
Figure 2.
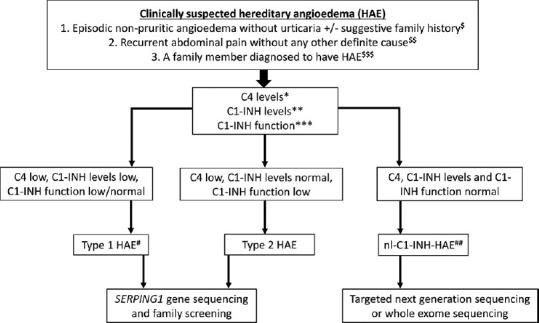
Simplified diagnostic algorithm for patients with clinically suspected HAE. $Family history of HAE may not be present in up to 20% of all patients with HAE. $$Recurrent pain abdomen may occasionally be the only clinical presentation of HAE. $$$Family members should be screened even if they are asymptomatic as late presentations and very mild presentations of HAE are known. *C4 levels are usually assessed using nephelometry, which may be normal in up to 20% of all patients even at the time of an acute attack. **C1-INH levels usually assessed using nephelometry. A repeat test is advised if the initial results are normal and there is high clinical suspicion of HAE. ***C1-INH function usually assessed using enzyme-linked immunosorbent assay (ELISA). Depending on the ease of accessibility, this test may be carried out at the time of initial presentation or after obtaining results of C4/C1-INH levels. Inappropriate storage or transport may affect the results of C1-INH functions. #A clinical possibility of acquired angioedema may be considered in patients with late-onset of symptoms (>40 years of age) and if there is no family history. Low C1q levels may be suggestive of acquired angioedema due to the presence of autoantibodies against C1-INH protein (seen in autoimmune diseases). ##At present, there are no biomarkers for diagnosis of nl-C1-INH-HAE