
Figure 1:
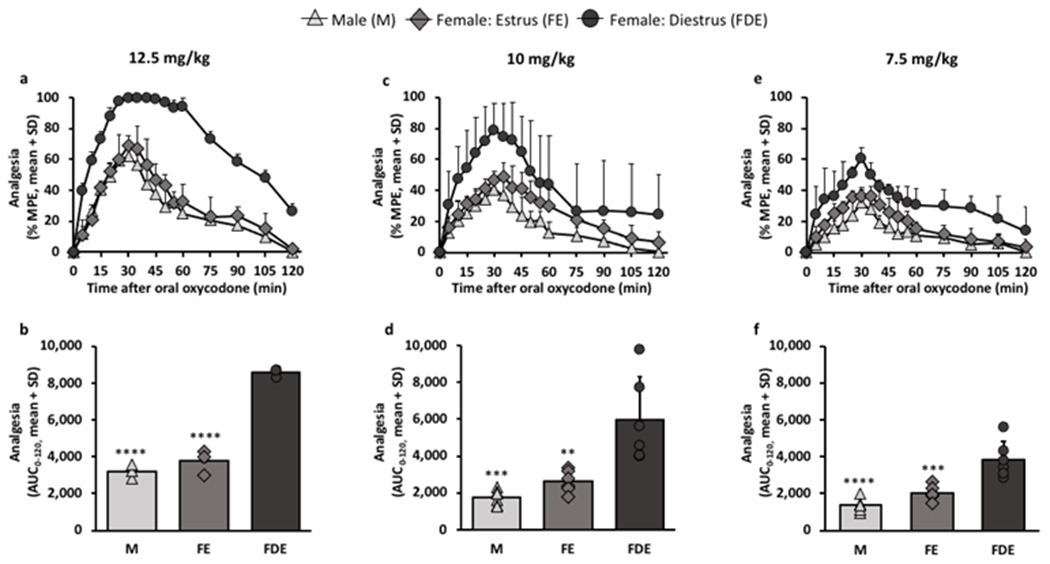
Females in diestrus had higher analgesia compared to males and females in estrus at varying oral oxycodone doses.
Analgesia was assessed after the following oral oxycodone doses- a, b, 12.5 mg/kg (n=3/group), c, d, 10 mg/kg (n=6/group), and e, f, 7.5 mg/kg (n=6/group). a, analgesic-time curve at 12.5 mg/kg (FSex/Cycle(2,6) = 123.70, p<0.0001; FTime(16,96) = 59.20, p<0.0001; FInteraction(32, 96) = 3.47, p<0.0001). b, analgesic AUC0-120 at 12.5 mg/kg (F(2,6) = 123.70, p<0.0001). c, analgesic-time curve at 10 mg/kg (FSex/Cycle(2,15) = 18.84, p<0.0001; FTime(16,240) = 80.67, p<0.0001; FInteraction(32, 240) = 4.65, p<0.0001). d, analgesic AUC0-120 at 10 mg/kg (F(2,15) = 14.94, p=0.0003). e, analgesic-time curve at 7.5 mg/kg (FSex/Cycle(2,15) = 27.17, p<0.0001; FTime(16,240) = 52.61, p<0.0001; FInteraction(32, 240) = 1.83, p=0.0059). f, analgesic AUC0-120 at 7.5 mg/kg (F(2,15) = 23.39, p<0.0001). Analgesic-time curves were assessed using two-way ANOVA with repeated measures by time. Analgesic AUCs0-120 were assessed using one-way ANOVA; **p<0.01, ***p<0.001, ****p<0.0001 relative to females in diestrus phase using Bonferroni post-hoc analysis.