

Abstract
Individual differences in child eating self-regulation are associated with excess weight gain and may be explained, in part, by the family feeding environment and a child’s general propensity to self-regulate outside of the context of eating (i.e., general self-regulation). Several studies have examined the associations between food parenting behaviors, child eating and general self-regulation, and child weight separately. However, there are a paucity of data on whether and how these factors interact to confer risk for weight gain in early childhood. The current systematic review identified 32 longitudinal studies that examined unidirectional or bidirectional associations among one or more of the following paths: food parenting behaviors and child eating self-regulation (path 1); child eating self-regulation and child weight (path 2); child eating self-regulation and child general self-regulation (path 3); food parenting behaviors and child general self-regulation (path 4); and child general self-regulation and child weight (path 5). Results indicated relationships of food parenting behaviors to child eating self-regulation, child weight to child eating self-regulation, and child general self-regulation to child weight. However, there were scant longitudinal data that examined paths 3 and 4. Further research on the developmental correlates of child eating self-regulation is needed to identify parent and child targets for early childhood obesity prevention.
Keywords: Children, Obesity, Self-Regulation, Food Parenting, Executive Function
1. Introduction
Approximately 18.5% of children in the United States meet criteria for obesity (i.e., body mass index [BMI; kg/m2] ≥ the 95th percentile for age and sex) (Hales et al., 2017), with a significant increase in severe obesity (i.e., BMI ≥120% of the 95th percentile) over the past five years among young children ages 2 to 5 y (Hales et al., 2018). Excess weight in childhood is associated with numerous health and psychosocial consequences (Baker et al., 2007; Gibson et al., 2017) and is a primary predictor of obesity in adolescence and adulthood (Nader et al., 2006; Simmonds et al., 2016). Although efficacious treatments exist, such as family-based behavioral obesity treatment (FBT) (Altman & Wilfley, 2015), a considerable proportion of children do not achieve clinically meaningful weight change (Epstein et al., 1990, 2007). Thus, it is critical to identify risk factors for obesity in early childhood (i.e., ages 1 to 5 y) to prevent exacerbated weight gain and the development of weight-related comorbidities. One such risk factor is poor eating self-regulation.
Eating self-regulation refers to the ability to initiate and terminate further eating in response to internal cues of hunger and fullness and is comprised of two processes: satiation and satiety (Vohs & Baumeister, 2016). Satiation is involved in signaling the start and end of a meal, whereas satiety is involved in preventing further feeding between eating episodes in the absence of physical hunger (Blundell et al., 2010). Findings from early experimental studies have suggested that young children have a nascent capacity to self-regulate energy intake. In their seminal study (Fomon et al., 1975), Fomon and colleagues found that infants consistently consumed the same amount of energy from formula despite manipulations in quantity and energy density. Such data suggest that children as early as infancy are able to respond to internal satiation cues in the absence of parental control.
Additional evidence from Birch and colleagues indicated that most, but not all, young children maintained their ability to respond to satiation cues during the preschool years (i.e., ages 3 to 5 y) (Birch & Deysher, 1985, 1986; Johnson & Birch, 1994). However, children varied in their ability to compensate for change in energy density by weight status, such that children with overweight or obesity demonstrated poorer ability to accurately adjust energy intake compared to children with healthy weight (Johnson & Birch, 1994). Perturbations in satiety have also been documented in children as young as 3 y using Fisher and Birch’s eating in the absence of hunger (EAH) laboratory paradigm (Fisher & Birch, 1999), during which children consume a meal until full and are then provided highly palatable snack foods to consume freely while playing.
Consistent with laboratory findings, individual differences in child eating self-regulation have also been documented using parent-report measures, such as Wardle and colleagues’ Children’s Eating Behavior Questionnaire (CEBQ) (Carnell & Wardle, 2007; Wardle et al., 2001). The “food approach” subscales (i.e., food responsiveness, emotional overeating, enjoyment of food, and desire to drink) are most central to poor eating self-regulation, as evidenced by their associations with greater energy intake and higher weight status (Carnell & Wardle, 2007, 2008; Webber et al., 2009). Specifically, child food responsiveness (i.e., the extent to which a child shows interest in food and eating) and enjoyment of food (i.e., the extent to which a child enjoys food or finds eating pleasurable) were positively correlated with energy intake and eating rate during a laboratory test meal (Carnell & Wardle, 2007). Additionally, one study found that these dimensions along with emotional overeating (i.e., the propensity to overeat in response to a range of negative emotions) and desire to drink (i.e., quantity and frequency of drink consumption) were associated with higher weight status in children (Webber et al., 2009). Taken together, these data suggest that subgroups of children may be behaviorally susceptible to perturbations in eating self-regulation from an early age. A better understanding of the influences of poor eating self-regulation in early childhood may aid the development of novel targets for childhood obesity prevention.
Because parents are primarily responsible for child feeding during early childhood, the feeding environment is an important social context for shaping the development of eating self-regulation (Birch & Fisher, 1998). Parents use a variety of practices that dictate what and how a child eats (i.e., food parenting practices) and create a general climate around feeding (i.e., feeding styles). Thus, the extent to which a child is able to engage their capacity to self-regulate eating may be contingent on food parenting behaviors (i.e., food parenting practices and feeding styles). Parents may alter their approach to feeding in response to child weight and perceived child eating self-regulation. One longitudinal study found that child adiposity at age 4 y was predictive of parent food restriction at 10 y but not the reverse (Derks et al., 2017). Another prospective analysis found bidirectional associations between parental instrumental feeding (i.e., use of food as reward) and child food responsiveness (Berge et al., 2020). Taken together, these studies suggest that certain food parenting behaviors may undermine child eating self-regulation. This relationship may be reciprocal; that is, higher child weight status and perceived poor eating self-regulation may drive parents to adjust feeding accordingly.
In addition to the role of food parenting behaviors, individual differences in general self-regulatory capacities (i.e., general self-regulation) may predispose subgroups of children to poor eating self-regulation (Russell & Russell, 2020). General self-regulation is a multi-dimensional construct that “operates across several levels of function and in its broadest sense represents the ability to volitionally plan, and, as necessary, modulate one’s behaviors to an adaptive end” (Montroy et al., 2016). A central aspect of general self-regulation is executive function (EF), which refers to the neurocognitive functions primarily associated with the prefrontal cortex that service goal-directed behavior (Zelazo et al., 2008). Findings from reviews have supported a link between executive function impairments and child overweight and obesity (Hayes et al., 2018; Liang et al., 2014; Reinert et al., 2013), which may be due to excess energy intake resulting from poor eating self-regulation (Egbert et al., 2019).
Although prior research has examined the associations between food parenting behaviors, child self-regulation (both general and eating specific), and child weight separately (Egbert et al., 2019; Tan & Lumeng, 2018; Ventura & Birch, 2008; Yee et al., 2017), no reviews have summarized whether or how (i.e., directionality) these associations interact. Further, data in early childhood are limited, which is a critical period for the development of self-regulation and the prevention of obesity. Therefore, the current review will synthesize longitudinal research on the following pathways (Fig. 1): path 1) association between food parenting behaviors and eating self-regulation; path 2) association between child eating self-regulation and weight; path 3) association between child eating self-regulation and general self-regulation; path 4) association between food parenting behaviors and child general self-regulation; path 5) association between child general self-regulation and weight. An integration of the literature could inform a conceptual model of the development of child eating self-regulation and identify parent and child targets for obesity prevention in early childhood.
Fig. 1.
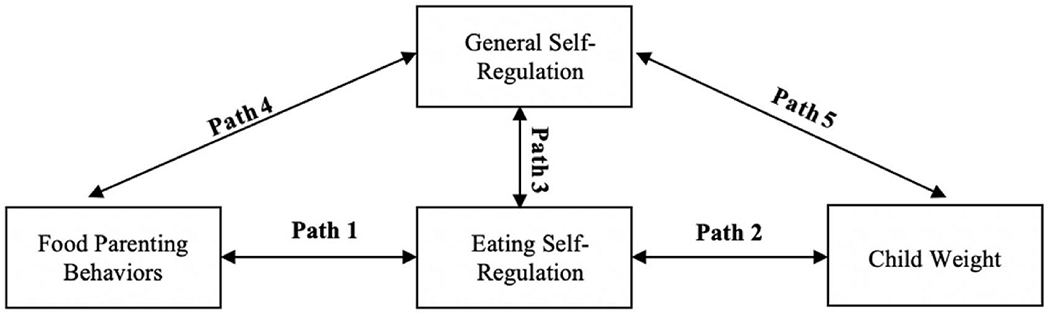
Conceptual model of parent-child influences on eating self-regulation and weight.
2. Methods
2.1. Operationalization of key constructs
The breadth of relevant constructs related to food parenting behaviors, child self-regulation (both eating and general), and child weight has led to inconsistent terminology and operationalization. The following section will provide a brief overview of operational definitions of key constructs and their measurement (Table 1).
Table 1.
Operationalization of key constructs and measurement.
| Construct | Definition | Common Measure(s) |
|---|---|---|
| Food Parenting Practices | ||
| Coercive Control | Food parenting practices intended to dominate, pressure, or control eating according to parents’ desires or expectations, including: • Pressure to eat • Restriction • Threats and bribes • Emotional feeding • Instrumental feeding/food as reward |
• Child Feeding Questionnaire • Parental Control Index • Comprehensive Feeding Practices Questionnaire • Structure and Control in Parent Feeding Questionnaire |
| Structure | Food parenting practices intended to provide enforcement of food-related rules and limits, structure of the feeding environment, and non-coercive monitoring of child food intake, including: • Snack and mealtime routines • Limit setting/Monitoring • Modeling • Food availability/accessibility |
• Family Meal Practices Survey • Family Food Rules Questionnaire • Child Feeding Questionnaire |
| Autonomy Support or Promotion | Food parenting practices intended to promote autonomy of food-related decision making and independence, including: • Nutritional information • Encouragement/praise • Child involvement • Reasoning/negotiation |
• Comprehensive Feeding Practices Questionnaire • Parent Feeding Style Questionnaire • Food Parenting Practices Questionnaire |
| Feeding Styles | ||
| Authoritarian | Feeding style characterized by high demandingness/low responsiveness, including: • Coercive control • Restrictive or punitive behaviors • Low warmth |
• Caregiver’s Feeding Styles Questionnaire |
| Authoritative | Feeding style characterized by high demandingness/high responsiveness, including: • Parental involvement • Structure • Reasoning/negotiation |
• Caregiver’s Feeding Styles Questionnaire |
| Indulgent/Permissive | Feeding style characterized by low demandingness/high responsiveness, including: • High warmth • Low monitoring/structure |
• Caregiver’s Feeding Styles Questionnaire |
| Uninvolved | Feeding style characterized by low demandingness/low responsiveness, including: • Low involvement, engagement, and attunement to child needs |
• Caregiver’s Feeding Styles Questionnaire |
| Eating Self-Regulation | ||
| Eating in the Absence of Hunger | Eating past the state of physical fullness | • EAH Paradigm and Questionnaire |
| Food Responsiveness | General interest in food and eating | • Children’s Eating Behavior Questionnaire |
| Emotional Overeating | Propensity to eat in response to a range of negative emotions | • Children’s Eating Behavior Questionnaire |
| Enjoyment of Food | Extent of a tendency to enjoy food and find eating and food pleasurable | • Children’s Eating Behavior Questionnaire |
| Desire to Drink | Quantity and frequency of drink consumption | • Children’s Eating Behavior Questionnaire |
| General Self-Regulation (Performance-Based Tasks) | ||
| “Cool” EF | ||
| Working Memory | Storing and manipulating information to complete complex tasks | • Backwards Digit Span |
| Cognitive Flexibility | Switching between thoughts and behaviors in response to environmental demands | • Wisconsin Card Sorting Task • Dimensional Change Card Sorting Task • Stroop Task |
| Inhibitory Control (may be considered “hot” EF in certain contexts) | Inhibiting responsiveness to pre-potent cues in favor of a different behavior | • Stop Signal Task |
| “Hot” EF | ||
| Delay of Gratification | Postponing immediate gratification in pursuit of long-term reward | • Modified Choice Paradigm |
| Affective Decision Making | Decision making under conditions of choice and uncertainty | • Children’s Gambling Task • Hungry Donkey Task |
| General Self-Regulation (Multi-Informant Questionnaires) | ||
| Global Measures of EF | Behavioral Regulation Index (composite of inhibitory, set shifting, and emotional control scales) Composite of emotional/personality, motivational, behavioral, cognitive functions | • Behavior Rating Inventory of Executive Functions • Behavioral Assessment of the Dysexecutive Syndrome in Children |
2.1.1. Food parenting behaviors
Food parenting behaviors is an encompassing term that includes both food parenting practices and feeding styles. Food parenting practices and feeding styles represent related, but distinct, aspects of the parent-child feeding dynamic (Collins et al., 2014). Food parenting practices refer to the behavioral strategies used to influence child eating, whereas feeding styles refer to the overall emotional quality of the parent-child dynamic in the context of feeding (Ventura & Birch, 2008). Results from a food parenting working group (Hughes et al., 2013) also identified general parenting styles; that is, the broad context of parent-child interactions across domains, as a relevant construct, and some researchers have postulated that general parenting styles may moderate the association between parent feeding behaviors, child eating self-regulation, and child weight (Larsen et al., 2018). Because research in this area is still emerging, the current review focused on parenting in the context of feeding (i.e., food parenting behaviors) and summarized findings on food parenting practices and feeding styles separately to distinguish their independent associations with child eating self-regulation and weight.
2.1.1.1. Food parenting practices.
Findings from observational studies show that food parenting practices are state-like in nature; that is, food parenting practices fluctuate (Berge et al., 2018; Eichler et al., 2019) and are sensitive to contextual factors (e.g., parental stress) that influence their consistent implementation across mealtimes (Berge et al., 2017). Various self-report measures have been developed to assess food parenting practices, including the Child Feeding Questionnaire (Birch et al., 2001), Parental Control Index (Wardle et al., 2005), Parent Feeding Style Questionnaire (Wardle et al., 2002), the Comprehensive Feeding Practices Questionnaire (Musher-Eizenman & Holub, 2007), and the Structure and Control in Parent Feeding Questionnaire (Savage et al., 2017). The varying terminology across measures, however, has led to inconsistent operationalization of specific food parenting practices. As a result, Vaughn and colleagues developed a content map to summarize key overarching domains and subdomains related to food parenting practices (Vaughn et al., 2016). The three domains include coercive control, structure, and autonomy support.
Coercive control refers to feeding practices intended to dominate, pressure, or control eating according to parents’ desires or expectations, including restricting food or setting strict limits, pressuring a child to eat, using food to bribe desired behavior or threaten misbehavior, and feeding to sooth negative emotions. Structure refers to feeding practices intended to provide enforcement of food-related rules and limits and monitor, but not restrict, food intake. These practices include setting routines around snacks and meals, setting limits and guidelines around what, when, and how a child eats while not restricting food consumption, modeling healthy eating, and providing a variety of foods in the home. Last, autonomy support includes feeding practices intended to promote autonomy of food-related decision making and independence, such as providing nutritional information, encouraging and praising healthy food choices, involving the child in food-related decision making, and reasoning and negotiating around what and how the child eats.
2.1.1.2. Feeding styles.
In contrast to food parenting practices, feeding styles are consistent, trait-like expressions of the overall parent-child feeding dynamic that vary in terms of demandingness and responsiveness (Hughes et al., 2005). In the context of feeding, demandingness refers to the extent to which a parent prompts child eating, and responsiveness refers to how a parent prompts child eating (Hughes et al., 2005). Feeding styles are further classified across these dimensions to form four unique categories: authoritarian (high demandingness/low responsiveness), authoritative (high demandingness/high responsiveness), permissive/indulgent (low demandingness, high responsiveness), and uninvolved (low demandingness/low responsiveness). A parent with an authoritarian feeding style may be overly restrictive, tell a child exactly what and how to eat, and set rigid boundaries around food and eating, whereas a parent with an authoritative feeding style may provide structure and limit setting around food and mealtimes but in a manner that is supportive and warm. A parent with a permissive or indulgent feeding style may lack boundaries regarding food and eating and may be overly responsive to child hunger cues. Last, a parent with an uninvolved feeding style may show little interest in assisting with eating and demonstrate a lack of boundaries and poor mealtime structure. The most common and well-validated measure of feeding styles is the Caregiver’s Feeding Styles Questionnaire (Hughes et al., 2005).
2.1.2. Eating self-regulation
As previously defined, eating self-regulation refers to the ability to initiate and terminate further eating in response to internal cues of hunger and fullness (Vohs & Baumeister, 2016). The current review only examined behavioral dimensions of eating self-regulation that have been measured using validated assessments suitable for younger children. These include the “food approach” subscales from the CEBQ (i.e., food responsiveness, enjoyment of food, emotional overeating, and desire to drink subscales) (Carnell & Wardle, 2007; Wardle et al., 2001) and Birch and colleagues’ EAH paradigm (Fisher & Birch, 1999). The CEBQ “food approach” subscales demonstrate good convergent validity with ad libitum energy intake following the EAH paradigm (Carnell & Wardle, 2007). Studies that assessed EAH using the Eating in the Absence of Hunger Questionnaire for Children and Adolescents (EAH-C) (Tanofsky-Kraff et al., 2008) or the Parent Report of Child Eating in the Absence of Hunger (EAH-PC) (Shomaker et al., 2013) were also reviewed. However, these measures do not demonstrate good concurrent validity with objectively measured EAH (Madowitz et al., 2014).
2.1.3. General self-regulation
Definitions of general self-regulation are broad and inconsistent across the literature (Cole et al., 2019). As such, the current review focused explicitly on EF. There is general agreement that EF involves higher-order cognitive processes that aid abstract and decontextualized decision making (i.e., “cool” EF) (Zelazo & Carlson, 2012). The core components of “cool” EF include cognitive flexibility (i.e., switching between thoughts and behaviors in response to environmental demands), working memory (i.e., storing and manipulating information to complete tasks), and inhibitory control (i.e., inhibiting responsiveness to pre-potent cues in favor of a different behavior), which work together across a variety of contexts to aid abstract problem solving. Substantive evidence also highlights the role of EF in motivation and emotion-based decision making (i.e., “hot” EF), including delayed gratification (i.e., delaying immediate reward) and affective decision making (i.e., choice under conditions of risk and uncertainty) (Zelazo & Carlson, 2012). Inhibitory control is also sometimes regarded as a “hot” EF depending on whether the stimulus prompts motivation or emotion.
From a developmental perspective, the “hot” - “cool” distinction may be particularly useful in elucidating which EF components are relevant to child eating self-regulation and weight in early childhood. Evidence suggests that “hot” and “cool” EF have different developmental correlates (Hongwanishkul et al., 2005). Further, “hot” and “cool” EF may have different developmental trajectories, with some data suggesting that “hot” EF develops more gradually than “cool” EF (Kerr & Zelazo, 2004; O’Toole et al., 2018). However, it remains unclear whether “hot” and “cool” EF are dissociable in early childhood. Thus, the current review examined both “hot” and “cool” aspects of EF to disentangle which components of EF are most central to eating and weight. Various methodologies have been used to measure “hot” and “cool” EF in young children, including performance-based tasks and multi-informant rating scales. An exhaustive overview of EF assessments is beyond the scope of the current review. However, the following assessments represent some of the most widely used methods that are suitable for young children.
2.1.3.1. Performance-based tasks.
Performance-based measures of EF provide an internally valid assessment of cognitive abilities under standardized conditions. The majority of performance-based tasks for children have been adapted from well-validated measures in adult samples. To measure working memory, the digit span subtest of the WISC-IV (Wechsler, 2003) for children is commonly administered. Cognitive flexibility is commonly assessed using the Wisconsin Card Sorting Task (Berg, 1948), the Dimensional Change Card Sorting Task (Zelazo, 2006), or the Stroop Task (Stroop, 1935), which all require a child to alter their card sorting strategy based on changes in shape, color, or word. Inhibitory control is commonly assessed using the Stop Signal Task (Matthews et al., 2005). To measure delayed gratification, the modified choice paradigm asks children to choose between a reward (food or nonfood) now or delaying receiving the reward in a week (Mischel et al., 1989). The number of trials in which a child chooses to delay the reward is operationalized as delay of gratification. Last, affective decision making is commonly assessed using the Hungry Donkey Task (food-specific reward) (Crone & van der Molen, 2004) or Children’s Gambling Task (monetary reward) (Kerr & Zelazo, 2004). In these tasks, children choose from deck of cards that convey rewards or losses. One deck of cards is more advantageous per trial but is disadvantageous across trials; affective decision making is operationalized as the number of advantageous choices made across trials.
2.1.3.2. Multi-informant questionnaires.
Although performance-based tasks demonstrate excellent internal validity, a common critique is their ecological validity; that is, how well task-based performance aligns with EF across a variety of real-world settings. As such, multi-informant questionnaires or rating scales, which assess child EF from the perspective of parents and teachers, provide ecologically valid assessments of child EF in the naturalistic environment. Common multi-informant questionnaires of EF include the total score or the behavioral regulation index of the Behavior Rating Inventory of Executive Functions (BRIEF) (Gioia et al., 2000), the single scale of the Behavioral Assessment of the Dysexecutive Syndrome in Children (BADS-C) (Wilson et al., 2004), among others (Toplak et al., 2013). Importantly, convergence between performance-based tasks and multi-informant ratings of child EF is modest (Toplak et al., 2013), which may reflect their measurement of different aspects of EF. Performance-based tasks measure optimal EF under highly controlled conditions, whereas multi-informant questionnaires assess success in goal pursuit across a variety of settings. Thus, both forms of assessments are valid, and their concurrent use provides insight into child EF capacities across levels of functioning.
2.1.4. Child weight status
Studies that measured body weight or adiposity were reviewed. The most common and widely available measure of body composition is BMI, which for children is standardized across age and sex. Overweight is defined as a BMI ≥ the 85th percentile for age and sex (Kuczmarski et al., 2002). Obesity and severe obesity are defined as BMI ≥ the 95th percentile for age and sex and 120th percentile of the 95th percentile for age and sex, respectively (Kuczmarski et al., 2002). Although BMI is not an objective measure of adiposity, it is strongly correlated with body fat mass in children (Martin-Calvo et al., 2016). Objective measures of adiposity including skinfold thickness, dual energy x-ray absorptiometry (DEXA) and bioelectrical impedance analysis (BIA) were also reviewed.
2.2. Literature Search and selection criteria
A systematic search of relevant articles was conducted from November 2020 to January 2021 using PubMed, Google Scholar, and MEDLINE databases. Data synthesis and extraction were conducted in compliance with Preferred Reporting Items for Systematic Reviews and Meta Analyses (PRISMA) guidelines. Articles were required to be original, quantitative research published in a peer-reviewed journal that included measures pertaining to at least one of the five paths (Fig. 2). Additional inclusion criteria were longitudinal study design, healthy sample of children ages one to five at the time of the first assessment with or without obesity, written in English, and published between the years 2000–2021 to highlight the most up-to-date literature. Studies were excluded for the following reasons: cross-sectional or qualitative study design, special population of children with a weight-related comorbidity (e.g., children with diabetes), participation in an intervention targeting child self-regulation or weight, children younger than 1 or older than 5 y at the time of first assessment, published prior to the year 2000, did not assess one of the five paths, examined general parenting but not food parenting behaviors. Review of articles on the link between food parenting behaviors and child weight status was beyond the scope of the review and has been summarized elsewhere (Ventura & Birch, 2008).
Fig. 2.
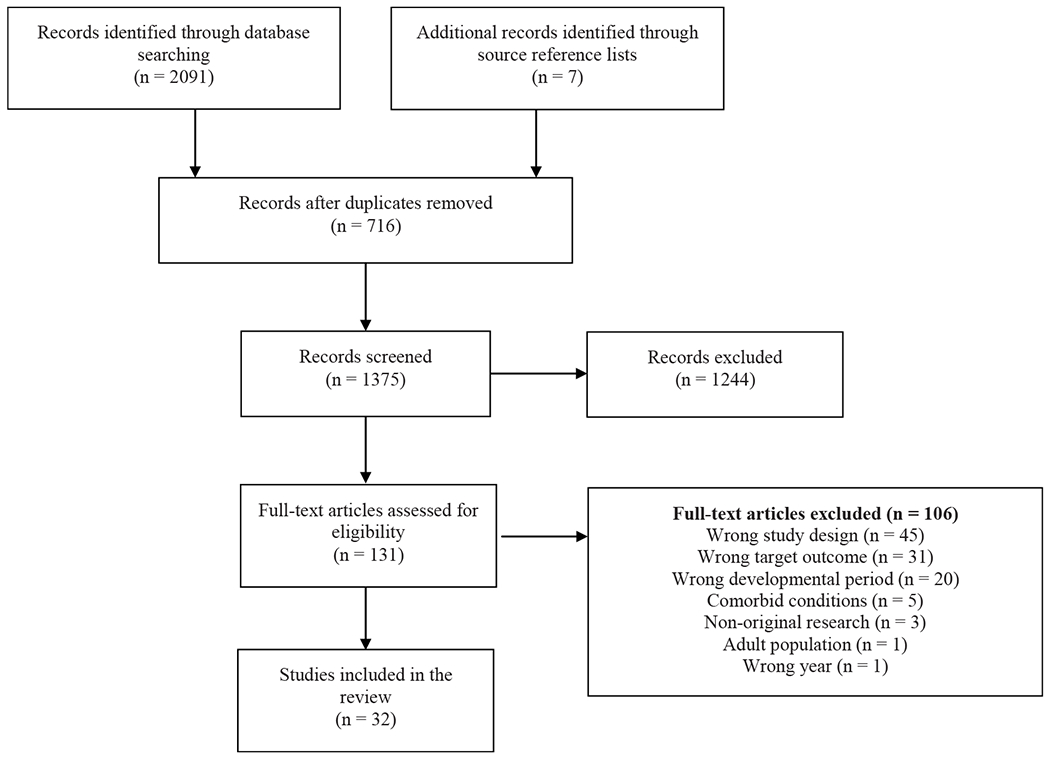
PRISMA flow chart of literature search and selection.
2.3. Search strategy
Separate search strings were used for each of the paths. Paths 1 and 4: food parenting behaviors search strings included parent, feeding, feeding styles, feeding practices, authoritative, authoritarian, permissive, uninvolved, restriction, pressure to eat. Paths 1–5: child self-regulation (both eating and general) search terms were regulat*, executive function, executive functioning, inhibitory control, working memory, cognitive flexibility, delay of gratification, self-control, eating self-regulation, appetite self-regulation, appetite. Paths 2 and 5: weight status search strings were obes*, overweight, body mass index, BMI, weight, adiposity. Abstract titles had to include the terms child, children, youth, toddler, toddlerhood, preschool, preschoolers, or childhood.
2.4. Data extraction and synthesis
Abstracts were retrieved from the databases and uploaded into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) and reviewed by the first author (A.C.G.) for inclusion/exclusion. Additional articles retrieved from the reference lists of articles were also reviewed. After removal of duplicates, each abstract was reviewed to ensure inclusion of measures pertaining to at least one of the five paths and to confirm the sample age of children at the baseline assessment fell during early childhood. The following information was extracted from the articles: path(s) addressed, year of publication, country, sample characteristics (e.g., sample size, child age, child sex), independent and dependent variables, measures, and main outcomes related to the relevant path(s).
3. Results
3.1. Study selection
Two thousand ninety-one references were imported for screening. After removing duplicates (n = 716), 1375 studies were screened against title and abstract, of which 1244 were excluded. Of the remaining 131 studies assessed for full-text eligibility, 106 studies were excluded due to the following reasons: 45 used cross-sectional or qualitative design, 31 did not examine the targeted outcome, 20 did not examine children in early childhood, five studies examined children with obesity and other conditions, three were non-original research (e.g., reviews), one study included an adult population, and one study was published prior to 2000. An additional seven studies were identified from reference lists and were screened and included for full-text extraction, yielding a final sample of 32 articles (Fig. 2).
3.2. Study characteristics
Of the 32 studies included, four studies examined food parenting behaviors and child eating self-regulation alone (path 1), five studies examined child eating self-regulation and child weight alone (path 2), and 10 studies examined food parenting behaviors and child eating self-regulation in combination with child weight (paths 1 and 2). One study examined child general self-regulation and eating self-regulation (path 3). No studies examined food parenting behaviors in relation to child general self-regulation alone (path 4), but three studies examined child general self-regulation as a moderator or mediator between food parenting and child weight status (paths 4 and 5). Nine studies examined the link between child general self-regulation and child weight alone (path 5). The majority (n = 25) of studies were published between 2010 and 2021, whereas seven studies were published between 2002 and 2009. Twenty-one studies were conducted in the United States, and the remaining studies were conducted in Australia (n = 5), Netherlands (n = 3), Norway (n = 2), or the United Kingdom (n = 1). The age of participants at the time of the first assessment ranged from 15 months to five years. The majority of samples (n = 26) included both boys and girls, whereas six studies from the same research group included only girls. Characteristics and main outcomes of each study are summarized in Tables 2 and 3 according to path(s) addressed. Results are summarized by domain of eating self-regulation (i.e., EAH, food responsiveness, emotional overeating, enjoyment of food, desire to drink) and general self-regulation (i.e., inhibitory control, working memory, cognitive flexibility, affective decision making, delayed gratification).
Table 2.
Studies examining path 1, path 2, or in combination.
| Authors | Country | Sample | Independent Variable(s) | Measure | Dependent Variable(s) | Measure | Direction Tested | Results |
|---|---|---|---|---|---|---|---|---|
| Path 1 Only: Food Parenting Behaviors (FPB) and Child Eating Self-Regulation (ESR) | ||||||||
| Farrow et al. (2015) | United Kingdom | n = 35; Age 2–7; boys and girls | food as reward; emotional feeding; restriction; pressure to eat | CFPQ | EAH | EAH protocol | FPB -> ESR | + Parental use of food as reward and restriction of food for health at ages 3–5 y associated with greater child EAH at ages 5–7 y |
| Bauer et al. (2017) | United States | n = 229; Age 21–33 months; boys and girls | parental restriction; EAH | IFSQ; EAH protocol | Parental restriction; EAH | IFSQ; EAH protocol |
FPB -> ESR ESR -> FPB |
- Maternal restriction of food amount at 21 months inversely associated with EAH at month 27 ∅ Maternal restriction of food amount at 27 months not associated with EAH at 33 months ∅ Maternal restriction of food quality at 21 months not associated with EAH at 27 or 33 months ∅ Child EAH at 21 months not associated with either type of maternal restriction at 27 or 33 months |
| Jansen et al. (2018) | Australia | n = 207; Age 2–5; boys and girls | structure and non-responsive related feeding practices | FPSQ | food responsiveness | CEBQ |
FPB -> ESR ESR -> FPB |
- Lower parental covert restriction at age 2 y associated with higher food responsiveness at age 3.7 y + Higher food as reward at age 2 y associated with higher food responsiveness at age 3.7 y ∅ Child food responsiveness not prospectively associated with parent feeding practices ∅ Parent meal structure not prospectively associated with child food responsiveness |
| Berge et al. (2020) | United States | n = 534; Age 2–4; boys and girls | food responsiveness; enjoyment of food; emotional feeding; control; encouragement; instrumental feeding | CEBQ; PFSQ | food responsiveness; enjoyment of food; emotional feeding; control; encouragement; instrumental feeding | CEBQ; PFSQ |
FPB -> ESR
ESR-> FPB |
+ Bidirectional prospective relationships between parental instrumental feeding and food responsiveness + Parent emotional feeding associated with child food responsiveness one year later ∅ Child food responsiveness not prospectively associated with parent emotional feeding one year later |
| Path 2 Only: Child ESR and Weight Status | ||||||||
| Shunk and Birch (2004) | United States | n = 153; Age 5–9; girls | weight status | BMI % | EAH | EAH protocol | weight -> ESR | + Risk for overweight at age 5 y associated with EAH at age 9 7 |
| Malian et al. (2014) | Australia | n = 37; Age 2–4.5; boys and girls | food responsiveness; enjoyment of food | CEBQ | EAH; weight status | EAH protocol; BMIz | ESR -> weight ESR -> ESR |
∅ Food responsiveness and enjoyment of food not associated with BMIz or EAH |
| Steinsbekk & Lars Wichstrom (2015) | Norway | n = 995; Age 4–8; boys and girls | enjoyment of food; food responsiveness; emotional overeating; weight status | CEBQ; BMI-SDs | enjoyment of food; food responsiveness; emotional overeating; weight status | CEBQ; BMI-SDs |
ESR -> weight
weight -> ESR |
+ Higher food responsiveness at age 6 predicted higher BMI SDs at age 6 y and increased weight gain from ages 6 to 8 y + Growth in BMI SDs from ages 4–6 y predicted both higher levels and growth of food responsiveness from ages 6–8 y ∅ No bidirectional associations among emotional overeating, enjoyment of food, and BMI SDs |
| Derks et al. (2018) | The Netherlands | n = 3331; Age 4–10; boys and girls | weight status; body fat mass; emotional overeating; food responsiveness; enjoyment of food | BMI-SDS and DXA scan; CEBQ | weight status; body fat mass; emotional overeating; food responsiveness; enjoyment of food | BMI-SDS and DXA scan; CEBA |
weight -> ESR ESR-> weight |
+ Higher BMI-SD and greater fat mass at age 4 y predicted more food responsiveness and enjoyment of food ∅ Weight and fat mass at age 4 y not prospectively associated with emotional overeating at age 10 y ∅ Child approach eating behaviors at age 4 y did not predict child BMI-SD or fat mass at age 10 y |
| Power et al. (2020) | United States | n = 118; Age 4–8; boys and girls | food responsiveness; emotional overeating; weight status | CEBQ; BMIz | food responsiveness; emotional overeating; weight status | CEBQ; BMIz |
weight -> ESR
ESR-> weight |
+ Bidirectional association between emotional overeating at mean age 6.3 y and BMIz at mean age 8.3 y ∅ No cross-lagged associations between BMIz and food responsiveness across timepoints |
| Path 1 and 2: FPB, Child ESR, and Child Weight | ||||||||
| Fisher and Birch (2002) | United States | n = 192; Age 5–7; girls | parental restriction | CFQ | EAH; weight status | EAH protocol; BMI % |
FPB -> ESR
ESR -> weight |
+ EAH at age 5 and 7 y associated with higher odds of overweight at both ages + Parental restriction at age 5 y predicted EAH at 7 y |
| Birch et al. (2003) | United States | n = 192; Age 5–9; girls | parental restriction; monitoring; pressure to eat | CFQ | EAH; weight status | EAH protocol; BMI % | FPB-> ESR weight, FPB-> ESR | + Higher levels of parental restriction at age 5 predicted higher EAH at age 7 and 9 y + Girls who were overweight at age 5 y and whose mothers reported high restriction had the greatest increases in EAH from 5 to 9 y |
| Francis and Birch (2005) | United States | n = 171; Age 5 y; girls | parental restriction | CFQ | EAH; weight status | EAH protocol; BMI % |
FPB-> ESR
ESR -> weight |
+ Restriction among mothers with overweight predicted daughter EAH at 7 and 9 y but not mothers with healthy weight + EAH of girls whose mothers had overweight associated with BMI change at age 7 and 9 y |
| Gregory et al. (2010) | Australia | n = 156; Age 2–4; boys and girls | parental restriction; monitoring; pressure to eat; modeling | CFQ; CEBQ; modeling questionnaire | Food responsiveness; interest in food; weight status | CEBQ; BMIz | FPB -> ESR ESR -> weight | ∅ Restriction not predictive of food responsiveness one year later ∅ No impact of feeding practices or child food-approach behaviors on child BMIz one year later |
| Rodgers et al. (2013) | Australia | n = 222, Age 2; boys and girls | CFQ subscales; CEBQ subscales; tendency to overeat | CFQ; PFQ; PFSQ; COEQ; CFPQ: CEBQ; DEBQ-P | CFQ subscales; CEBQ subscales; tendency to overeat | CFQ; PFQ; PFSQ; COEQ; CFPQ: CEBQ; DEBQ-P |
FPB -> ESR, weight
ESR -> FPB |
- Monitoring predicted child food approach behaviors one year later - Child food approach behaviors predicted instrumental feeding one year later + Instrumental feeding associated with BMIz change one year later + Child tendency to overeat associated with instrumental feeding one year later + Child emotional eating associated with emotional feeding and covert control one year later |
| Path 1 and 2 Continued: FPB, Child ESR, and Child Weight | ||||||||
| Bergmeier et al. (2015) | Australia | n = 201; Age 3-5; boys and girls | parent feeding styles; restriction; pressure to eat | PSQ; CFQ | enjoyment of food; weight status | CEBQ; BMIz | FPB -> EAH, weight | ∅ No significant prospective associations between restriction or pressure to eat at time 1 and enjoyment of food or BMIz at time 2 |
| Steinsbekk, Belsky, & Wichstrom (2016) | Norway | n = 797; Age 4-8; boys and girls | instrumental feeding; encouragement to eat; control overeating; CEBQ subscales; weight status | PFSQ; CEBQ; BMI | instrumental feeding; encouragement to eat; control overeating; CEBQ subscales; weight status | PFSQ; CEBQ; BMI |
FPB -> ESR weight -> ESR ESR -> FPB |
+ Greater instrumental feeding at age 6 y predicted increased food responsiveness and emotional overeating at age 8 y + Greater encouragement to eat at age 6 y predicted increased emotional overeating at age 8 y + Child BMI at age 6 y positively associated with food responsiveness at age 8 y ∅ Emotional overeating, enjoyment of food, or BMI did not predict parent feeding practices |
| Galindo et al. (2018) | United States | n = 138; Age 4-5; boys and girls | pressure to eat; observed parental prompting; EAH | CFQ; BMIz; EAH protocol | pressure to eat; observed parental prompting; EAH | CFQ; EAH protocol |
weight -> ESR
FPB-> ESR |
+ Higher child weight at time 1 predicted EAH at time 2 + Observed prompts to eat a different food predicted EAH at time 2 ∅ Self-reported pressure to eat not predictive of EAH at time 2 |
| Derks et al. (2019) | The Netherlands | n = 3514; Age 4-10; boys and girls | weight status; parental monitoring, restriction, pressure to eat | BMI-SDs; CFQ | food responsiveness; enjoyment of food; emotional overeating | CEBQ | Weight -> ESR FPB -> ESR |
+ Children with overweight or obesity were more likely to have increasing patterns of emotional overeating compared to underweight/healthy weight peers - Monitoring associated with lower odds of increasing patterns of emotional overeating + Restrictive feeding associated with higher odds of increasing patterns of emotional overeating, food responsiveness, enjoyment of food - Pressure to eat associated with lower odds of increasing food responsiveness |
| Jansen et al. (2018) | The Netherlands | n = 3643; Age 4–9; boys and girls | food as reward; food responsiveness; emotional overeating; child weight | CFQ; CEBQ; BMIz | food as reward; food responsiveness; emotional overeating; child weight | CFQ; CEBQ; BMIz |
FPB -> ESR
ESR -> FPB |
+ Parent use of food as reward at age 4 y associated with higher levels of emotional overeating at age 9 y + Higher emotional overeating and food responsiveness at age 4 associated with parent food as reward at age 9 ∅ Child BMIz at age 4 y was not associated with later food as reward at age 9 y |
Table 3.
Studies examining path 3, path 4, path 5, or in combination.
| Authors | Country | Sample | Independent Variable(s) | Measure | Dependent Variable(s) | Measure | Direction Tested | Results |
|---|---|---|---|---|---|---|---|---|
| Paths 3,4,5: FPB, Child ESR/General Self-Regulation (GSR), and Child Weight | ||||||||
| Rollins et al. (2014) | United States | n = 192; Age 5–7; girls | parental restriction; child perceived restriction; inhibitory control | CFQ; RAQ; CBQ; CEBQ | weight status; EAH | BMI%; EAH protocol | FPB; GSR -> ESR; weight | + Girls whose mothers used sets limits + restricts all snacks had a higher approach and EAH at 5 y - Low inhibitory control girls whose mothers used sets limits + restricts all snacks or unlimited access to snacks had greater increases in EAH and BMI from 5 to 7 y |
| Paths 4 and 5: Food Parenting, Child GSR, and Child Weight | ||||||||
| Anzman and Birch (2009) | United States | n = 197; Age 5–15; girls | perceived parental restriction; inhibitory control | CFQ (child report); CBQ | weight status | BMI% | FPB; GSR - > weight | -Lower inhibitory control at age 7 y associated with higher BMIs at all time points - BMI gains were the highest among girls who perceived higher parental control at age 7 y and were low on inhibitory control |
| Connell et al. (2014) | United States | n = 778; Age 4–15; boys and girls | parent feeding style; delayed gratification | parental sensitivity and expectations for child self-control; delay of gratification task | weight status | BMI% | GSR; FPB - > weight | - Boys who had authoritarian mothers and failed to delay gratification had a sig steeper rate of growth in BMI from childhood to 15 y |
| Lelakowska et al. (2019) | United States | n = 169; 24–30 months; boys and girls | motional overeating; inhibitory control; parental monitoring; parental restriction | CEBQ; Snack Delay Task; CFQ | weight status | BMI | GSR; FPB - > weight | ∅ Toddler inhibitory control at 24 months not prospectively associated with BMI at 30 months ∅ Parental monitoring of eating at 24 months not associated with BMI at 30 months - Child emotional overeating at 24 months associated with BMI at 30 months |
| Path 5: Child GSR and Weight | ||||||||
| Francis and Susman (2009) | United States | n = 106; Age 3–12; boys and girls | delayed gratification; inhibitory control | self-imposed waiting task; toy task | weight status | BMIz | GSR - > weight | - Children who were low on inhibitory control and delayed gratification at age 3 and 5 y had the most rapid BMIz gains from age 3 to 12 y |
| Authors | Country | Sample | Independent Variable(s) | Measure(s) | Dependent Variable(s) | Measure(s) | Direction Tested | Results |
|
| ||||||||
| Seeyave et al. (2009) | United States | n = 805; Age 4–11; boys and girls | delayed gratification | self-imposed waiting task | weight status | BMI% | GSR - > weight | - Poor delay gratification at 4 y predicted child overweight at age 11 y |
| Graziano et al. (2010) | United States | n = 57; Age 2–5.5; boys and girls | delayed gratification | self-imposed waiting task | weight status | BMIz | GSR - > weight | - Better emotion regulation and delayed gratification at 2 y associated with less increase in BMI at 5.5 y - Children with poorer emotion regulation and lower delayed gratification were more likely to be classified as overweight/at risk for overweight |
| Graziano et al. (2013) | United States | n = 195; Age 2–10; boys and girls | delayed gratification | self-imposed waiting task | weight status | BMIz | GSR - > weight | - Better delayed gratification at 2 y predicted lower levels of BMI-z at 10 y - Poor delayed gratification at age 2 y associated with increased odds for overweight by 74% at age 10 |
| Lumeng et al. (2013) | United States | n = 848; Age 4–15; boys and girls | delayed gratification | self-imposed waiting task | weight status | BMI% | GSR - > weight | + Relation between negative life events and BMI at 15 y was stronger among children with better delayed gratification versus those with poorer delayed gratification |
| Bub et al. (2016) | United States | n = 1023; Age 4.5–15; boys and girls | delayed gratification | self-imposed waiting task | weight status | BMIz | GSR - > weight | - Children with better self-regulation (composite score of delayed gratification, impulsivity, and selective attention) at 4.5 had lower BMIz gains at 8, 11, and 15 years |
| Anderson et al. (2017) | United States | n = 10,995; Age 3–11; boys and girls | parent-reported cognitive regulation | CSBQ | weight status | BMIz | GSR - > weight | ∅ Parent-reported cognitive regulation at 3 y not associated with child BMIz at 11 y |
| Anderson et al. (2018) | United States | n = 6400; Age 2–5.5; boys and girls | cognitive self-regulation | Bayley Short Form – Research Edition | weight status | BMI% | GSR - > weight | + - Highest prevalence of obesity at age 5.5 y for girls was among those with the highest and lowest self-regulation age 2 y - Highest prevalence of obesity at age 5.5 y for boys was among those who had lowest self-regulation at 2 y |
| Francis et al. (2020) | United States | n = 1007; Age 15 months-15; boys and girls | delayed gratification; inhibitory control | self-imposed waiting task; CBQ | weight status | BMI% trajectories | GSR - > weight | - Youth in the severe obesity trajectory had lower odds of parent-report of high inhibitory control than youth in the non-overweight trajectory from age 2 to 15 y ∅ No differences in odds for weight trajectories over time and delayed gratification |
Note. Bold indicates significant paths. + signified positive association; - signifies negative association; + - signifies mixed findings; ∅ signifies null findings. Constructs not outlined in the operationalization and key constructs section were not reviewed.
Abbreviations: FPB, food parenting behaviors; GSR, general self-regulation; ESR, eating self-regulation; BMI, body mass index; BMIz, body mass index z-score; BMI %, body mass index percentile; BMI-SDs, body mass index standardized; CFPQ; Comprehensive Feeding Practices Questionnaire; IFSQ, Infant Feeding Styles Questionnaire; EAH, eating in the absence of hunger; FPSQ, Feeding Practices and Structure Questionnaire; PFSQ, Parent Feeding Style Questionnaire; CEBQ, Children’s Eating Behavior Questionnaire; DXA, dual-energy x-ray absorptiometry; CFQ, Child Feeding Questionnaire; PFQ, Preschooler Feeding Questionnaire; COEQ, Control Over Eating Questionnaire; DEBQ-P, Dutch Eating Behavior Questionnaire-Parent Report; PSQ, Parenting Styles Questionnaire; RAQ, Restricted Access Questionnaire; CBQ; Child Behavior Questionnaire; CSBQ, Children’s Social Behavior Questionnaire.
3.3. Path 1: food parenting behaviors and child eating self-regulation
Of the 14 studies that examined food parenting behaviors and child eating self-regulation either alone or in combination with child weight status, all studies examined food parenting practices (Bauer et al., 2017; Berge et al., 2020; Bergmeier et al., 2015; Birch et al., 2003; Derks et al., 2019; Farrow et al., 2015; Fisher & Birch, 2002; Francis & Birch, 2005; Galindo et al., 2018; Gregory et al., 2010; Jansen et al., 2018, 2020; Rodgers et al., 2013; Steinsbekk et al., 2016).
3.3.1. Evidence for food parenting behaviors - > child eating self-regulation
3.3.1.1. EAH.
Four studies reported positive associations between food parenting practices and child EAH (Birch et al., 2003; Farrow et al., 2015; Fisher & Birch, 2002; Francis & Birch, 2005), and two studies reported mixed findings (Bauer et al., 2017; Galindo et al., 2018). In a series of longitudinal studies that examined EAH in girls, parental restriction at age 5 y was predictive of child EAH at age 7 y (Fisher & Birch, 2002) and age 9 y (Birch et al., 2003). Further, the greatest gains in EAH from ages 5 to 9 y were observed among girls with overweight whose mothers had high levels of restriction (Birch et al., 2003) and whose mothers reported high levels of restriction and had overweight (Francis & Birch, 2005). In another study of 35 preschool-aged children, parental restriction of food for health reasons and use of food as reward from ages 3 to 5 y were independently and positively associated with child EAH from ages 5 to 7 y (Farrow et al., 2015). In contrast, one longitudinal cohort study of 221 toddlers followed from 21 to 33 months (Bauer et al., 2017) reported negative associations between maternal restriction of food amount, but not food quality, at 21 months and child EAH at 27 months. However, EAH at 21 months was not associated with maternal restriction of type or quality of food at 27 or 33 months. Findings from Galindo and colleagues (Galindo et al., 2018) were also mixed. In a sample of 138 preschool-aged children followed from ages 4 to 5 y, parental prompts to eat a different food observed in the laboratory predicted child EAH approximately one year later, however, self-reported pressure to eat did not predict child EAH.
3.3.1.2. Food responsiveness.
Six studies examined the relationship of food parenting practices to child food responsiveness, two of which reported a positive association (Berge et al., 2020; Steinsbekk et al., 2016) and four reported mixed or null findings (Derks et al., 2019; Gregory et al., 2010; Jansen et al., 2018, 2020). Four studies examined the relationship between parental instrumental feeding (i.e., use of food as reward) and child food responsiveness. In a longitudinal study of 534 toddlers (Berge et al., 2020), parental instrumental feeding predicted greater child food responsiveness one year later. Additionally, in a sample of 797 children (Steinsbekk et al., 2016), greater parental instrumental feeding at age 6 y predicted greater child food responsiveness at age 8 y. Jansen and colleagues (Jansen et al., 2018) found a negative prospective association among parental instrumental feeding at age 2 y and child food responsiveness at age 3.7 y. Last, one analysis of 3643 preschoolers followed from ages 4 to 9 y found no association between parental instrumental feeding at age 4 y and child food responsiveness at age 9 y (Jansen et al., 2020).
Three studies examined the association between parental restriction and child food responsiveness. In a latent class growth analysis that identified distinct patterns of eating behaviors among 3514 children followed from ages 4 to 10 y (Derks et al., 2019), less parental pressure to eat and greater restriction were associated with patterns of increasing food responsiveness overtime. Conversely, Jansen and colleagues (Jansen et al., 2018) found a negative prospective association among parental restriction at age 2 y and child food responsiveness at age 3.7 y, and one analysis of 156 preschool-aged children ages 2 to 4 y found no association between parental restriction and food responsiveness one year later (Gregory et al., 2010). Last, one study (Jansen et al., 2018) also examined parental mealtime structure and did not report a significant relationship with food responsiveness.
3.3.1.3. Emotional overeating.
Four studies examined the association between food parenting practices and child emotional overeating (Derks et al., 2019; Jansen et al., 2020; Rodgers et al., 2013; Steinsbekk et al., 2016). Two studies reported significant, positive associations between parental instrumental feeding and long-term child emotional overeating (Jansen et al., 2020; Steinsbekk et al., 2016). Additionally, one study (Rodgers et al., 2013) found that parent emotional feeding was predictive of higher child emotional overeating over time. Finally, monitoring of food intake was negatively associated with odds of increasing emotional overeating from ages 4 to 10 y, whereas parental restriction was predictive of greater odds of increasing emotional overeating (Derks et al., 2019).
3.3.1.4. Enjoyment of food.
Three studies examined whether food parenting practices predicted child enjoyment of food (Bergmeier et al., 2015; Derks et al., 2019; Steinsbekk et al., 2016). One study (Bergmeier et al., 2015) found that parental restriction and parental pressure to eat at age 3 y did not predict child enjoyment of food at age 5 y. Similarly, Steinsbekk and colleagues (Steinsbekk et al., 2016) did not report significant prospective relationships among food parenting practices, including instrumental feeding, encouragement to eating, and control overeating, and child enjoyment of food. Last, one study (Derks et al., 2019) reported a significant, positive association between maternal restriction and increasing enjoyment of food from ages 4 to 10 y.
3.3.1.5. Desire to drink.
No studies reported on the prospective association between food parenting behaviors and child desire to drink.
3.3.2. Evidence for child eating self-regulation - > food parenting behaviors
3.3.2.1. EAH.
One study examined the relation between child EAH and food parenting practices. In their bidirectional analysis of 221 toddlers, Bauer and colleagues (Bauer et al., 2017) did not find an association between child EAH at 21 months and maternal restriction of food amount or food quality at 27 or 33 months.
3.3.2.2. Food responsiveness.
Two studies examined whether child food responsiveness predicted food parenting practices (Berge et al., 2020; Jansen et al., 2020). Jansen and colleagues (Jansen et al., 2020) found that higher food responsiveness at age 4 y was associated with greater parental instrumental feeding at age 9 y. In contrast, Berge and colleagues (Berge et al., 2020) did not find a prospective relationship between child food responsiveness and parent emotional feeding one year later among 534 preschool-aged children.
3.3.2.3. Emotional overeating.
Three studies examined whether child emotional overeating predicted food parenting practices (Jansen et al., 2020; Rodgers et al., 2013; Steinsbekk et al., 2016). Jansen and colleagues (Jansen et al., 2020) found a positive relationship between emotional overeating at age 4 y and parent instrumental feeding at age 9 y. Further, findings from another study (Rodgers et al., 2013) indicated a positive association between child emotional eating and maternal emotional feeding and covert control one year later. However, Steinsbekk and colleagues (Steinsbekk et al., 2016) did not find evidence for an association between emotional overeating at age 6 y and parent feeding practices at age 8 y.
3.3.2.4. Enjoyment of food.
One study (Steinsbekk et al., 2016) examined whether child enjoyment of food predicted food parenting practices. Results did not support an association between enjoyment of food at age 6 y and parent feeding practices at age 8 y.
3.3.2.5. Desire to drink.
No studies examined the relationship of child desire to drink to food parenting practices.
3.4. Path 2: child eating self-regulation and weight
Fifteen studies reported on child eating self-regulation and weight alone or in combination with food parenting behaviors (Bergmeier et al., 2015; Birch et al., 2003; Derks et al., 2018, 2019; Fisher & Birch, 2002; Francis & Birch, 2005; Galindo et al., 2018; Gregory et al., 2010; Jansen et al., 2020; Mallan et al., 2014; Power et al., 2020; Rodgers et al., 2013; Shunk & Birch, 2004; Steinsbekk et al., 2016; Steinsbekk & Wichstrøm, 2015).
3.4.1. Evidence for child eating self-regulation - > child weight
3.4.1.1. EAH.
Two studies examined the relationships of child EAH to weight status (Fisher & Birch, 2002; Francis & Birch, 2005). In an analysis of 192 girls followed from age 5 to 7 y, EAH at 5 y and 7 y were associated with greater odds of overweight at both time points (Fisher & Birch, 2002). Further, in a follow-up study of the same sample, girls whose mothers had overweight demonstrated a greater increase in BMI from ages 5 to 9 y compared to girls of healthy-weight mothers (Francis & Birch, 2005).
3.4.1.2. Food responsiveness.
Five studies examined the relationship of food responsiveness to weight status (Derks et al., 2018; Gregory et al., 2010; Mallan et al., 2014; Power et al., 2020; Steinsbekk & Wichstrøm, 2015). In a bidirectional analysis of 995 preschool-aged children followed from ages 4 to 8 y, higher food responsiveness at 6 y, but not enjoyment of food or emotional overeating, was associated with increased weight gain from ages 6 to 8 y (Steinsbekk & Wichstrøm, 2015). In contrast, four studies found null associations between food responsiveness and child weight status (Derks et al., 2018; Gregory et al., 2010; Mallan et al., 2014; Power et al., 2020). Two studies in toddlers followed from ages 2 to 4 y did not report a prospective association between food responsiveness and child BMIz (Gregory et al., 2010; Mallan et al., 2014). Similarly, results from a bidirectional analysis of 118 preschoolers indicated a non-significant relationship between food responsiveness and BMIz across time points from ages 4 to 8 y (Power et al., 2020). Finally, Derks and colleagues (Derks et al., 2018) found no associations between child food-approach behaviors at 4 y and changes in BMI-SD and fat mass at 10 y.
3.4.1.3. Emotional overeating.
Three studies examined the relationship of emotional overeating to weight status (Derks et al., 2018; Power et al., 2020; Steinsbekk & Wichstrøm, 2015). Findings from a bidirectional analysis among 118 preschoolers indicated a significant reciprocal relationship between emotional overeating at age 6 y and BMIz at age 8 y (Power et al., 2020). However, two bidirectional analyses (Derks et al., 2018; Steinsbekk & Wichstrøm, 2015) among preschool-aged children did not report significant prospective relationships among emotional overeating and BMI-SD or fat mass during middle childhood.
3.4.1.4. Enjoyment of food.
Of the two studies that examined the prospective association between enjoyment of food and weight status (Derks et al., 2018; Mallan et al., 2014), neither study reported significant relationships of enjoyment of food to long-term child weight status or objectively measured fat mass.
3.4.1.5. Desire to drink.
No studies examined the association between desire to drink and child weight status.
3.4.2. Evidence for child weight - > child eating self-regulation
3.4.2.1. EAH.
Two studies examined the relationship of child weight status to EAH (Galindo et al., 2018; Shunk & Birch, 2004). One longitudinal study of EAH in 153 girls found that girls at risk for overweight at age 5 y were more likely to have EAH at age 9 y compared to girls with healthy weight (Shunk & Birch, 2004). Another bidirectional analysis of 138 children found a positive association between child weight at mean age 4.7 y and EAH 18 months later (Galindo et al., 2018).
3.4.2.2. Food responsiveness.
Two studies examined the relationship of child weight to food responsiveness, and both reported positive associations (Derks et al., 2018; Steinsbekk & Wichstrøm, 2015). Findings from Steinsbekk and colleagues (Steinsbekk & Wichstrøm, 2015) indicated that child BMI at age 6 y was positively associated with food responsiveness at age 8 y. Similarly, Derks and colleagues (Derks et al., 2018) found that higher BMI-SD and fat mass at age 4 y predicted greater food responsiveness at age 10 y.
3.4.2.3. Emotional overeating.
Three studies examined the association of child weight to emotional overeating (Derks et al., 2018; Power et al., 2020; Steinsbekk & Wichstrøm, 2015). In a bidirectional analysis of child weight and food-approach behaviors (Power et al., 2020), results indicated significant reciprocal associations between child BMIz and emotional overeating at a mean age of 6.3 y and a mean age of 8.3 y, respectively. Derks and colleagues (Derks et al., 2018) also reported a significant, positive association between child weight and emotional overeating. Specifically, children with obesity at 3.5 y were more likely to demonstrate increasing patterns of emotional overeating from ages 4 to 10 y compared to children with underweight or healthy weight. In contrast, one study (Steinsbekk & Wichstrøm, 2015) did not support any significant relationships between child weight and emotional overeating.
3.4.2.4. Enjoyment of food.
Two studies examined the association of child weight to enjoyment of food, and findings were mixed (Derks et al., 2018; Steinsbekk & Wichstrøm, 2015). Derks et al. (2018) found that higher BMI-SD and fat mass at age 4 y predicted greater enjoyment of food at age 10 y. However, in an analysis of 995 children followed from ages 4 to 8 y, there were no significant relationships between child weight and enjoyment of food over time (Steinsbekk & Wichstrøm, 2015).
3.4.2.5. Desire to drink.
No studies examined the association between child weight and desire to drink.
3.5. Path 3: child general self-regulation and eating self-regulation
Only one study (Rollins et al., 2014) examined the association between general self-regulation and eating self-regulation but in combination with parent feeding and child weight (i.e., paths 3,4,5).
3.5.1. Evidence for general self-regulation - > eating self-regulation
3.5.1.1. Inhibitory control.
In a latent profile analysis that examined whether distinct patterns of parent feeding practices interacted with child inhibitory control to confer risk for EAH and weight gain in girls (Rollins et al., 2014), results showed that girls whose mothers reported setting limits on amount and types of food and restricting all snack intake had the greatest EAH at 5 y. Further, girls who were low in parent-reported inhibitory control and whose mothers either reported setting limits and restricting all snack intake or who allowed unlimited access to snacks had greatest increases in EAH and BMI from ages 5 to 7 y.
3.5.2. Evidence for eating self-regulation - > general self-regulation
No studies examined whether child eating self-regulation predicted general self-regulation over time.
3.6. Path 4 and path 5: food parenting, child general self-regulation, and child weight
No studies examined the association with food parenting and child general self-regulation alone. However, three studies examined food parenting and general self-regulation in combination with child weight (Anzman & Birch, 2009; Connell & Francis, 2014; Lelakowska et al., 2019).
3.6.1. Evidence for food parenting + child general self-regulation - > child weight
3.6.1.1. Inhibitory control.
Two studies (Anzman & Birch, 2009; Lelakowska et al., 2019) examined the interaction between food parenting and child inhibitory control to weight over time. In one analysis of 197 girls ages 5 to 15 y, low parent-reported inhibitory control at age 7 y was prospectively associated with higher gains in BMI over time. Further, BMI gains over time were the highest among girls with low inhibitory control and who reported high perceived parental control over their eating (Anzman & Birch, 2009). In contrast, one study in 169 toddlers (Lelakowska et al., 2019) reported no association between inhibitory control at 24 months and BMI at 30 months, nor an interaction between inhibitory control and parental restriction on toddler BMI.
3.6.1.2. Delayed gratification.
One study (Connell & Francis, 2014) examined the interaction between food parenting and child delayed gratification predicting child weight. In the only analysis to examine parent feeding styles in relation to child general self-regulation and weight, Connell and colleagues (Connell & Francis, 2014) reported an association between authoritarian feeding style and delayed gratification among boys only, such that boys with poor delayed gratification at age 5 y and whose mothers had an authoritarian feeding style exhibited the steepest gains in BMI from ages 5 to 15 y. However, these findings were not significant among girls.
3.6.1.3. Working memory.
No studies examined the interaction between food parenting and working memory on child weight over time.
3.6.1.4. Cognitive flexibility.
No studies examined the interaction between food parenting and cognitive flexibility on child weight over time.
3.6.1.5. Affective decision making.
No studies examined the interaction between food parenting and child affective decision making on child weight over time.
3.6.2. Evidence for child weight - > food parenting + child general self-regulation
No studies examined the association of child weight to food parenting and child general self-regulation.
3.7. Path 5: child general self-regulation and child weight
Nine studies examined the association between child general self-regulation and weight (Anderson et al., 2017; Anderson & Whitaker, 2018; Bub et al., 2016; Francis et al., 2020; Francis & Susman, 2009; Graziano et al., 2010, 2013; Lumeng et al., 2013; Seeyave et al., 2009).
3.7.1. Evidence for general self-regulation - > child weight
3.7.1.1. Inhibitory control.
Two studies examined the relationship of child inhibitory control to child weight (Francis et al., 2020; Francis & Susman, 2009). In a study of 106 children followed from ages 3 to 12 y (Francis & Susman, 2009), children who demonstrated poor inhibitory control at age 3 y during a laboratory self-control procedure demonstrated increases in BMIz across all time points. Further, children with poor inhibitory control and delayed gratification demonstrated the most rapid gains in BMIz from ages 3 to 12 y. Finally, results from a latent growth curve analysis of 1007 children indicated that children with severe obesity from ages 2 to 15 y had lower odds of parent-reported high inhibitory control at age 5 y compared to children who did not have overweight from ages 2 to 15 y (Francis et al., 2020).
3.7.1.2. Delayed gratification.
Six studies examined the association of delayed gratification to child weight (Bub et al., 2016; Francis & Susman, 2009; Graziano et al., 2010, 2013; Lumeng et al., 2013; Seeyave et al., 2009). Barring one study (Lumeng et al., 2013), results overwhelmingly supported a negative association between delayed gratification and child weight over time. Findings from one study (Francis & Susman, 2009) indicated that children with poor delayed gratification during a self-imposed waiting task at age 5 demonstrated gains in BMIz up to age 12 y, and gains in BMIz were the steepest among children who demonstrated both poor inhibitory control at age 3 y and poor delayed gratification at age 5 y. Similarly, in a longitudinal analysis of 805 children followed from ages 4 to 11 y (Seeyave et al., 2009), poor delayed gratification during a self-imposed waiting task at age 4 y predicted overweight status at age 11 y. Findings from a series of longitudinal studies in 2-year-olds (Graziano et al., 2010, 2013) found that poor delayed gratification during a self-imposed waiting task was prospectively associated with greater increases in BMIz at age 5.5 y and increased odds of overweight at age 10 y. Further, another study (Bub et al., 2016) found that children with better delayed gratification at age 4.5 y had lower BMIz gains at age 8, 11, and 15 y. In contrast, although this study examined delayed gratification as a moderator and not a predictor of child weight, Lumeng and colleagues (Lumeng et al., 2013) found a positive association between negative life events, delayed gratification, and child weight in a sample of 848 children followed from age 4 to 15 y. Specifically, the negative impact of negative life events at age 4 y on BMI at age 15 y was strongest among children who had better delayed gratification. Finally, one study (Francis et al., 2020) found no relationships of delayed gratification at age 5 y to differences in risk for overweight, obesity, or severe obesity trajectories from ages 2 to 15 y.
3.7.1.3. Global measures of general self-regulation.
In contrast to the prior studies that examined specific EF domains, two studies (Anderson et al., 2017; Anderson & Whitaker, 2018) examined general self-regulation using parent-reported global composite ratings. In a sample of 10,995 youth followed from age 3 to 11 y, Anderson and colleagues (Anderson et al., 2017) examined the association between parent-reported child general self-regulation and child weight using a composite score of cognitive self-regulation on the Child Social Behavioral Questionnaire. Results did not support an association between parent-reported child cognitive self-regulation at age 3 y and child BMIz at age 11 y. In another study of 6400 children conducted by the same research group (Anderson & Whitaker, 2018), boys who had the lowest self-regulation at age 2 y, as indicated by parent report on the Bayley Short Form, demonstrated the highest prevalence of obesity at age 5.5. y. However, findings in girls were mixed, such girls who had the highest and the lowest self-regulation at age 2 y had the highest obesity prevalence at age 5.5 y.
3.7.1.4. Working memory.
No studies examined the relationship of working memory to child weight over time.
3.7.1.5. Cognitive flexibility.
No studies examined the association of cognitive flexibility to child weight over time.
3.7.1.6. Affective decision making.
No studies examined the relationship of child affective decision making to child weight over time.
3.7.2. Evidence for child weight - > general self-regulation
No studies examined the association of child weight to general self-regulation.
4. Discussion
4.1. Summary
The purpose of this review was to synthesize longitudinal research on the links between food parenting behaviors, child eating self-regulation, and child general self-regulation to clarify their role in the development of child overweight and obesity during early childhood. The number of studies included in the current review (n = 32) demonstrates the increase in longitudinal research since Ventura and Birch’s (Ventura & Birch, 2008) call for improved casual inference on the associations between parent feeding behaviors, child eating behavior, and weight. Further, although data on the link between child eating self-regulation, general self-regulation, and weight are limited, the growing attention to the role of self-regulation as a risk factor for childhood overweight and obesity is promising for the field.
4.1.1. Summary of findings: path 1
Overall, there was overwhelming evidence to support a relationship of food parenting behaviors to child eating self-regulation, although findings varied depending on eating self-regulation dimension. The majority of studies supported a positive, prospective relationship between parental restriction and child EAH (Birch et al., 2003; Farrow et al., 2015; Fisher & Birch, 2002; Francis & Birch, 2005). These findings suggest that parental attempts to restrict the amount and type of food may be counterproductive to teaching children to eat in response to hunger and satiety cues. Some, but not all, longitudinal studies also found positive associations between parent feeding practices characterized by other dimensions of coercive control (e.g., restriction, instrumental feeding, emotional feeding) and child emotional overeating over time (Jansen et al., 2018, 2020; Steinsbekk et al., 2016), whereas food parenting practices intended to provide structure (e.g., monitoring) were negatively associated with emotional overeating (Derks et al., 2019; Rodgers et al., 2013). These findings suggest that appropriate monitoring of food intake, while not restricting food, may protect against the development of emotional overeating over time.
Surprisingly, the majority of studies that examined the association of food parenting behaviors to child food responsiveness or enjoyment of food reported mixed or null results. Inconsistent findings may reflect age-related differences in study samples. Indeed, studies that found positive associations among food parenting practices characterized by coercive control and food responsiveness or enjoyment of food investigated preschool-aged children (Berge et al., 2020; Derks et al., 2019), whereas studies that found null results or negative associations investigated toddlers (Gregory et al., 2010; Jansen et al., 2018). It is plausible that controlling food parenting practices have more of a negative effect on food responsiveness and enjoyment of food as children develop and become more susceptible to external factors in their environment that shape eating self-regulation. Examination of parent-specific predictors of child food responsiveness and enjoyment of food throughout development is an important future direction to elucidate the developmental course of these eating self-regulation domains.
There was less evidence to support an effect of child eating self-regulation on food parenting behaviors. Of the three studies that examined the relationship of child eating self-regulation to parent feeding practices (Jansen et al., 2020; Rodgers et al., 2013; Steinsbekk et al., 2016), two studies found a positive prospective relationship between child emotional overeating and parent instrumental feeding, emotional feeding, and coercive control. These findings suggest that some parents may alter their feeding practices in response to aspects of child eating self-regulation. Notably, parents who use food as a reward or to sooth may inadvertently encourage a child to eat as a way to cope with negative emotions. Teaching parents alternative strategies for consoling their child (e.g., problem solving, emotion validation, re-direction) could be an important additive component to childhood obesity prevention programming.
4.1.2. Summary of findings: path 2
Apart from studies that examined EAH, few studies supported an effect of child eating self-regulation on weight status. Indeed, the majority of studies did not find that food responsiveness, emotional eating, or enjoyment of food predicted weight over time. In contrast, there was considerable evidence consistent with an effect of child weight on eating self-regulation over time. Overall, children with greater weight and body fat in early childhood demonstrated greater food responsiveness and emotional overeating during middle childhood, whereas findings on the prospective relationship of child weight to enjoyment of food were mixed. The lack of robust support for an effect of child food-approach behaviors on weight was surprising in light of cross-sectional data that have shown positive associations between food-approach behaviors, energy intake, and weight status (Carnell & Wardle, 2007, 2008; Webber et al., 2009). It is plausible that poor eating self-regulation, independent of the influence of the feeding environment, is not substantial to pose risk for excess weight in early childhood or perhaps has a protracted effect on child weight during middle childhood. Rather, study findings suggest that certain subgroups of children who have overweight or obesity during early childhood may be more susceptible to develop food-approach behaviors in later childhood. From a prevention standpoint, these findings highlight the importance of helping children establish a healthy weight during early childhood to prevent the development of unhealthy eating behaviors during middle childhood and adolescence.
4.1.3. Summary of findings: paths 3 and 4
Overall, few longitudinal studies examined the associations between eating self-regulation and general self-regulation and food parenting behaviors and general self-regulation. Indeed, no studies examined the interaction between general- and eating self-regulation alone, and only one studied examined the association between general- and eating self-regulation in combination with food parenting behaviors and child weight (Rollins et al., 2014). Further, only three studies examined the interaction between food parenting behaviors and child general self-regulation on child weight (Anzman & Birch, 2009; Connell & Francis, 2014; Lelakowska et al., 2019). Although findings are preliminary, results from these studies indicated that children with poor inhibitory control or delayed gratification whose parents restricted or set limits around snack food were at elevated risk for gains in EAH and BMI. These findings suggest that children with impairments in aspects of both “hot” and “cool” EF may have difficulty following particularly restrictive feeding guidelines, especially when the stimulus is highly motivating/rewarding (i.e., food specific). Similarly, there was evidence to suggest that parents may use punitive strategies to help their child with poor EF regulate their eating behavior. For example, Connell and colleagues (Connell & Francis, 2014) found that parents with an authoritarian feeding style and whose children had low inhibitory control had the greatest gains in BMI. Surprisingly, despite cross-sectional and longitudinal data that have shown an association between indulgent/permissive feeding style and child weight (Frankel et al., 2014; Hughes et al., 2008, 2016, 2021), no longitudinal studies examined the association between indulgent/permissive feeding and child weight among children with poor general self-regulation. Longitudinal data are needed to examine the interaction between feeding styles, particularly authoritarian and indulgent/permissive, and child general self-regulation on child weight gain.
Taken together, preliminary data suggest that food parenting practices characterized by coercive control and an authoritarian feeding style are counterproductive to aiding the development of healthy eating self-regulation and weight over time, particularly among children with pre-existing EF impairments. Teaching parents alternative strategies to help their child with poor inhibitory control or delayed gratification engage in healthy food-related decisions (e.g., supporting autonomy, providing structure, modeling, monitoring) could be particularly useful in preventing further development of poor eating self-regulation and excess weight. However, more prospective research is needed.
4.1.4. Summary of findings: path 5
Studies overwhelmingly supported a significant, negative effect of child general self-regulation on weight, although no studies examined the effect of child weight on general self-regulation. Specifically, results showed that poor delayed gratification in early childhood was a robust predictor of gains in weight over time. Moreover, preliminary evidence from two studies suggested that poor inhibitory control in early childhood was also associated with increased weight gain (Francis et al., 2020; Francis & Susman, 2009). In line with prior reviews in older children and adolescents (Egbert et al., 2019; Hayes et al., 2018), these findings show that certain components of both “hot” and “cool” EF may be risk factors for excess weight. However, due to the dearth of data on other EF constructs including working memory, cognitive flexibility, and affective decision making, it is unclear which aspects of EF (i.e., “hot” vs. “cool”) are most central to the development of overweight and obesity. Further, given that only one study examined the overlap between child general self-regulation and eating self-regulation (Rollins et al., 2014), the mechanisms by which impairments in general self-regulation are related to excess weight are still unclear. Future research is needed to examine the bidirectional relationships between general self-regulation and eating self-regulation in relation to weight over time to determine which components are most important to target in childhood prevention and treatment programs.
4.2. Strengths and limitations
Strengths of the current review include the rigorous methodological approach to data extraction and synthesis following PRISMA guidelines, the assessment of only longitudinal studies to disentangle directionality, and the synthesis of study findings across literatures. One limitation worth noting is the selective operationalization of eating self-regulation and general self-regulation. Studies were excluded from the current review if they did not assess one of the five eating- or general self-regulation constructs (Table 1). Although intended to enhance synthesis on the most important eating self-regulation and general self-regulation constructs in children, future research should prioritize examination of other eating self-regulation constructs (e.g., loss of control eating) and general self-regulation constructs (e.g., impulsivity, reinforcing value of food) associated with parent feeding and child weight. Another limitation is that we only examined studies that investigated parenting in the context of feeding as opposed to general parenting. Thus, general parenting styles were not included in the conceptual model. Future research should include measures of both food-specific and non-food-specific parenting to clarify their associations with child eating self-regulation and weight outcomes. Last, although inclusion of longitudinal studies is a strength of the review, few studies employed an experimental design necessary to make causal claims on the direction of the paths.
4.3. Future directions
At present, there are insufficient data to support the proposed conceptual model in its totality (Fig. 1). Specifically, few studies have examined a relationship between general self-regulation and eating self-regulation (path 3) and food parenting behaviors and child general self-regulation (path 4). Further, the majority of studies on the association between child general self-regulation and weight (path 5) focused exclusively on delayed gratification and inhibitory control, which precludes understanding of the role of other aspects of “hot” and “cool” EF in the development of childhood overweight and obesity. As such, the following areas warrant further investigation (Table 4).
Table 4.
Future directions for child eating self-regulation research.
| Themes | Specific Areas for Future Research |
|---|---|
| Increase Empirical Evidence | ο Examine the overlap between general self-regulation and eating self-regulation by including measures of both constructs ο Identify specific executive functions related to child weight ο Increase longitudinal data on the association between child general self-regulation and food parenting practices and feeding styles ο Evaluate sociocultural differences in food parenting practices and feeding styles among socioeconomically diverse families o Evaluate general parenting styles as a moderator of the association between parent feeding behaviors, child eating self-regulation, and weight |
| Improve Measurement | ο Identify developmentally appropriate measurement of executive function in early childhood οCorroborate objective measures of child eating self-regulation with parent report to improve validity |
| Explore Developmental Trajectories | ο Evaluate the developmental course of child general self-regulation in relation to child eating self-regulation and weight οExamine differential developmental trajectories of child eating self-regulation by child weight status and food parenting practices and feeding styles |
| Tailor Childhood Obesity Prevention and Treatment Strategies | ο Evaluate whether improving eating self-regulation and general self-regulation prevents excess weight gain in children ο Examine whether targeting controllingfood parenting practices and feeding styles improves eating self-regulation and weight outcomes among young children with overweight/obesity ο Identify strategies to support the development of healthy eating self-regulation in socioeconomically diverse children with overweight/obesity |
At present, it remains unclear whether impairments in self-regulation are related to excess weight through deficits in top-down cognitive control processes (i.e., EF) or through deficits in eating-specific self-regulatory processes. The lack of research in this area to date is surprising considering the prominent hypothesis that impairments in EF lead to overweight and obesity through excess energy intake resulting from poor eating self-regulation. Future research should prioritize examining the overlap between general self-regulation and eating self-regulation in order to disentangle their associations and identify specific components that are the most relevant to child weight status. Further, definitions and measurement of EF constructs were inconsistent. For example, measures ranged from parent-reported questionnaires of child general self-regulatory capacities (e.g., BRIEF-SR) to computerized performance-based tasks of specific EF components. As EF is rapidly developing in younger children, a consensus from the field regarding the most developmentally appropriate measures of EF in early childhood is needed. Finally, the majority of study samples were comprised of White, Non-Hispanic youth from high socioeconomic backgrounds. Given the role of poverty on impairments in self-regulation and risk for obesity (Hails et al., 2019), examining these associations in ethnic and racially diverse youth and youth from socioeconomically diverse backgrounds is critical.
5. Conclusion
Using a developmental framework, the current review aimed to integrate findings from longitudinal studies in order to clarify the links between food parenting behaviors, child self-regulation (eating and non-eating specific), and child weight during early childhood. Overall, the majority of studies showed effects of food parenting behaviors on certain aspects of child eating self-regulation, child weight on child eating self-regulation, and child general self-regulation on child weight. However, there was minimal evidence to support associations between child general self-regulation and eating self-regulation and food parenting behaviors and general self-regulation. Further research on the developmental correlates of child eating self-regulation is needed in order to elucidate parent and child-specific targets for obesity prevention during early childhood.
Role of funding sources
This work was supported by the National Heart, Lung, and Blood Institute (T32HL130357) awarded to Denise E. Wilfley, PhD.
Footnotes
Ethical statement
IRB review was not required because no human subjects were tested.
Declaration of competing interest
None.
Data sharing and availability
The lead author has full access to the data used for the systematic review and will make it available upon request.
References
- Altman M, & Wilfley DE (2015). Evidence update on the treatment of overweight and obesity in children and adolescents. Journal of Clinical Child and Adolescent Psychology, 44(4), 521–537. 10.1080/15374416.2014.963854 [DOI] [PubMed] [Google Scholar]
- Anderson SE, Sacker A, Whitaker RC, & Kelly Y (2017). Self-regulation and household routines at age three and obesity at age eleven: Longitudinal analysis of the UK Millennium Cohort Study. International Journal of Obesity, 41(10), 1459–1466. 10.1038/ijo.2017.94 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson SE, & Whitaker RC (2018). Association of self-regulation with obesity in boys vs girls in a US national sample. JAMA Pediatrics, 172(9), 842–850. 10.1001/jamapediatrics.2018.1413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anzman SL, & Birch LL (2009). Low inhibitory control and restrictive feeding practices predict weight outcomes. The Journal of Pediatrics, 155(5), 651–656. 10.1016/j.jpeds.2009.04.052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baker JL, Olsen LW, & Sørensen TIA (2007). Childhood body-mass index and the risk of coronary heart disease in adulthood. New England Journal of Medicine, 357(23), 2329–2337. 10.1056/NEJMoa072515 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bauer KW, Haines J, Miller AL, Rosenblum K, Appugliese DP, Lumeng JC, & Kaciroti NA (2017). Maternal restrictive feeding and eating in the absence of hunger among toddlers: A cohort study. International Journal of Behavioral Nutrition and Physical Activity, 14(1), 172. 10.1186/s12966-017-0630-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berg EA (1948). A simple objective technique for measuring flexibility in thinking. The Journal of General Psychology, 39(1), 15–22. 10.1080/00221309.1948.9918159 [DOI] [PubMed] [Google Scholar]
- Berge JM, Miller J, Veblen-Mortenson S, Kunin-Batson A, Sherwood NE, & French SA (2020). A bidirectional analysis of feeding practices and eating behaviors in parent/child dyads from low-income and minority households. The Journal of Pediatrics, 221, 93–98. 10.1016/j.jpeds.2020.02.001. e20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berge JM, Tate A, Trofholz A, Fertig AR, Miner M, Crow S, & Neumark-Sztainer D (2017). Momentary parental stress and food-related parenting practices. Pediatrics, 140(6), Article e20172295. 10.1542/peds.2017-2295 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berge JM, Tate A, Trofholz A, Loth K, Miner M, Crow S, & Neumark-Sztainer D (2018). Examining variability in parent feeding practices within a low-income, racially/ethnically diverse, and immigrant population using ecological momentary assessment. Appetite, 127, 110–118. 10.1016/j.appet.2018.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bergmeier HJ, Skouteris H, Haycraft E, Haines J, & Hooley M (2015). Reported and observed controlling feeding practices predict child eating behavior after 12 months. Journal of Nutrition, 145(6), 1311–1316. 10.3945/jn.114.206268 [DOI] [PubMed] [Google Scholar]
- Birch LL, & Deysher M (1985). Conditioned and unconditioned caloric compensation: Evidence for self-regulation of food intake in young children. Learning and Motivation, 16(3), 341–355. 10.1016/0023-9690(85)90020-7. [DOI] [Google Scholar]
- Birch LL, & Deysher M (1986). Caloric compensation and sensory specific satiety: Evidence for self regulation of food intake by young children. Appetite, 7(4), 323–331. 10.1016/s0195-6663(86)80001-0 [DOI] [PubMed] [Google Scholar]
- Birch LL, & Fisher JO (1998). Development of eating behaviors among children and adolescents. Pediatrics, 101(3 Pt 2), 539–549. [PubMed] [Google Scholar]
- Birch LL, Fisher JO, & Davison KK (2003). Learning to overeat: Maternal use of restrictive feeding practices promotes girls’ eating in the absence of hunger. American Journal of Clinical Nutrition, 78(2), 215–220. 10.1093/ajcn/78.2.215 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birch LL, Fisher JO, Grimm-Thomas K, Markey CN, Sawyer R, & Johnson SL (2001). Confirmatory factor analysis of the child feeding questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite, 36(3), 201–210. 10.1006/appe.2001.0398. [DOI] [PubMed] [Google Scholar]
- Blundell J, de Graaf C, Hulshof T, Jebb S, Livingstone B, Lluch A, Mela D, Salah S, Schuring E, van der Knaap H, & Westerterp M (2010). Appetite control: Methodological aspects of the evaluation of foods. Obesity Reviews, 11(3), 251–270. 10.1111/j.1467-789X.2010.00714.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bub KL, Robinson LE, & Curtis DS (2016). Longitudinal associations between self-regulation and health across childhood and adolescence. Health Psychology, 35(11), 1235–1245. 10.1037/hea0000401 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carnell S, & Wardle J (2007). Measuring behavioural susceptibility to obesity: Validation of the child eating behaviour questionnaire. Appetite, 48(1), 104–113. 10.1016/j.appet.2006.07.075. [DOI] [PubMed] [Google Scholar]
- Carnell S, & Wardle J (2008). Appetite and adiposity in children: Evidence for a behavioral susceptibility theory of obesity. American Journal of Clinical Nutrition, 88 (1), 22–29. 10.1093/ajcn/88.1.22 [DOI] [PubMed] [Google Scholar]
- Cole PM, Ram N, & English MS (2019). Toward a unifying model of self-regulation: A developmental approach. Child Development Perspectives, 13(2), 91–96. 10.1111/cdep.12316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins C, Duncanson K, & Burrows T (2014). A systematic review investigating associations between parenting style and child feeding behaviours. Journal of Human Nutrition and Dietetics, 27(6), 557–568. 10.1111/jhn.12192 [DOI] [PubMed] [Google Scholar]
- Connell LE, & Francis LA (2014). Positive parenting mitigates the effects of poor self-regulation on body mass index trajectories from ages 4-15 years. Health Psychology, 33(8), 757–764. 10.1037/hea0000014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crone EA, & van der Molen MW (2004). Developmental changes in real life decision making: Performance on a gambling task previously shown to depend on the ventromedial prefrontal cortex. Developmental Neuropsychology, 25(3), 251–279. 10.1207/s15326942dn2503_2 [DOI] [PubMed] [Google Scholar]
- Derks IPM, Bolhuis K, Sijbrands EJG, Gaillard R, Hillegers MHJ, & Jansen PW (2019). Predictors and patterns of eating behaviors across childhood: Results from the Generation R study. Appetite, 141, 104295. 10.1016/j.appet.2019.05.026 [DOI] [PubMed] [Google Scholar]
- Derks IPM, Sijbrands EJG, Wake M, Qureshi F, van der Ende J, Hillegers MHJ, Jaddoe VWV, Tiemeier H, & Jansen PW (2018). Eating behavior and body composition across childhood: A prospective cohort study. International Journal of Behavioral Nutation and Physical Activity, 15(1), 96. 10.1186/s12966-018-0725-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Derks IP, Tiemeier H, Sijbrands EJ, Nicholson JM, Voortman T, Verhulst FC, Jaddoe VW, & Jansen PW (2017). Testing the direction of effects between child body composition and restrictive feeding practices: Results from a population-based cohort. American Journal of Clinical Nutrition, 106(3), 783–790. 10.3945/ajcn.117.156448 [DOI] [PubMed] [Google Scholar]
- Egbert AH, Creber C, Loren DM, & Bohnert AM (2019). Executive function and dietary intake in youth: A systematic review of the literature. Appetite, 139, 197–212. 10.1016/j.appet.2019.04.013 [DOI] [PubMed] [Google Scholar]
- Eichler J, Schmidt R, Poulain T, Hiemisch A, Kiess W, & Hilbert A (2019). Stability, continuity, and bi-directional associations of parental feeding practices and standardized child body mass index in children from 2 to 12 years of age. Nutrients, 11(8), 1751. 10.3390/nu11081751 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Epstein LH, McCurley J, Wing RR, & Valoski A (1990). Five-year follow-up of family-based behavioral treatments for childhood obesity. Journal of Consulting and Clinical Psychology, 58(5), 661–664. 10.1037//0022-006x.58.5.661 [DOI] [PubMed] [Google Scholar]
- Epstein LH, Paluch RA, Roemmich JN, & Beecher MD (2007). Family-based obesity treatment, then and now: Twenty-five years of pediatric obesity treatment. Health Psychology, 26(4), 381–391. 10.1037/0278-6133.26.4.381 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrow CV, Haycraft E, & Blissett JM (2015). Teaching our children when to eat: How parental feeding practices inform the development of emotional eating—A longitudinal experimental design. American Journal of Clinical Nutrition, 101(5), 908–913. 10.3945/ajcn.114.103713 [DOI] [PubMed] [Google Scholar]
- Fisher JO, & Birch LL (1999). Restricting access to foods and children’s eating. Appetite, 32(3), 405–419. 10.1006/appe.1999.0231 [DOI] [PubMed] [Google Scholar]
- Fisher JO, & Birch LL (2002). Eating in the absence of hunger and overweight in girls from 5 to 7 y of age. American Journal of Clinical Nutrition, 76(1), 226–231. 10.1093/ajcn/76.1.226 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fomon SJ, Filmer LJ, Thomas LN, Anderson TA, & Nelson SE (1975). Influence of formula concentration on caloric intake and growth of normal infants. Acta Paediatrica Scandinavica, 64(2), 172–181. 10.1111/j.1651-2227.1975.tb03818.x [DOI] [PubMed] [Google Scholar]
- Francis LA, & Birch LL (2005). Maternal weight status modulates the effects of restriction on daughters’ eating and weight. International Journal of Obesity, 29(8), 942–949. 10.1038/sj.ijo.0802935 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Francis LA, Rollins BY, Bryce CI, & Granger DA (2020). Biobehavioral dysregulation and its association with obesity and severe obesity trajectories from 2 to 15 years of age: A longitudinal study. Obesity, 28(4), 830–839. 10.1002/oby.22762 [DOI] [PubMed] [Google Scholar]
- Francis LA, & Susman EJ (2009). Self-regulation and rapid weight gain in children from age 3 to 12 years. Archives of Pediatrics and Adolescent Medicine, 163(4), 297–302. 10.1001/archpediatrics.2008.579 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frankel LA, O’Connor TM, Chen TA, Nicklas T, Power TG, & Hughes SO (2014). Parents’ perceptions of preschool children’s ability to regulate eating. Feeding style differences. Appetite, 76, 166–174. 10.1016/j.appet.2014.01.077 [DOI] [PubMed] [Google Scholar]
- Galindo L, Power TG, Beck AD, Fisher JO, O’Connor TM, & Hughes SO (2018). Predicting preschool children’s eating in the absence of hunger from maternal pressure to eat: A longitudinal study of low-income, latina mothers. Appetite, 120, 281–286. 10.1016/j.appet.2017.09.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson LY, Allen KL, Davis E, Blair E, Zubrick SR, & Byrne SM (2017). The psychosocial burden of childhood overweight and obesity: Evidence for persisting difficulties in boys and girls. European Journal of Pediatrics, 176(7), 925–933. 10.1007/s00431-017-2931-y [DOI] [PubMed] [Google Scholar]
- Gioia GA, Isquith PK, Guy SC, & Kenworthy L (2000). Behavior rating inventory of executive function. Child Neuropsychology, 6(3), 235–238. 10.1076/chin.6.3.235.3152 [DOI] [PubMed] [Google Scholar]
- Graziano PA, Calkins SD, & Keane SP (2010). Toddler self-regulation skills predict risk for pediatric obesity. International Journal of Obesity, 34(4), 633–641. 10.1038/ijo.2009.288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graziano PA, Kelleher R, Calkins SD, Keane SP, & Brien MO (2013). Predicting weight outcomes in preadolescence: The role of toddlers’ self-regulation skills and the temperament dimension of pleasure. International Journal of Obesity, 37(7), 937–942. 10.1038/ijo.2012.165 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gregory JE, Paxton SJ, & Brozovic AM (2010). Maternal feeding practices, child eating behaviour and body mass index in preschool-aged children: A prospective analysis. International Journal of Behavioral Nutrition and Physical Activity, 7, 55. 10.1186/1479-5868-7-55 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hails KA, Zhou Y, & Shaw DS (2019). The mediating effect of self-regulation in the association between poverty and child weight: A systematic review. Clinical Child and Family Psychology Review, 22(3), 290–315. 10.1007/s10567-019-00279-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hales CM, Carroll MD, Fryar CD, & Ogden CL (2017). Prevalence of obesity among adults and youth: United States, 2015-2016. NCHS Data Brief, (288), 1–8. [PubMed] [Google Scholar]
- Hales CM, Fryar CD, Carroll MD, Freedman DS, & Ogden CL (2018). Trends in obesity and severe obesity prevalence in US youth and adults by sex and age, 2007-2008 to 2015-2016. The Journal of the American Medical Association, 319(16), 1723–1725. 10.1001/jama.2018.3060 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes JF, Eichen DM, Barch DM, & Wilfley DE (2018). Executive function in childhood obesity: Promising intervention strategies to optimize treatment outcomes. Appetite, 124, 10–23. 10.1016/j.appet.2017.05.040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hongwanishkul D, Happaney KR, Lee WS, & Zelazo PD (2005). Assessment of hot and cool executive function in young children: Age-related changes and individual differences. Developmental Neuropsychology, 28(2), 617–644. 10.1207/s15326942dn2802_4 [DOI] [PubMed] [Google Scholar]
- Hughes SO, Frankel LA, Beltran A, Hodges E, Hoerr S, Lumeng J, Tovar A, & Kremers S (2013). Food parenting measurement issues: Working group consensus report. Childhood Obesity, 9 Suppl(Suppl 1), S95–S102. 10.1089/chi.2013.0032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughes SO, Power TG, O’Connor TM, Orlet Fisher J, & Chen TA (2016). Maternal feeding styles and food parenting practices as predictors of longitudinal changes in weight status in hispanic preschoolers from low-income families. Journal of Obesity, 7201082. 10.1155/2016/7201082, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughes SO, Power TG, O’Connor TM, Fisher JO, Micheli NE, & Papaioannou MA (2021). Maternal feeding style and child weight status among hispanic families with low-income levels: A longitudinal study of the direction of effects. International Journal of Behavioral Nutrition and Physical Activity, 18(1), 30. 10.1186/s12966-021-01094-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hughes SO, Power TG, Orlet Fisher J, Mueller S, & Nicklas TA (2005). Revisiting a neglected construct: Parenting styles in a child-feeding context. Appetite, 44(1), 83–92. 10.1016/j.appet.2004.08.007 [DOI] [PubMed] [Google Scholar]
- Hughes SO, Shewchuk RM, Baskin ML, Nicklas TA, & Qu H (2008). Indulgent feeding style and children’s weight status in preschool. Journal of Developmental and Behavioral Pediatrics, 29(5), 403–410. 10.1097/DBP.0b013e318182a976 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jansen PW, Derks IPM, Mou Y, van Rijen EHM, Gaillard R, Micali N, Voortman T, & Hillegers MHJ (2020). Associations of parents’ use of food as reward with children’s eating behaviour and BMI in a population-based cohort. Pediatric Obesity, 15(11), Article e12662. 10.1111/ijpo.12662 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jansen E, Williams KE, Mallan KM, Nicholson JM, & Daniels LA (2018). Bidirectional associations between mothers’ feeding practices and child eating behaviours. International Journal of Behavioral Nutrition and Physical Activity, 15(1), 3. 10.1186/s12966-018-0644-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson SL, & Birch LL (1994). Parents’ and children’s adiposity and eating style. Pediatrics, 94(5), 653–661. [PubMed] [Google Scholar]
- Kerr A, & Zelazo PD (2004). Development of “hot” executive function: The Children’s Gambling Task. Brain and Cognition, 55(1), 148–157. 10.1016/s0278-2626(03)00275-6 [DOI] [PubMed] [Google Scholar]
- Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, Wei R, Curtin LR, Roche AF, & Johnson CL (2002). 2000 CDC growth charts for the United States: Methods and development. Vital and Health Statistics, (246), 1–190. [PubMed] [Google Scholar]
- Larsen JK, Sleddens EFC, Vink JM, Fisher JO, & Kremers SPJ (2018). General parenting styles and children’s obesity risk: Changing focus. Frontiers in Psychology, 9(2119). 10.3389/fpsyg.2018.02119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lelakowska G, Kanya MJ, Balassone BR, Savoree SL, Boddy LE, Power TG, & Bridgett DJ (2019). Toddlers’ impulsivity, inhibitory control, and maternal eating-related supervision in relation to toddler body mass index: Direct and interactive effects. Appetite, 142, 104343. 10.1016/j.appet.2019.104343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liang J, Matheson BE, Kaye WH, & Boutelle KN (2014). Neurocognitive correlates of obesity and obesity-related behaviors in children and adolescents. International Journal of Obesity, 38(4), 494–506. 10.1038/ijo.2013.142 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lumeng JC, Wendorf K, Pesch MH, Appugliese DP, Kaciroti N, Corwyn RF, & Bradley RH (2013). Overweight adolescents and life events in childhood. Pediatrics, 132(6), e1506–1512. 10.1542/peds.2013-1111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madowitz J, Liang J, Peterson CB, Rydell S, Zucker NL, Tanofsky-Kraff M, Harnack L, & Boutelle KN (2014). Concurrent and convergent validity of the eating in the absence of hunger questionnaire and behavioral paradigm in overweight children. International Journal of Eating Disorders, 47(3), 287–295. 10.1002/eat.22213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mallan KM, Nambiar S, Magarey AM, & Daniels LA (2014). Satiety responsiveness in toddlerhood predicts energy intake and weight status at four years of age. Appetite, 74, 79–85. 10.1016/j.appet.2013.12.001 [DOI] [PubMed] [Google Scholar]
- Martin-Calvo N, Moreno-Galarraga L, & Martinez-Gonzalez MA (2016). Association between body mass index, waist-to-height ratio and adiposity in children: A systematic review and meta-analysis. Nutrients, 8(8). 10.3390/nu8080512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matthews SC, Simmons AN, Arce E, & Panlus MP (2005). Dissociation of inhibition from error processing using a parametric inhibitory task during functional magnetic resonance imaging. NeuroReport, 16(7), 755–760. [DOI] [PubMed] [Google Scholar]
- Mischel W, Shoda Y, & Rodriguez ML (1989). Delay of gratification in children. Science, 244(4907), 933. [DOI] [PubMed] [Google Scholar]
- Montroy JJ, Bowles RP, Skibbe LE, McClelland MM, & Morrison FJ (2016). The development of self-regulation across early childhood. Developmental Psychology, 52(11), 1744–1762. 10.1037/dev0000159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Musher-Eizenman D, & Holub S (2007). Comprehensive Feeding Practices Questionnaire: Validation of a new measure of parental feeding practices. Journal of Pediatric Psychology, 32(8), 960–972. 10.1093/jpepsy/jsm037 [DOI] [PubMed] [Google Scholar]
- Nader PR, O’Brien M, Houts R, Bradley R, Belsky J, Crosnoe R, Friedman S, Mei Z, & Susman EJ (2006). Identifying risk for obesity in early childhood. Pediatrics, 118(3), e594–e601. 10.1542/peds.2005-2801 [DOI] [PubMed] [Google Scholar]
- O’Toole S, Monks CP, & Tsermentseli S (2018). Associations between and development of cool and hot executive functions across early childhood. British Journal of Developmental Psychology, 36(1), 142–148. 10.1111/bjdp.12226 [DOI] [PubMed] [Google Scholar]
- Power TG, Hidalgo-Mendez J, Fisher JO, O’Connor TM, Micheli N, & Hughes SO (2020). Obesity risk in hispanic children: Bidirectional associations between child eating behavior and child weight status over time. Eating Behaviors, 36, 101366. 10.1016/j.eatbeh.2020.101366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinert KR, Po’e EK, & Barkin SL (2013). The relationship between executive function and obesity in children and adolescents: A systematic literature review. Journal of Obesity, 820956. 10.1155/2013/820956, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rodgers RF, Paxton SJ, Massey R, Campbell KJ, Wertheim EH, Skouteris H, & Gibbons K (2013). Maternal feeding practices predict weight gain and obesogenic eating behaviors in young children: A prospective study. International Journal of Behavioral Nutrition and Physical Activity, 10, 24. 10.1186/1479-5868-10-24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rollins BY, Loken E, Savage JS, & Birch LL (2014). Maternal controlling feeding practices and girls’ inhibitory control interact to predict changes in BMI and eating in the absence of hunger from 5 to 7 y. American Journal of Clinical Nutrition, 99(2), 249–257. 10.3945/ajcn.113.063545 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell CG, & Russell A (2020). “Food” and “non-food” self-regulation in childhood: A review and reciprocal analysis. International Journal of Behavioral Nutrition and Physical Activity, 17(1), 33. 10.1186/s12966-020-00928-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Savage JS, Rollins BY, Kugler KC, Birch LL, & Marini ME (2017). Development of a theory-based questionnaire to assess structure and control in parent feeding (SCPF). International Journal of Behavioral Nutrition and Physical Activity, 14(1), 9. 10.1186/s12966-017-0466-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seeyave DM, Coleman S, Appugliese D, Corwyn RF, Bradley RH, Davidson NS, Kaciroti N, & Lumeng JC (2009). Ability to delay gratification at age 4 years and risk of overweight at age 11 years. Archives of Pediatrics and Adolescent Medicine, 163(4), 303–308. 10.1001/archpediatrics.2009.12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shomaker LB, Tanofsky-Kraff M, Mooreville M, Reina SA, Courville AB, Field SE, Matheson BE, Brady SM, Yanovski SZ, & Yanovski JA (2013). Links of adolescent- and parent-reported eating in the absence of hunger with observed eating in the absence of hunger. Obesity, 21(6), 1243–1250. 10.1002/oby.20218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shunk JA, & Birch LL (2004). Girls at risk for overweight at age 5 are at risk for dietary restraint, disinhibited overeating, weight concerns, and greater weight gain from 5 to 9 years. Journal of the American Dietetic Association, 104(7), 1120–1126. 10.1016/j.jada.2004.04.031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simmonds M, Llewellyn A, Owen CG, & Woolacott N (2016). Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obesity Reviews, 17(2), 95–107. 10.1111/obr.12334 [DOI] [PubMed] [Google Scholar]
- Steinsbekk S, Belsky J, & Wichstrøm L (2016). Parental feeding and child eating: An investigation of reciprocal effects. Child Development, 87(5), 1538–1549. 10.1111/cdev.12546 [DOI] [PubMed] [Google Scholar]
- Steinsbekk S, & Wichstrøm L (2015). Predictors of change in BMI from the age of 4 to 8. Journal of Pediatric Psychology, 40(10), 1056–1064. 10.1093/jpepsy/jsv052 [DOI] [PubMed] [Google Scholar]
- Stroop JR (1935). Studies of interference in serial verbal reactions. Journal of Experimental Psychology, 18(6), 643–662. 10.1037/h0054651 [DOI] [Google Scholar]
- Tan CC, & Lumeng JC (2018). Associations between cool and hot executive functions and children’s eating behavior. Current Nutrition Reports, 7(2), 21–28. 10.1007/s13668-018-0224-3 [DOI] [PubMed] [Google Scholar]
- Tanofsky-Kraff M, Ranzenhofer LM, Yanovski SZ, Schvey NA, Faith M, Gustafson J, & Yanovski JA (2008). Psychometric properties of a new questionnaire to assess eating in the absence of hunger in children and adolescents. Appetite, 51(1), 148–155. 10.1016/j.appet.2008.01.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toplak ME, West RF, & Stanovich KE (2013). Practitioner review: Do performance-based measures and ratings of executive function assess the same construct? Journal of Child Psychology and Psychiatry, 54(2), 131–143. 10.1111/jcpp.12001. [DOI] [PubMed] [Google Scholar]
- Vaughn AE, Ward DS, Fisher JO, Faith MS, Hughes SO, Kremers SP, Musher-Eizenman DR, O’Connor TM, Patrick H, & Power TG (2016). Fundamental constructs in food parenting practices: A content map to guide future research. Nutrition Reviews, 74(2), 98–117. 10.1093/nutrit/nuv061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ventura AK, & Birch LL (2008). Does parenting affect children’s eating and weight status? International Journal of Behavioral Nutrition and Physical Activity, 5(1), 15. 10.1186/1479-5868-5-15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vohs KD, & Baumeister RF (2016). Handbook of self-regulation: Research, theory, and applications. Guilford Publications. [Google Scholar]
- Wardle J, Carnell S, & Cooke L (2005). Parental control over feeding and children’s fruit and vegetable intake: How are they related? Journal of the American Dietetic Association, 105(2), 227–232. 10.1016/j.jada.2004.11.006 [DOI] [PubMed] [Google Scholar]
- Wardle J, Guthrie CA, Sanderson S, & Rapoport L (2001). Development of the children’s eating behaviour questionnaire. Journal of Child Psycholgoy and Psychiatry, 42(7), 963–970. 10.1111/1469-7610.00792 [DOI] [PubMed] [Google Scholar]
- Wardle J, Sanderson S, Guthrie CA, Rapoport L, & Plomin R (2002). Parental feeding style and the inter-generational transmission of obesity risk. Obesity Research, 10(6), 453–462. 10.1038/oby.2002.63 [DOI] [PubMed] [Google Scholar]
- Webber L, Hill C, Saxton J, Van Jaarsveld CΗM, & Wardle J (2009). Eating behaviour and weight in children. International Journal of Obesity, 33(1), 21–28. 10.1038/ijo.2008.219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wechsler D (2003). Wechsler Intelligence Scale for Children 4th edition (4th ed.). Pearson. [Google Scholar]
- Wilson F, Emslie H, Burden V, Nimmo-Smith I, & Wilson BA (2004). Behavioural Assessment of the Dysexecutive Syndrome for Children (BADS-C): Utility in clinical practice? Brain Impairment, 5(1), 109. 10.3316/informit.995540428101872 [DOI] [Google Scholar]
- Yee AZ, Lwin MO, & Ho SS (2017). The influence of parental practices on child promotive and preventive food consumption behaviors: A systematic review and meta-analysis. International Journal of Behavioral Nutrition and Physical Activity, 14(1), 47. 10.1186/s12966-017-0501-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zelazo PD (2006). The dimensional change card sort (dccs): A method of assessing executive function in children. Nature Protocols, 1(1), 297–301. 10.1038/nprot.2006.46 [DOI] [PubMed] [Google Scholar]
- Zelazo PD, & Carlson SM (2012). Hot and cool executive function in childhood and adolescence: Development and plasticity. Child Development Perspectives, 6(4), 354–360. 10.1111/j.1750-8606.2012.00246.x. [DOI] [Google Scholar]
- Zelazo PD, Carlson SM, & Kesek A (2008). The development of executive function in childhood. In Handbook of developmental cognitive neuroscience (2nd ed., pp. 553–574). MIT Press. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The lead author has full access to the data used for the systematic review and will make it available upon request.