

Abstract
The knowledge, attitude, and practice of nurses in intensive care units (ICUs) are determinants for the efficacy of preventing the medical device–related pressure injury (MDRPI). The aim of this study was to determine the level and factors of knowledge, attitude, and practice of nurses' ICUs on preventing medical MDRPI in western China. An annual cross‐sectional study was conducted in hospitals of western China from May 2020 to September 2020. Nurses' knowledge and attitudes were assessed using Clinical Nurses Prevention MDRPI of Critically Ill Patients for the Knowledge, Attitude, Practice Assessment Scale. SPSS software version 25.0 and independent t‐test, Chi‐square, Fisher exact, one‐way analysis of variance, and multiple linear regression tests were used for data analysis. A total of 1002 nurses in ICUs from 37 hospitals in Gansu Province, China, participated in this study. The scores of overall KAP, knowledge, attitudes, and practice were 149.17 ± 24.62, 53.83 ± 12.23, 37.24 ± 6.35 and 58.10 ± 9.83, respectively. There was a positive and significant relationship between three variables. Findings revealed that nurses' knowledge score in the Tertiary hospital was higher than scores of other hospitals as 3.840 units. Moreover, the knowledge score and practice score of nurses with bachelor's degree or above were higher than other nurses and are 0.978 and 1.106 units, respectively. Based on the findings, practice of nurses increased by 0.992 units, with a 1‐year increase in work experience of nurses in the ICU. The levels of knowledge, attitude, and practice of nurse in ICUs on preventing MDRPI were acceptable. The findings of the study highlight that a comprehensive approach should be conducted for raising the level of knowledge, attitude, and practice of nurses' ICUs on preventing medical MDRPI, as well as improving the quality of care for critically ill patients.
Keywords: attitude, knowledge, medical devices, practice, pressure injury
1. INTRODUCTION
Medical device–related pressure injury (MDRPI) is a common and important problem occurring in all health care around the world. The National Pressure Ulcer Advisory Panel (NPUAP) proposed the conception of MDRPI, and defined it as pressure injuries caused by medical devices for diagnosis or treatment, the shape of the damaged part is consistent with the shape of the medical device. 1 In addition, the results of previous studies also suggested that pressure injury can develop in any tissue exposed to pressure and that medical devices pose a substantial risk for their formation. 2
The patients in intensive care units (ICUs) have a higher risk of developing MDRPI due to the widespread use of medical devices for diagnosis and treatment. 3 The results of a point prevalence and cross‐sectional study (N = 2240) reported that the prevalence of MDRPI with patients in ICU was 1.65%. 4 According to the results of the 2009 International Pressure Ulcer Prevalence Survey, the prevalence rate of pressure injury in the ICU was 12.1%, and it occupied the highest rate of hospital‐associated pressure injury. 5 In a systematic review and meta‐analysis, the most frequent MDRPI anatomic sites were the head and face of about 51%, and the other anatomic sites including the lower extremities such as the pelvic area, the upper extremities, and the back and the prevalence rate of pressure injury were 27%, 7.5%, 3.0%, and 1.5%, respectively. 6 In addition, prior studies concluded that MDRPI not only directly increases the rate of infection but also decreases the quality of life and increases additional medical expense for patients in ICU. 7 , 8
Basic knowledge, positive attitude, and correct practice are necessary to improve the quality and safety of nursing care. A few investigations have been performed on preventing pressure injury knowledge, attitudes, and practice among nurses. 9 , 10 Lotfi et al 11 concluded that nurse's knowledge and attitude levels regarding pressure injury were relatively low; however, their practice towards preventing pressure injury were quietly acceptable. A multicentre cross‐sectional study reported that nursing students' knowledge on pressure ulcer prevention was relatively low. 10 However, Apold et al concluded that nurse's knowledge and attitude about the MDRPI could impact the practice of preventing measures. 12 A nurse's knowledge and attitude plays an important role in preventing pressure injury. The results of prior studies reported that nurses in ICUs lack the knowledge of preventing pressure injury could incur the prevalence of MDRPI. 13
In recent years, the relationships among nurse characteristics, PI knowledge, and reported practices were mostly explored by prior studies. 13 In case of Turkey, the importance of training activities related to pressure injury management has been emphasised in the last 15 years. However, rarely scholars focus on the relationships among the knowledge, attitude, and practice of nurses in ICU. The prior studies related to the MDRPI that more focused on the analysis of the reason of developing into MDRPI and the development and application of risk assessment scales of MDRPI. 14 , 15 Hence, the present study sought to investigate the level and factors of knowledge, attitude, and practice of nurses' ICUs on preventing medical MDRPI in western China.
2. MATERIALS AND METHODS
2.1. Samples and setting
A multicentric cross‐sectional study was performed from May 2020 to September 2020 with a random sampling approach in 37 hospitals in Gansu Province, China. Previous study have examined samples of nurses in ICU using the same instrument and reported the scoring rate of prevention of MDRPI was 72.07%. 16 Based on the simple random sampling formula, n = t 2 α PQ/δ 2, the absolute allowable error was δ 0.03, assuming the probability of type I error α = 0.05, Z 0.05 = 1.96, and the P value of .7207; the required sample size of 947 was calculated eventually. After screening the nurses for inclusion and exclusion criteria, a total of 1002 nurses were enrolled into the study by random sampling method (Figure 1).
FIGURE 1.
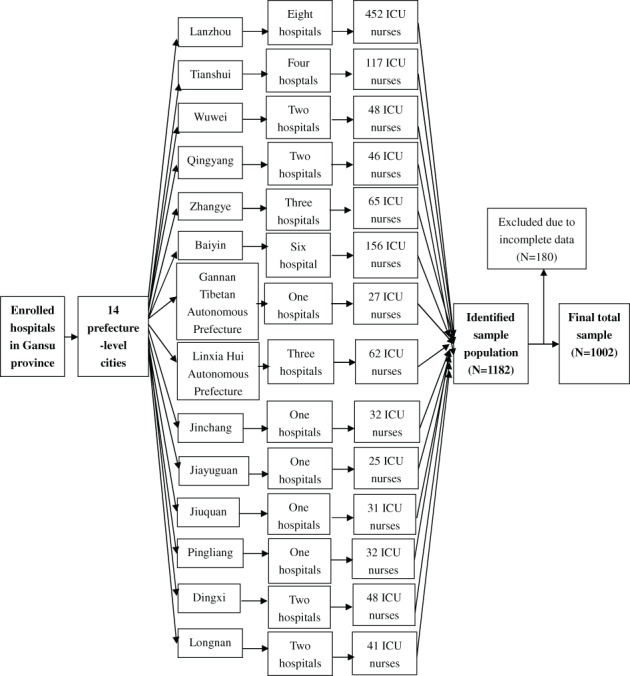
Flowchart of intensive care unit nurse sample selection in hospitals in Gansu Province, China
All participants met the following inclusion criteria: (a) currently working in the ICU ≥ 1 year; (b) obtaining a Nursing Practice Certificate issued by the Ministry of Health of China; and (c) volunteer to take part in the study. Nurses who did not accept to participate or who do not sign the informed consent were excluded.
2.2. Data collection instruments
“The knowledge, attitude, practice assessment scale for prevention MDRPI in clinical nurses” 17 was used to investigate the level and factors of knowledge, attitude, and practice of nurses' ICUs on preventing medical MDRPI in western China. The scale consists of four sections incorporating demographic information and three questionnaires. It can evaluate the knowledge, attitude, and practice of clinical nurses in the prevention of MDRPI. The total score of the scale was 38 ~ 190 points, the higher the score, the higher the level of the clinical nurses' MDRPI prevention of critically ill patients for the knowledge, attitude, practice. Section 1 discusses the demographic information of the scale including age, gender, highest educational attainment, work experiences, position, level of hospital, type of hospital, and type of department.
Section 2 discusses nurse's knowledge on preventing MDRPI: this questionnaire consists of 15 multiple choice items related to MDRPI prevention with five alternate responses. The 15 items reflect nine themes: definition, risk factors, assessment tools, prevention strategies, operating specifications, stage of MDRPI prevention trainings received, experience of nursing patients with MDRPI, and the often common locations for these MDRPIs. The responses were presented on a 5‐point Likert‐type scale, with responses ranging from 1 “unknown” to 5 “well aware”, and the answer was scored 1 ~ 5, respectively. A maximum score of 75 is possible.
Section 3 discusses nurse's attitude towards MDRPI prevention: this questionnaire consists of nine items that measure attitudes towards MDRPI prevention. The nine items reflect four themes: responsibility for MDRPI prevention, confidence in the effectiveness of MDRPI prevention, attitude in taking part in the education program of knowledge on preventing MDRPI, and significance of MDRPI prevention. The instrument includes five subscales that use a 5‐point Likert scale (1 = strongly disagree to 5 = strongly agree). Higher scores indicated more positive attitudes.
Section 4 discusses nurses' practice on preventing MDRPI: this questionnaire consists of 14 items that practice on MDRPI prevention. The nine items reflect four themes: skin assessment, take measures on MDRPI prevention, feedback the occurrence of MDRPI to the nursing department leaders, and nursing records. The responses were presented on a 5‐point Likert‐type scale, with responses ranging from 1 “never done” to 5 “often”, the answer was scored 1–5, respectively. Higher scores indicated more positive practice.
2.3. Data collection
In the study, the electronic questionnaires were used to collect data. First is to obtain the consent of the nursing department leaders in each hospital. Second, researcher would communicate with each department head nurse about the purpose of the survey and the principle of anonymous survey completion. Finally, after obtaining informed consent from the nurses, each department head nurse sent an electronic questionnaire with an attached consent page to all eligible nurses in their department and asked the nurses to complete the survey with their mobile phones.
2.4. Data analysis
In this study, the continuous variables were described by means and deviation, reported as mean ± SD, while categorical variables were summarised by frequency and percentage. The rate of scores of total and each dimension = mean scores/theoretical maximum × 100%.
The independent t‐test and one‐way ANOVA was performed to examine differences between MDRPI prevention scales and demographic information. Scheffe's test was adopted as post‐test of one‐way ANOVA. Pearson correlation coefficient was used to examine the relationship between knowledge, attitude, and practice. Multiple linear regression analysis was adopted to analyse data after the results of ANOVA were statistically significant. Additionally, multiple linear regression model enter method was applied to determine which of the demographic variables had the most effect on each of the variables of knowledge, attitude, and practice. Independent variables were also introduced into a regression model that was significant by univariate analysis. Categorical variables were transformed into dummy variables.
All data were analysed using the IBM SPSS Statistics for Windows (SPSS, ver. 25.0). The P value of ≤.05 indicated to be of statistical significance.
2.5. Ethical considerations
The study was approved by our university's Institutional Review Board (IRB) before data collection began. All participations in the study were voluntary.
3. RESULTS
Thirty‐seven hospitals that offer nurses in ICUs agreed to participate in the study, and a total of 1002 nurses completed the questionnaire. The median age of participants was 23.97 ± 4.90 years. Most participants were female (94.7%), while the male only occupied 5.3%. The largest proportion of nurses' highest educational attainment were bachelor degree (59.4%) and the smallest proportion were postgraduate or above (1.7%). In addition, 46.5% of participants had 11 to 15 years of clinical work experience, 66.7% worked in tertiary hospital, and the most common clinical units were in general ICUs, approximately occupied 51.7%. Overall, in the aspect of position and technical title of the participants, 93.4% ICU nurses were the general nurse, and 48.2% had the technical title of Senior nurse. The results are shown in Table 1.
TABLE 1.
Demographic characteristics correlation with knowledge, attitude, and practice in the area of MDRPI prevention (N = 1002)
| Variable | Frequency (%) | Knowledge | Attitude | Practice | |||
|---|---|---|---|---|---|---|---|
| Mean ± SD | Test results | Mean ± SD | Test results | Mean ± SD | Test results | ||
| Age | |||||||
| ≤25 | 169 (16.9) | 50.72 ± 10.22 | F = 5.73 | 35.33 ± 6.3 | F = 11.40 | 57.15 ± 9.70 | F = 2.03 |
| 26 to 30 | 507 (50.6) | 53.82 ± 12.59 | P < .001 | 37.09 ± 6.45 | P < .001 | 57.85 ± 10.15 | P = .11 |
| 31 to 35 | 224 (22.4) | 55.29 ± 12.47 | 37.89 ± 6.21 | 58.52 ± 9.22 | |||
| ≥36 | 102 (10.1) | 55.84 ± 12.06 | 39.7 ± 5.24 | 59.99 ± 9.6 | |||
| Mean ± SD | 23.97 ± 4.90 | ||||||
| Gender | |||||||
| Male | 53 (5.3) | 56.02 ± 11.34 | t = 1.339 | 37.35 ± 6.35 | t = −0.28 | 60.02 ± 10.30 | t = 1.462 |
| Female | 949 (94.7) | 53.71 ± 12.27 | P = .181 | 37.24 ± 6.35 | P = .78 | 57.99 ± 9.80 | P = .144 |
| Level of hospital | |||||||
| Tertiary hospital | 668 (66.7) | 56.06 ± 11.74 | t = 8.379 | 38.03 ± 6.14 | t = 5.666 | 59.24 ± 9.47 | t = 5.265 |
| Secondary hospital | 334 (33.3) | 49.38 ± 11.98 | P < .001 | 35.65 ± 6.48 | P < .001 | 55.81 ± 10.15 | P < .001 |
| Type of ICU | |||||||
| General ICU | 518 (51.7) | 54.05 ± 12.01 | t = 0.591 | 53.83 ± 12.23 | t = −0.488 | 58.15 ± 9.70 | t = 0.166 |
| Specialist ICU | 484 (48.3) | 53.60 ± 12.47 | P = .555 | 37.14 ± 6.12 | P = .626 | 58.05 ± 9.98 | P = .868 |
| Type of hospital | |||||||
| General hospital | 975 (97.3) | 54.00 ± 12.21 | t = 2.648 | 37.32 ± 6.32 | t = 2.414 | 58.15 ± 9.82 | t = 1.025 |
| Specialist hospital | 27 (2.7) | 47.70 ± 11.52 | P = .008 | 34.33 ± 6.95 | P = .016 | 56.19 ± 10.34 | P = .305 |
| Work experiences | |||||||
| ≥21 years | 35 (3.5) | 55.77 ± 14.04 | F = 5.78 | 39.23 ± 5.11 | F = 10.99 | 57.86 ± 11.63 | F = 2.61 |
| 16 to 20 years | 169 (16.9) | 56.88 ± 11.83 | P = .001 | 39.33 ± 5.74 | P < .001 | 59.91 ± 9.39 | P = .049 |
| 11 to 15 years | 466 (46.5) | 53.72 ± 12.52 | 37.12 ± 6.49 | 58.01 ± 9.56 | |||
| ≤5 years | 332 (33.1) | 52.23 ± 11.54 | 36.13 ± 6.29 | 57.33 ± 10.14 | |||
| Mean ± SD | 3.09 ± 0.79 | ||||||
| Highest educational attainment | |||||||
| Postgraduate or above | 17 (1.7) | 45.59 ± 13.91 | F = 15.254 | 38.77 ± 6.59 | F = 21.186 | 52.47 ± 12.67 | F = 17.636 |
| Bachelor degree | 595 (59.4) | 55.76 ± 11.80 | P < .001 | 38.46 ± 5.86 | P < .001 | 59.78 ± 8.90 | P < .001 |
| Three‐year college education | 365 (36.4) | 51.59 ± 12.16 | 35.38 ± 6.64 | 56.10 ± 10.32 | |||
| Secondary vocational school education | 25 (2.5) | 46.44 ± 12.16 | 34.20 ± 6.04 | 51.20 ± 10.24 | |||
| Position | |||||||
| Nurse | 936 (93.4) | 53.74 ± 12.38 | t = −0.928 | 37.09 ± 6.41 | t = −2.762 | 58.10 ± 9.88 | t = −0.45 |
| Head nurse | 66 (6.6) | 55.18 ± 9.75 | P = .353 | 39.32 ± 5.14 | P = .006 | 58.15 ± 9.21 | P = .964 |
| Technical title | |||||||
| Nurse | 382 (38.1) | 52.09 ± 12.13 | F = 5.78 | 35.79 ± 6.33 | F = 17.19 | 56.92 ± 10.29 | F = 6.42 |
| Senior nurse | 483 (48.2) | 54.37 ± 12.14 | P < .001 | 37.57 ± 6.43 | P < .001 | 58.4 ± 9.63 | P < .001 |
| Supervisor nurse | 127 (12.7) | 56.98 ± 12.34 | 40.19 ± 4.85 | 60.90 ± 8.38 | |||
| Associate chief nurse or above | 10 (1.0) | 53.90 ± 9.18 | 38.80 ± 4.98 | 53.00 ± 10.65 | |||
Abbreviations: ICU, intensive care unit; MDRPI, medical device–related pressure injury.
The total scores of 1002 ICU nurses were 149.17 ± 24.62, the rate of score was 82.87%. Although the scores of knowledge, attitude, and practice on preventing MDRPI were 53.83 ± 12.23, 37.24 ± 6.35, and 58.10 ± 9.83, the rate of scores were 82.81%, 82.76%, and 83%, respectively. Multiple choice questions have the three items with the lowest scores in each dimension of the knowledge, attitude, and practice assessment scale for prevention, and the participant responses are shown in Table 2.
TABLE 2.
The three items with the lowest scores in each dimension of the knowledge, attitude, and practice assessment scale for prevention of MDRPI in clinical nurses
| Dimension | Items | Scores |
|---|---|---|
| knowledge | K10. You take the initiative to learn knowledge of MDRPI | 3.45 ± 1.033 |
| K11. You have participated in academic lectures or trainings on MDRPI | 3.14 ± 1.148 | |
| K12. You have taken care for patients with MDRPI | 3.06 ± 1.182 | |
| Attitude | A4. Continuous evaluation helps to prevent the prevalence of MDRPI | 4.12 ± 0.820 |
| A7. MDRPI is an indicator to measure the quality of care | 4.04 ± 0.827 | |
| A3. Most MDRPI can be avoided | 4.02 ± 0.870 | |
| Practice | P13. There are records of taking measures to relieve local pressure in the records of care for patients with using medical devices | 4.06 ± 0.930 |
| P5. For patients who use masks to inhale oxygen, you will take preventive measures in the bridge of the patient's nose | 4.06 ± 0.882 | |
| P10. Feedback the prevalence of MDRPI and occurrence of general pressure injuries to the nursing department leaders separately | 3.92 ± 1.066 |
Abbreviation: MDRPI, medical device–related pressure injury.
According to the results of one‐way ANOVA (Table 1), there was a vital relationship between age and knowledge (P < .001). Based on the results of the Scheffe's test, there was an obvious difference about knowledge score between ages of ≤25 years and those of 26 to 30 years (P = .041), 31 to 35 years (P = .003), and ≥36 years (P = .010). The knowledge score in age with ≤25 years was significantly lower. Independent t‐test results showed that there was a significant relationship between the knowledge and level of hospital of the nurses in the ICU. Knowledge about the MDRPI prevention in subjects with tertiary hospital was significantly higher (P < .001). There was also an obvious difference in terms of knowledge and type of hospital of the nurses in the ICU. Knowledge about the MDRPI prevention in subjects with general hospital was significantly higher (P = .008). Moreover, based on the results of one‐way ANOVA, there was a statistically significant difference between knowledge and work experience of nurses (P = .001). Scheffe's test results showed that subjects with work experience 16 to 20 years in ICUs were more knowledgeable than less than 5 years (P < .001) and 11 to 15 years (P = .004). Based on the results of one‐way ANOVA, there was a significant relationship between knowledge and highest educational attainment of nurses (P < .001) and technical title of nurses (P < .001). Scheffe's test consequences also demonstrated that knowledge about the MDRPI prevention in subjects with bachelor degree was obviously higher (P < .001), and senior nurse was more knowledgeable than nurse (P < .001).
Based on the results of independent t‐test results (Table 1), there was a statistically significant difference between the level of hospital and attitude of nurses (P < .001), and the attitude of nurses in tertiary hospital was significantly higher than that of nurses in secondary hospital. Besides, independent t‐test results also demonstrated that there was a significant difference in attitude between nurses employed in the general hospital and those in other hospitals (P = .016). Independent t‐test findings also demonstrated that there was an obvious difference between nurses' attitude and position (P = .006), head nurse's attitude was significantly higher than other nurses. One‐way ANOVA results (Table 1) showed that there was a significant relationship between age and attitude (P < .001). The consequences of the Scheffe's test reported that there was an obvious difference about attitude score between age of ≤25 years and that of 26 to 30 years (P = .019), 31 to 35 years (P = .001), and ≥36 years (P < .001). The attitude score in age with ≤25 years was significantly negative. Similarly, as shown in Table 1, there was an obvious difference between attitude and work experience of ICU nurses (P < .001). Scheffe's test results demonstrated that there was a significant relationship between the attitudes of ICU nurses with 16 to 20 years of work experience and those with 11 to 15 years of work experience (P < .001) and ≤25 years of work experience (P < .001); attitude scores were higher in subjects with 16 to 20 years of work experience. Moreover, there was an obvious difference between the attitude and technical title of the ICU nurses (P < .001). Based on the consequences of Scheffe's test, attitudes of subjects with supervisor nurses were significantly more than nurse (P < .001) and senior nurse (P < .001).
What is more, the results of independent t‐test (Table 1) demonstrated that there was an obvious difference between level of hospital and practice of nurses (P < .001), and practice of nurses in tertiary hospital was significantly higher than that of nurses in secondary hospital. One‐way ANOVA results (Table 1) showed that there was an obvious difference between work experience and practice (P = .049). Moreover, one‐way ANOVA results (Table 1) also showed that there was an obvious difference between the practice and technical title of the nurses in ICU (P < .001). Scheffe's test results demonstrated that practice of subjects with senior nurses was significantly more than nurse (P < .001). The three items with the lowest scores in each dimension of the knowledge, attitude, and practice assessment scale for MDRPI prevention in clinical nurses are shown in Table 2.
What is more, the results of correlation of knowledge, attitude, and practice related to MDRPI prevention of nurses in ICU are shown in Table 3. There was an obvious and positive relationship between knowledge and attitude (r = 0.571, P < .001). By increasing the knowledge score, attitude scores were also increased. At the same time, knowledge and practice also had an obvious and positive relationship (r = 0.603, P < .001), which reported that increased knowledge score would increase practice score. At the same time, attitude and practice had an obvious and positive relationship (r = 0.689, P < .001), which reported that increased attitude score would increase practice score.
TABLE 3.
Correlation of knowledge, attitude, and practice related to prevention MDRPI of nurses in ICU
| Scores of knowledge | Scores of attitude | Scores of practice | |
|---|---|---|---|
| Scores of knowledge | |||
| Pearson's correlation | 1 | 0.571** | 0.603** |
| Sig. | 0.000 | 0.000 | |
| N | 1002 | 1002 | 1002 |
| Scores of attitude | |||
| Pearson's correlation | 0.571** | 1 | 0.689** |
| Sig. | 0.000 | 0.000 | |
| N | 1002 | 1002 | 1002 |
| Scores of practice | |||
| Pearson's correlation | 0.603** | 0.689** | 1 |
| Sig. | 0.000 | 0.000 | |
| N | 1002 | 1002 | 1002 |
Abbreviations: ICU, intensive care unit; MDRPI, medical device–related pressure injury.
Note: ** P < .01.
As shown in Table 4, the variables of level of hospital, scores of attitude, and scores of practice were associated with ICU nurses' knowledge in the study. The knowledge scores of tertiary hospital were higher than that of secondary hospital ICU nurses by 3.84 units, and with one unit increase in the attitude score of ICU nurses, nurses' knowledge was increased by 0.523 units. When the practice score of ICU nurses increased by one unit, nurses' knowledge was increased by 0.489 units.
TABLE 4.
The results of linear regression analysis to investigate the effect of demographic characteristics on ICU nurses' knowledge about prevention of MDRPI (N = 1002)
| Independent variables | B coefficient | Standard coefficient | β‐value | Statistics | P‐value |
|---|---|---|---|---|---|
| Age | 0.046 | 0.52 | .003 | 0.089 | .929 |
| Work experiences | −1.036 | 0.555 | −.067 | −1.868 | .062 |
| Level of hospital | 3.84 | 0.671 | .148 | 5.726 | .000 |
| Technical title | −1.358 | 1.071 | −.037 | −1.268 | .205 |
| Highest educational attainment | −0.442 | 0.677 | −.018 | −0.653 | .514 |
| Type of hospital | −1.256 | 0.671 | −.088 | −1.468 | .075 |
| Scores of attitude | 0.523 | 0.065 | .272 | 8.055 | .000 |
| Scores of practice | 0.489 | 0.041 | .393 | 11.835 | .000 |
Abbreviations: ICU, intensive care unit; MDRPI, medical device–related pressure injury.
Table 5 shows that the variables of highest educational attainment, scores of knowledge, and scores of practice were associated with ICU nurses' attitude in this study. The attitude score of bachelor degree was higher than that of other nurses, and with one unit increase in the knowledge score of ICU nurses, nurses' attitude was increased by 0.118 units. When the practice score of ICU nurses increased by one unit, nurses' attitude was increased by 0.343 units.
TABLE 5.
The results of linear regression analysis to investigate the effect of demographic characteristics on ICU nurses' attitude about prevention of MDRPI (N = 1002)
| Independent variables | B coefficient | Standard coefficient | β‐value | Statistics | P value |
|---|---|---|---|---|---|
| Age | 0.223 | 0.252 | .03 | 0.886 | .376 |
| Work experiences | −0.171 | 0.267 | −.021 | −0.639 | .523 |
| Level of hospital | 0.062 | 0.328 | .005 | 0.191 | .849 |
| Type of hospital | 0.959 | 0.612 | .05 | 1.568 | .117 |
| Technical title | −1.158 | 0.613 | −.045 | −1.89 | .059 |
| Position | 0.868 | 0.515 | .042 | 1.348 | .094 |
| Highest educational attainment | 0.978 | 0.327 | .074 | 2.992 | .003 |
| Scores of knowledge | 0.118 | 0.014 | .226 | 8.123 | .000 |
| Scores of practice | 0.343 | 0.018 | .53 | 19.402 | .000 |
Abbreviations: ICU, intensive care unit; MDRPI, medical device–related pressure injury.
As shown in Table 6, the variables of highest educational attainment, work experiences, scores of knowledge, and scores of practice were associated with ICU nurses' practice in the present study. The practice score of bachelor degree was higher than other nurses, and with a 1‐year increase in the work experience of ICU nurses, nurses' practice related to prevention of MDRPI was increased by 0.992 unit. What is more, ICU nurses' knowledge score increased by one unit, and the nurses' practice score was increased by 0.253 units. When the attitude score of ICU nurses increased by one unit, nurses' practice was increased by 0.792 units.
TABLE 6.
The results of linear regression analysis to investigate the effect of demographic characteristics on ICU nurses' practice about prevention of MDRPI (N = 1002)
| Independent variables | B coefficient | Standard coefficient | β‐value | Statistics | P value |
|---|---|---|---|---|---|
| Level of hospital | −0.531 | 0.488 | −.026 | −1.088 | .277 |
| Work experiences | 0.992 | 0.318 | .08 | 3.121 | .002 |
| Technical title | 0.526 | 0.745 | .018 | 0.706 | .481 |
| Highest educational attainment | 1.106 | 0.484 | .055 | 2.286 | .022 |
| Scores of knowledge | 0.253 | 0.021 | .314 | 11.848 | .000 |
| Scores of attitude | 0.792 | 0.041 | .512 | 19.275 | .000 |
Abbreviations: ICU, intensive care unit; MDRPI, medical device–related pressure injury.
4. DISCUSSION
According to the results of the present study, the score rate of knowledge of ICU nurses on preventing MDRPI was 82.81%, and the level of knowledge was acceptable. The results of this study were similar to other prior studies. 18 , 19 Kaddourah et al 18 reported that the knowledge score of preventing pressure injury was at an acceptable level. In addition, Strand and Lindgren 19 also reported that knowledge of pressure injury was adequate. However, prior studies have shown that the knowledge of the nurses related to the prevention of pressure injury was unfavourable. 20 , 21 The reason of causing the difference in the results of the present study and other studies may be summarised as the following: first, the level of knowledge of nurses regarding the prevention pressure injury was assessed by different instruments. Second, whether the nurses received the education programme was an important factor affecting the level of knowledge.
According to the results of the present study, ICU nurses' attitudes toward the pressure injury were acceptable. Obviously, knowledge of nurses regarding the prevention pressure injury can affect the nurses' attitude. 7 , 8 The results of the present study also suggested that there was a positive correlation between knowledge, attitude, and practice of preventing pressure injury. Moreover, the results of a cross‐sectional study conducted by Khojastehfar 20 demonstrated that an undesirable level of knowledge towards pressure injury prevention was related to the nurses' negative attitude regarding the pressure injury prevention. According to the results of abovementioned studies, education program of nurse's knowledge regarding prevention pressure injury should be paid more attention by authorities. Furthermore, the nurse's attitude of preventing pressure injury may be associated with these factors, such as facilities and equipment, facility policies, and healthcare policy. 22
The results of the study showed that the nurse's practice was also desirable. Meanwhile, according to the results of the present study, the adequate knowledge and positive attitude towards prevention pressure injury were related to the desirable practice regarding prevention pressure injury. In contrary to the present study, prior studies have shown that the knowledge and practice of the nurses related to the prevention of pressure injuries were unsatisfactory, but the practice of preventing pressure injuries was acceptable. 20 , 21 A study conducted by Khojastehfar 20 reported that the results of practice of preventing pressure injury in contrary to their knowledge and attitude regarding prevention of pressure injury can be associated with tool used in the study. In addition, the mean MDRPI prevention practice score in the present study was obviously higher than results demonstrated in other studies. 16 , 23 Meanwhile, the nurses' practice score was the highest compared to the score of knowledge and attitude in this study, which might be related to the increasing focus on pressure injury prevention in Chinese medical departments in recent years.
Based on the results of the present study, nurses' knowledge towards to prevention of MDRPI in tertiary hospital was higher than scores of other hospitals and it is 3.840 units, which might be because the head of tertiary hospital pays more attention to the nurses' education training to increase the nurses' knowledge with regard to MDRPI. Meanwhile, the scores of attitude and practice were higher, the nurses' knowledge was more adequate. In other words, a positive attitude and practice also promote an increase in nurses' knowledge. However, there was no relationship between nurses' highest educational attainment and knowledge score in the present study. The result of the study was in contrary with previous studies. Khojastehfar et al 20 and Jiang et al 24 suggested that nurses with higher educational attainment were more likely to have adequate MDRPI prevention knowledge than those with a lesser degree/certificate. The reason for this contrary result may also be related to the fact that some Chinese nurses study a bachelor's degree part‐time instead of taking a full‐time bachelor's degree program, while the level of initial nurse educational attainment were usually low. 24 , 25
The results of this study demonstrated that nurses' highest educational attainment was related to the attitude of MDRPI prevention, while nurses with bachelor's degree or above show higher results than other nurses by 0.978 units. On the one hand, nurses with high educational attainment in the hospital have more chance to participate in the education training that gives more awareness about the damage of MDRPI for patients. A descriptive cross‐sectional study conducted by Lotfi et al 11 showed that relevant training program could improve nurses' attitude regarding the prevention of MDRPI. On the other hand, the results might be associated with the issue of social desirability. More attention and learning opportunities tend to give the nurses with high educational attainment. Therefore, nurses with high educational attainment usually tend to have a positive attitude facing their work, and hope that their attitude and practice deserve social desirability and have a positive load concerning patients' care. 20
The results of the present study demonstrated that nurses' practice was improved by an increase in work experience. The results were similar to those of previous studies. Based on the results of the study by Barakat‐Johnson, 26 it is suggested that more work experience helped the nurses to increase their knowledge. What is more, there was a significant association between knowledge towards the prevention of MDRPI and practice regarding the prevention of MDRPI. Similarly, Khojastehfar et al 20 reported that positive attitude and better practice towards prevention of MDRPI of nurses in ICUs might be related to the fact that the nurse worked longer in hospital. In addition, the present study also demonstrated that there was a positive relationship between nurse with highest educational attainment, knowledge on prevention of MDRPI, and practice.
5. CONCLUSION
MDRPI was a serious, preventable, and common medical problem in the ICU department. The aim of this study was to investigate the level of Chinese nurses' knowledge, attitude, and practice towards prevention of MDRPI. Generally, the scores of nurses' knowledge, attitude, and practice of preventing MDRPI were acceptable. What is more, the results of cross‐sectional study indicated that nurses' highest educational attainment was related to the attitude and practice on prevention of MDRPI; however, the relationship between knowledge and Chinese nurse's highest educational attainment needs to be further studied. In addition, the present study also reported that education training would have a positive effect on nurse's knowledge, attitude, and practice of preventing MDRPI. Hence, the results of this study suggested that developed educational programmes for the prevention of MDRPI and managing care services for patients at risk of developing the MDRPI were important measures to decrease the prevalence of MDRPI.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
ACKNOWLEDGEMENTS
The authors wish to thank all ICU nurses who participated in this study. This study was funded by Health Industry Research Project of Gansu Province of China (GSWSKY‐2019‐103), Lanzhou Science and Technology Plan Project (2019SHFZ0019), and Longyuan Youth Innovation and Entrepreneurship Team Project (201807) .
Zhang Y‐B, He L, Gou L, et al. Knowledge, attitude, and practice of nurses in intensive care unit on preventing medical device–related pressure injury: A cross‐sectional study in western China. Int Wound J. 2021;18:777–786. 10.1111/iwj.13581
Ya‐Bin Zhang and Li He contributed equally as co‐first authors to this work.
Funding information Health Industry Research Project of Gansu Province of China, Grant/Award Number: GSWSKY‐2019‐103; Lanzhou Science and Technology Plan Project, Grant/Award Number: 2019SHFZ0019; Longyuan Youth Innovation and Entrepreneurship Team Project, Grant/Award Number: 201807
DATA AVAILABILITY STATEMENT
date available
REFERENCES
- 1. Kottner J, Cuddigan J, Carville K, et al. Prevention and treatment of pressure ulcers/injuries: the protocol for the second update of the international clinical practice guideline 2019. J Tissue Viability. 2019;28(2):51‐58. [DOI] [PubMed] [Google Scholar]
- 2. Karadag A, Hanönü SC, Eyikara E. A prospective, descriptive study to assess nursing staff perceptions of and interventions to prevent medical device‐related pressure injury. Ostomy Wound Manage. 2017;63(10):34‐41. [PubMed] [Google Scholar]
- 3. Flodgren, G. , Conterno, L.O. , Mayhew, A. , Omar, O. , Pereira, C.R. , Shepperd, S. , 2013. Interventions to improve professional adherence to guidelines for prevention of device‐related infections. Cochrane database Syst rev (3), Cd006559. [DOI] [PubMed]
- 4. Liu Y, Li T, Fu C, Zhou X, Jiang Q. Causes and solution of medical‐devices‐related pressure ulcer in intensive care unit. Chin J Modern Nurs. 2014;20(11):1252‐1254. [Google Scholar]
- 5. Edger M. Effect of a patient‐repositioning device in an intensive care unit on hospital‐acquired pressure injury occurences and cost: a before‐after study. J Wound Ostomy Continence Nurs. 2017;44(3):236‐240. [DOI] [PubMed] [Google Scholar]
- 6. Kayser SA, VanGilder CA, Ayello EA, Lachenbruch C. Prevalence and analysis of medical device‐related pressure injuries: results from the international pressure ulcer prevalence survey. Adv Skin Wound Care. 2018;31(6):276‐285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Beeckman D, Defloor T, Demarré L, Van Hecke A, Vanderwee K. Pressure ulcers: development and psychometric evaluation of the attitude towards pressure ulcer prevention instrument (APuP). Int J Nurs Stud. 2010a;47(11):1432‐1441. [DOI] [PubMed] [Google Scholar]
- 8. Beeckman D, Vanderwee K, Demarré L, Paquay L, Van Hecke A, Defloor T. Pressure ulcer prevention: development and psychometric validation of a knowledge assessment instrument. Int J Nurs Stud. 2010b;47(4):399‐410. [DOI] [PubMed] [Google Scholar]
- 9. Florin J, Bååth C, Gunningberg L, Mårtensson G. Attitudes towards pressure ulcer prevention: a psychometric evaluation of the Swedish version of the APuP instrument. Int Wound J. 2016;13(5):655‐662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Simonetti V, Comparcini D, Flacco ME, Di Giovanni P, Cicolini G. Nursing students' knowledge and attitude on pressure ulcer prevention evidence‐based guidelines: a multicenter cross‐sectional study. Nurse Educ Today. 2015;35(4):573‐579. [DOI] [PubMed] [Google Scholar]
- 11. Lotfi M, Aghazadeh AM, Asgarpour H, Nobakht A. Iranian nurses' knowledge, attitude and behaviour on skin care, prevention and management of pressure injury: a descriptive cross‐sectional study. Nurs Open. 2019;6(4):1600‐1605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Apold J, Rydrych D. Preventing device‐related pressure ulcers: using data to guide statewide change. J Nurs Care Qual. 2012;27(1):28‐34. [DOI] [PubMed] [Google Scholar]
- 13. Gu Y, Li WR. Analysis on the knowledge, attitude and practice current situation and influencing factors of ICU nurses toward medical device‐related pressure injury. J Nurs Train. 2020;35(12):1073‐1079. [Google Scholar]
- 14. Galetto S, Nascimento E, Hermida PMV, Malfussi LBH. Medical device‐related pressure injuries: an integrative literature review. Rev Bras Enferm. 2019;72(2):505‐512. [DOI] [PubMed] [Google Scholar]
- 15. Widiati, E. , Nurhaeni, N. , Gayatri, D. , 2017. Medical‐device related pressure injuries to children in the intensive care unit. Compr child Adolesc Nurs 40 (sup1), 69‐77. [DOI] [PubMed]
- 16. Wei X, Yan F, Jing M, Li L, Wang Z. Nurses' knowledge, attitudes and practice towards prevention of medical device related pressure injury in intensive care units:a cross‐sectional study. Chin J Nurs. 2020;55(01):45‐50. [Google Scholar]
- 17. Y‐D H. Construction and Application of the Clinical Nurses Prevention Medical Device Related Pressure Injury of Critically Ill Patients for the Knowledge, Attitude, Practice Assessment Scale. Hebei, China: North China University of Science and Technology; 2018. [Google Scholar]
- 18. Kaddourah B, Abu‐Shaheen AK, Al‐Tannir M. Knowledge and attitudes of health professionals towards pressure ulcers at a rehabilitation hospital: a cross‐sectional study. BMC Nurs. 2016;15:17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Strand T, Lindgren M. Knowledge, attitudes and barriers towards prevention of pressure ulcers in intensive care units: a descriptive cross‐sectional study. Intensive Crit Care Nurs. 2010;26(6):335‐342. [DOI] [PubMed] [Google Scholar]
- 20. Khojastehfar S, Najafi Ghezeljeh T, Haghani S. Factors related to knowledge, attitude, and practice of nurses in intensive care unit in the area of pressure ulcer prevention: a multicenter study. J Tissue Viability. 2020;29(2):76‐81. [DOI] [PubMed] [Google Scholar]
- 21. Tayebi Myaneh Z, Rafiei H, Hosseinigolafshani SZ, Rashvand F. Relationship between practice and attitude regarding pressure injury among intensive care nurses in Iran: a descriptive, correlational study. Wound Manag Prev. 2020;66(6):27‐34. [PubMed] [Google Scholar]
- 22. Tirgari B, Mirshekari L, Forouzi MA. Pressure injury prevention: knowledge and attitudes of Iranian intensive care nurses. Adv Skin Wound Care. 2018;31(4):1‐8. [DOI] [PubMed] [Google Scholar]
- 23. Nuru N, Zewdu F, Amsalu S, Mehretie Y. Knowledge and practice of nurses towards prevention of pressure ulcer and associated factors in Gondar University hospital, Northwest Ethiopia. BMC Nurs. 2015;14:34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Jiang L, Li L, Lommel L. Nurses' knowledge, attitudes, and behaviours related to pressure injury prevention: a large‐scale cross‐sectional survey in mainland China. J Clin Nurs. 2020;29(17–18):3311‐3324. [DOI] [PubMed] [Google Scholar]
- 25. Hou J, Michaud C, Li Z, et al. Transformation of the education of health professionals in China: progress and challenges. Lancet. 2014;384(9945):819‐827. [DOI] [PubMed] [Google Scholar]
- 26. Barakat‐Johnson M, Barnett C, Wand T, White K. Knowledge and attitudes of nurses toward pressure injury prevention: a cross‐sectional multisite study. J Wound Ostomy Continence Nurs. 2018;45(3):233‐237. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
date available