
FIGURE 1.
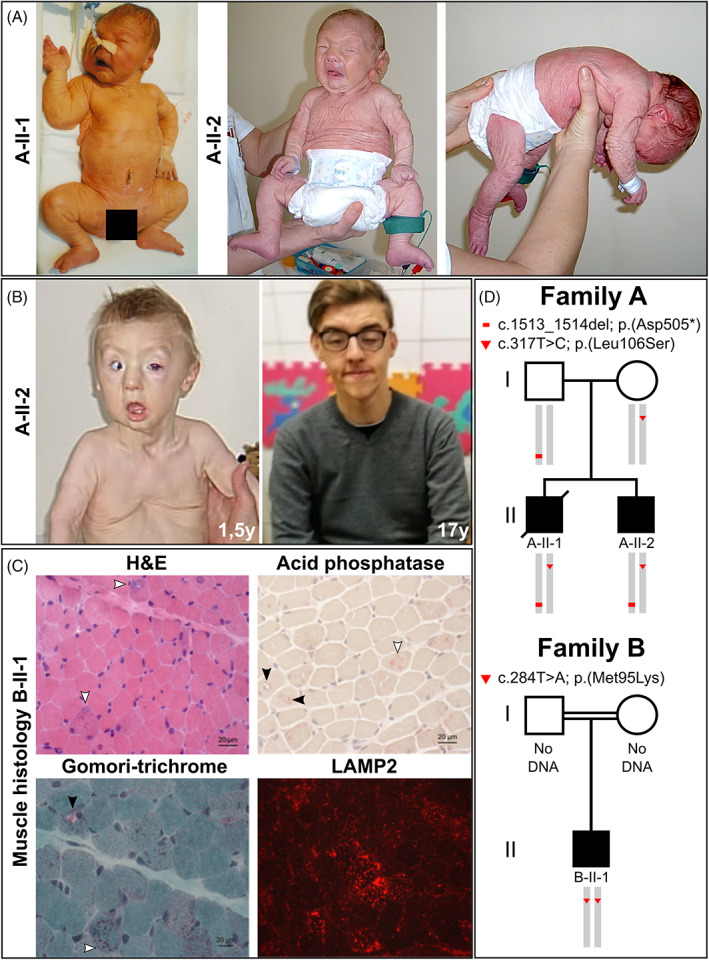
Clinical features of the affected individuals and disease gene identification. A, Both affected individuals A‐II‐1 and A‐II‐2 postnatally showed strong and generalized cutis laxa. Their facial gestalt was dysmorphic due to a triangular, mask‐like, face with a short and pointed chin. Additionally, individual A‐II‐2 showed a strong muscular hypotonia. B, Evolving phenotype in proband A‐II‐2 shows a strong improvement of the cutis laxa phenotype from 1.5 to 17 years of age. With 1.5 years of age he still showed an entropion and a strong pectus excavatum deformation. The cutis laxa phenotype improved within the first year of life. C, Histological findings: H&E staining revealed myofibres displaying centralized nuclei as well as rimmed vacuoles (white arrows). Additional Gomori‐trichrome staining shows mitochondrial accumulation within one representative vacuoles (black arrow) as well as within the sarcoplasm (white arrow) in a proportion of muscle cells. Acid phosphatase staining showed a positive reactivity of a proportion of vacuoles (black arrows) in addition to sarcoplasmic deposits (white arrow). Prominent build‐up of deposits of LAMP2 in a proportion of muscle fibers are respectively highlighted by white arrows. D, Schematic view of the co‐segregation analysis performed in both affected individuals from family A and their parents. The substitution c.317 T > C; p.(Leu106Ser) was transmitted via maternal, whereas the alteration c.1513_1514del; p.(Asp505*) was inherited through the paternal line. Both affected individuals were compound heterozygous. The alteration c.284 T > A; p.(Met95Lys) was found in a homozygous state in the affected individual from family B