
Fig. 1. Adipocyte function in healthy, obese, GDM and pre-eclampsia pregnancy.
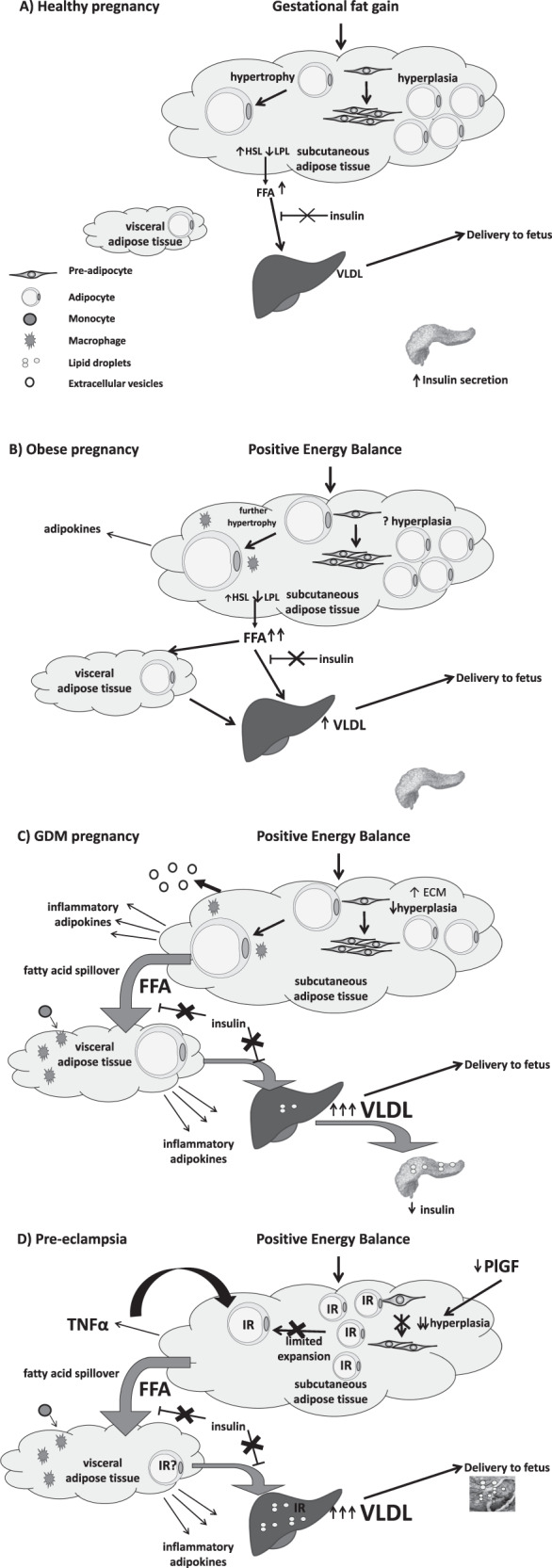
A In healthy pregnancy gestational fat storage is accommodated by adipocyte hypertrophy. The physiologically healthy level of insulin resistance permits controlled adipocyte lipolysis in order to supply triglycerides to the fetus via placental uptake of fatty acids from maternal VLDL. B Obese women already exhibit SAT and VAT adipocyte hypertrophy prior to pregnancy. During pregnancy they develop a greater degree of insulin resistance than lean women which reduces the ability of insulin to downregulate adipocyte lipolysis. This results in increased FFA flux to the liver and increased liver VLDL production. C In women who develop GDM, it is hypothesised that there is reduced hyperplasia and SAT hypertrophy resulting in fatty acid spillover. These fatty acids can cascade to ectopic sites including VAT, the liver and the pancreas and may lead to pancreatic dysfunction β-cell failure and the development of GDM. D In women who develop pre-eclampsia, it is hypothesised that there is an innate maternal insulin resistance manifest in both SAT and VAT. This insulin resistance reduces adipocyte differentiation, reducing the number of mature adipocytes and thereby reducing the capacity of SAT to store fat. Fatty acid spillover occurs leading to hypertriglyceridaemia and deposition of ectopic fat in the liver and placenta contributing to further maternal insulin resistance and placental dysfunction. FFA free fatty acid, HSL hormone-sensitive lipase, LPL lipoprotein lipase, SAT subcutaneous adipose tissue, VAT visceral adipose tissue, VLDL very low density lipoprotein.