. Sports Med. 2010;40:729–746. [DOI] [PubMed] [Google Scholar]
- 31. Sheehan FT, Sipprell WH III, Boden BP. Dynamic sagittal plane trunk control during anterior cruciate ligament injury. Am J Sports Med. 2012;40:1068–1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Stuelcken MC, Mellifont DB, Gorman AD. Mechanisms of anterior cruciate ligament injuries in elite women’s netball: a systematic video analysis. J Sports Sci. 2016;34:1516–1522. [DOI] [PubMed] [Google Scholar]
- 33. Takazama Y, Ikeda H, Saita Y, et al. Return to play of rugby players after anterior cruciate ligament reconstruction using hamstring autograft: return to sports and graft failure according to age. Arthroscopy. 2017;33:181–189. [DOI] [PubMed] [Google Scholar]
- 34. van Mechelen W, Hlobil H, Kemper HC. Incidence, severity, aetiology and prevention of sports injuries: a review of concepts. Sports Med. 1992;14:82–99. [DOI] [PubMed] [Google Scholar]
- 35. Waldén M, Krosshaug T, Bjørneboe J, Andersen TE, Faul O, Hägglund M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: a systematic video analysis of 39 cases. Br J Sports Med. 2015;49:1452–1462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Withrow TJ, Huston LJ, Wojtys EM, Ashton-Miller JA. The relationship between quadriceps muscle force, knee flexion, and anterior cruciate ligament strain in an in vitro simulated jump landing. Am J Sports Med. 2006;34:269–274. [DOI] [PubMed] [Google Scholar]
- 37. Woods C, Hawkins R, Hulse M, Hodson A. The Football Association Medical Research Programme: an audit of injuries in professional football-analysis of preseason injuries. Br J Sports Med. 2002;36:436–441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Zhou J, Schilaty ND, Hewett TE, Bates NA. Analysis of timing of secondary ACL injury in professional athletes does not support game timing or season timing as a contributor to injury risk. Int J Sports Phys Ther. 2020;15(2):254–262. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211048182 for Systematic Video Analysis of Anterior Cruciate Ligament Injuries in Professional Male Rugby Players: Pattern, Injury Mechanism, and Biomechanics in 57 Consecutive Cases by Francesco Della Villa, Filippo Tosarelli, Rocco Ferrari, Alberto Grassi, Luca Ciampone, Gianni Nanni, Stefano Zaffagnini and Matthew Buckthorpe in Orthopaedic Journal of Sports Medicine