
FIGURE 1.
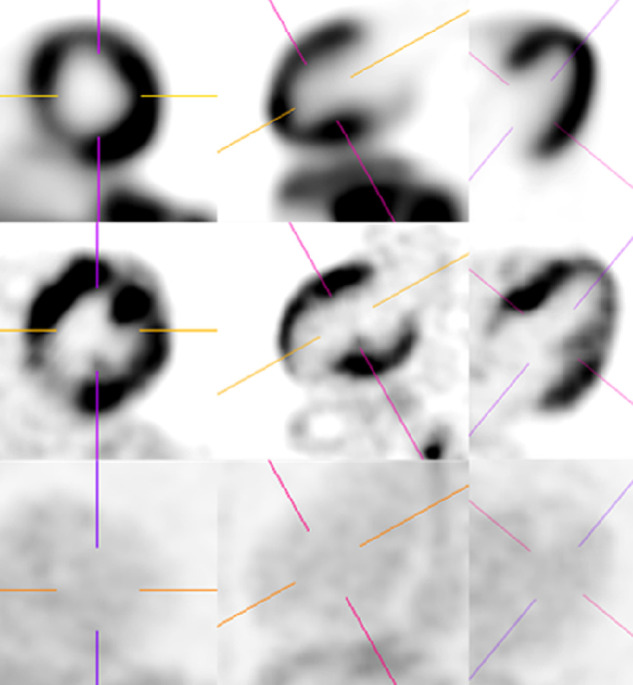
A 62-y-old woman with inferior wall motion abnormality, arrythmia, and an old outside PET/CT report raising suspicion of CS. Prior endomyocardial biopsy was negative; there was no pathologic or imaging proof of sarcoidosis elsewhere in the body. On the basis of clinical findings, patient was considered as presumably having CS and referred for PET/CT. First PET/CT was obtained with Diet-B (top: 13N-ammonia; middle: 18F-FDG/PET), which was reported as active CS with complete myocardial suppression. However, the observer evaluated as indeterminant secondary to partial suppression. Patient subsequently received steroids, and a follow-up study was performed with Diet-C (bottom). This time, both report and observer agreed that there was complete suppression with no active CS. While it is possible that this presumable CS case might have responded to treatment, it is also possible that the initial interpretation was incorrect, and patient might have received unnecessary treatment.