

Abstract
Patients with a history of hypertensive disorders of pregnancy (HDP) suffer higher rates of long-term cardiovascular events including heart failure, coronary artery disease, and stroke. Cardiovascular changes during pregnancy can act as a natural stress test, subsequently unmasking latent cardiovascular disease in the form of HDP. Because HDP now affect 10% of pregnancies in the United States, the American Heart Association has called for physicians who provide peripartum care to promote early identification and cardiovascular risk reduction. In this review, we discuss the epidemiology, pathophysiology, and outcomes of HDP-associated cardiovascular disease. In addition, we propose a multi-pronged approach to support cardiovascular risk reduction for women with a history of HDP. Additional research is warranted to define appropriate blood pressure targets in the postpartum period, optimize the use of pregnancy history in risk stratification tools, and clarify the effectiveness of preventive interventions. The highest rates of HDP are in populations with poor access to resources and quality health care, making it a major risk for inequity of care. Interventions to decrease long-term cardiovascular disease risk in women following HDP must also target disparity reduction.
Keywords: cardiovascular disease, hypertension, preeclampsia, pregnancy, risk factors
One in 4 cardiovascular-related deaths in women are preventable. Nevertheless, cardiovascular disease (CVD) remains the leading cause of death among women.1 Physiological changes during pregnancy may unmask asymptomatic CVD such as chronic hypertension or prediabetes. Perinatal care may be the first time a woman interacts with a medical professional2. Therefore, the peripartum period represents an important opportunity to identify women at risk for future CVD and deliver preventive health care.
Hypertensive disorders of pregnancy (HDP) include gestational hypertension, chronic hypertension (CHTN), preeclampsia, and superimposed preeclampsia, which affect ≈10% of all pregnancies in the United States.3 Gestational hypertension and preeclampsia are the most common, characterized by hypertension after 20 weeks of gestation. Preeclampsia is the leading cause of prematurity and ranks third among causes of maternal mortality worldwide.3 Additionally, in women with HDP cardiovascular events occur earlier and increase their risk of cardiac mortality.4,5 To mitigate this risk the American College of Cardiology and the American Heart Association guidelines were updated to include a history of HDP as a major risk factor for developing CVD.6 In 2017, they urgently called for collaboration between providers to promote early identification and modification of CVD in reproductive-aged women.7
This review discusses the epidemiology, pathophysiology, and outcomes of CVD associated with HDP, with attention to new-onset hypertension in pregnancy (gestational hypertension and preeclampsia). We highlight ongoing health inequity, as the highest rates of HDP are among Black women with limited access to quality health care. Finally, we propose a model for leveraging postpartum care to address CVD risk factors and integrating a history of HDP into long-term CVD risk management.
HDP CLINICAL DEFINITIONS
Hypertension during pregnancy is defined as systolic blood pressure (BP) ≥140 mm Hg and/or diastolic BP ≥90 mm Hg on 2 occasions at least 4 hours apart.3 For further description of the HDP subtypes, please see Table.
Table.
Hypertensive Disorders of Pregnancy Definitions
| Diagnosis | Criteria‡ |
|---|---|
| Chronic hypertension | Hypertension* diagnosed before 20 wks gestational age and persisting beyond 6 wks postpartum |
| Preeclampsia | Hypertension* diagnosed after 20 wks gestational age in the presence of: |
| Proteinuria† | |
| Or (in the absence of proteinuria) other signs of organ dysfunction (as described below) | |
| Preeclampsia with severe features (above criteria plus any of the following) | Severe hypertension‡ |
| Seizures (eclampsia) | |
| Thrombocytopenia (platelet count <100 000×109/L) | |
| Elevated transaminases (≥2-fold higher than the upper limit of normal) | |
| Renal insufficiency (serum creatinine >1.1 mg/dL) | |
| Pulmonary edema | |
| Headache or visual disturbance | |
| Gestational hypertension | Hypertension* diagnosed after 20 wks gestational age in the absence of proteinuria and other signs of organ dysfunction |
| Chronic hypertension with superimposed preeclampsia | Preexisting chronic hypertension that subsequently meets criteria for preeclampsia |
Hypertension is defined as systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg on 2 occasions at least 4 h apart.
Proteinuria defined as ≥300 mg/24 h or a urine protein creatinine ratio ≥0.3.
Severe hypertension defined as systolic BP ≥160 mm Hg and/or diastolic BP ≥110 mm Hg. Severe hypertension can be confirmed within a short interval to facilitate timely antihypertensive medication.
HDP PATHOPHYSIOLOGY
Although the pathogenesis of HDP is incompletely understood, disordered inflammatory responses and/or imbalanced angiogenic profiles play a role. Preeclampsia, a syndrome of multi-factorial causes, is characterized by a dysfunctional placenta that releases antiangiogenic and inflammatory factors into the maternal circulation. These soluble factors are associated with endothelial dysfunction, hypertension, and organ damage.8 Risk factors for preeclampsia include >35 years of age, nulliparity, history of preeclampsia, use of assisted reproductive technologies, and several chronic medical conditions (eg, CHTN, kidney disease, and diabetes).3 Increased maternal levels of TNF-α (tumor necrosis factor-alpha) and angiotensin II type 1 receptor autoantibodies support inflammation in preeclampsia.9,10 Male fetal sex is associated with an increased risk of preeclampsia in non-Asian mothers.11 Genetic variations in the fetal genome near FLT1 (fms-related tyrosine kinase 1), a gene involved in angiogenesis,12,13 as well as maternal polymorphisms in ACVR2a, the receptor for activin A14 may also play a role in preeclampsia pathogenesis.
Delivery (of the placenta) leads to resolution of several preeclampsia symptoms, highlighting the placental role in preeclampsia pathogenesis. During pregnancy in a patient with preeclampsia, dysregulated remodeling of the uteroplacental spiral arteries15,16 causes placental oxidative stress and ischemia with excessive release of inflammatory and anti-angiogenic factors such as sFlt1 (soluble fms-like tyrosine kinase 1).17,18 sFlt1 interferes with PlGF (placental growth factor) and vascular endothelial growth factor binding.19 Circulating sFlt1 levels are increased both during active disease and several weeks before symptom onset.20 An elevated sFlt1-to-PIGF ratio or depressed PlGF alone are increasingly used to predict risk of preeclampsia and guide management.21–24 Evidence suggests that sFlt1 levels can predict adverse pregnancy outcomes and cardiovascular dysfunction during preeclampsia and postpartum.25,26
Preeclampsia is also considered a cardiovascular system maladaptation to pregnancy.27 Preexisting cardiovascular dysfunction may lead to placental dysfunction and preeclampsia.28 Bolstering this theory, vascular lesions found in placentas of preeclamptic patients resemble early atherosclerotic plaques.16,29
CVD MECHANISMS AMONG WOMEN WITH HDP
The association between HDP and CVD is well established, especially among patients with preeclampsia.4,30,31 The increased cardiovascular demands during pregnancy (eg, increased cardiac output) may unmask latent hypertension, making pregnancy a cardiovascular stress test.32,33 However, evidence suggests that preeclampsia and other HDP also contribute independently to postpartum CVD risk.34 For example, increased levels of preeclampsia-associated inflammatory cells35 and angiotensin II type 1 receptor autoantibodies are found in preeclamptic patients several years postpartum,10,36 which may explain the independent association between preeclampsia and subsequent CVD risk. Another possible factor linking preeclampsia and myocardial dysfunction is dysregulated activin A signaling. Activin A, a marker of myocardial inflammation and fibrosis, may contribute to the pathogenesis of preeclampsia and be predictive of heart failure development.37,38 In women with HDP, elevated activin A levels correlated strongly with myocardial dysfunction and increased left ventricular mass 1-year postpartum39 and 8 to 10 years after preeclamptic pregnancy.40
It is likely that both preexisting risk factors and HDP-induced dysfunction leads to elevated CVD risk.41 Indeed, a 2010 review of ≈25000 women found that prepregnancy obesity, dyslipidemias, and BP contributed as much as HDP to future CVD risk.42 Without intervention, each HDP occurrence compounds a woman’s vascular susceptibility increasing rates of vascular dysfunction by middle age, relative to women without HDP.
LONG-TERM CARDIOVASCULAR RISK
HDP and Risk of CHTN
Patients with HDP are at higher risk for developing chronic conditions that predispose them to CVD (eg, diabetes).43–45 The risk of CHTN is 4-fold higher 1-year postpartum, and remains >2-fold higher 10 and 20 years postpartum, relative to those with normotensive pregnancies.46,47 Emerging evidence suggests that smoking, obesity, and preterm delivery may help identify HDP patients at risk of developing CHTN.48,49
HDP and Risk of Cardiovascular Events and Mortality
Long-term cardiovascular morbidity is elevated among patients with a history of HDP.4,5,50,51 In the decades that follow an HDP-complicated pregnancy, the risk of heart failure, stroke, and ischemic heart disease are ≈4-, 2-, and 2-fold higher, respectively, than in women with normotensive pregnancies.51 A 2017 meta-analysis of 22 studies and >250000 women with preeclampsia suggested that prepregnancy hypertension played a role in the later development of CVD.31 In addition, the risks for developing stroke, heart failure, and ischemic heart disease were the highest 1 to 10 years postpartum, suggesting many women with a history of HDP may experience adverse cardiac events before middle age.31 A 2017 prospective cohort study similarly observed that by 1-year postpartum, 23% of patients affected by preeclampsia had stage B heart failure.52
The effect of preeclampsia on subsequent cardiovascular disease is stronger with more severe and earlier onset.53 A 2018 meta-analysis of 22 studies found that a second pregnancy complicated by preeclampsia doubled the risks of subsequent hypertension, ischemic heart disease, and stroke, nearly tripled the risk of heart failure, and increased combined cardiovascular events by >50%.54 Fetal growth disorders (preterm and small-for-gestational age delivery) may exacerbate the already increased risk of developing CVD following an HDP.49,55,56
HDP is also associated with CVD mortality.55 A retrospective observational study of >15000 postpartum patients over a 50-year period found an increase in CVD-related death among patients with preeclampsia.50 Studies evaluating the Medical Birth Registry of Norway observed that the association between preeclampsia and cardiovascular death was highest for preterm and singleton deliveries.57,58
RACIAL DISPARITIES IN HDP AND CVD
Black women are 2.5 to 3 times more likely to die from pregnancy-related causes than their White counterparts regardless of socioeconomic status.59 Moreover, nearly every type of severe maternal morbidity is more likely among Black women with preeclampsia (eg, acute myocardial infarction, stroke, and inpatient mortality).60 A 2019 Centers for Disease Control and Prevention report argued that 60% of these deaths would have been preventable with better access to high-quality care and timely diagnosis.61 Several mechanisms including genetic predispositions and social stress have been proposed for the higher prevalence of preeclampsia among Black women.62,63 Conversely, African immigrants have lower risk for preeclampsia than their United States-born counterparts.64 Further work to identify the mechanisms by which socioeconomic and racial factors contribute to HDP and CVD risk are needed.
CARDIOVASCULAR RISK REDUCTION
In summary, women with HDP are at higher risk for cardiovascular morbidity and mortality. Although the mechanisms are unclear, the cardiovascular demands of pregnancy likely unmask latent cardiovascular risk factors and HDP fosters cardiovascular dysfunction that may occur early in the postpartum period. Thus, we recommend initiating screening and prevention among these patients as soon as possible after delivery. In addition, we provide the following strategies and timeline for improving cardiovascular risk reduction as a starting place for a formal working group recommendation (Figures 1 and 2).
Figure 1. Strategies for cardiovascular disease (CVD) risk reduction following hypertensive disorders of pregnancy.
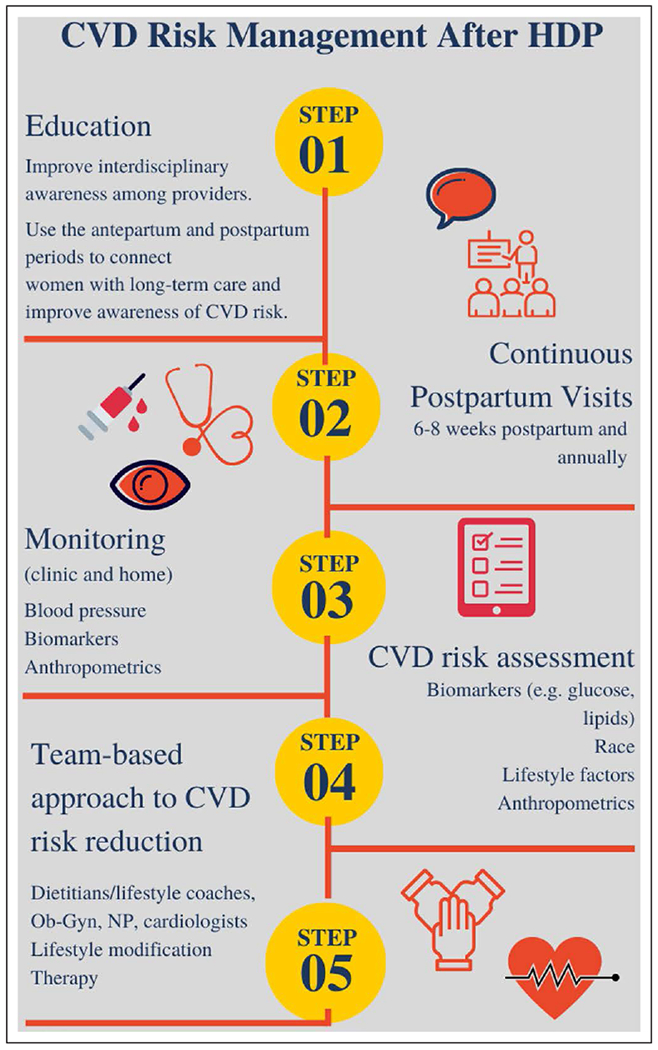
Suggested strategies include a multidisciplinary team-based approach for early identification of CVD risk factors, consistent monitoring and education. HDP indicates hypertensive disorders of pregnancy; NP, nurse practitioner; and Ob-gyn, obstetrician-gynecologist.
Figure 2. Timeline for primary prevention of cardiovascular disease (CVD) following hypertensive disorders of pregnancy.
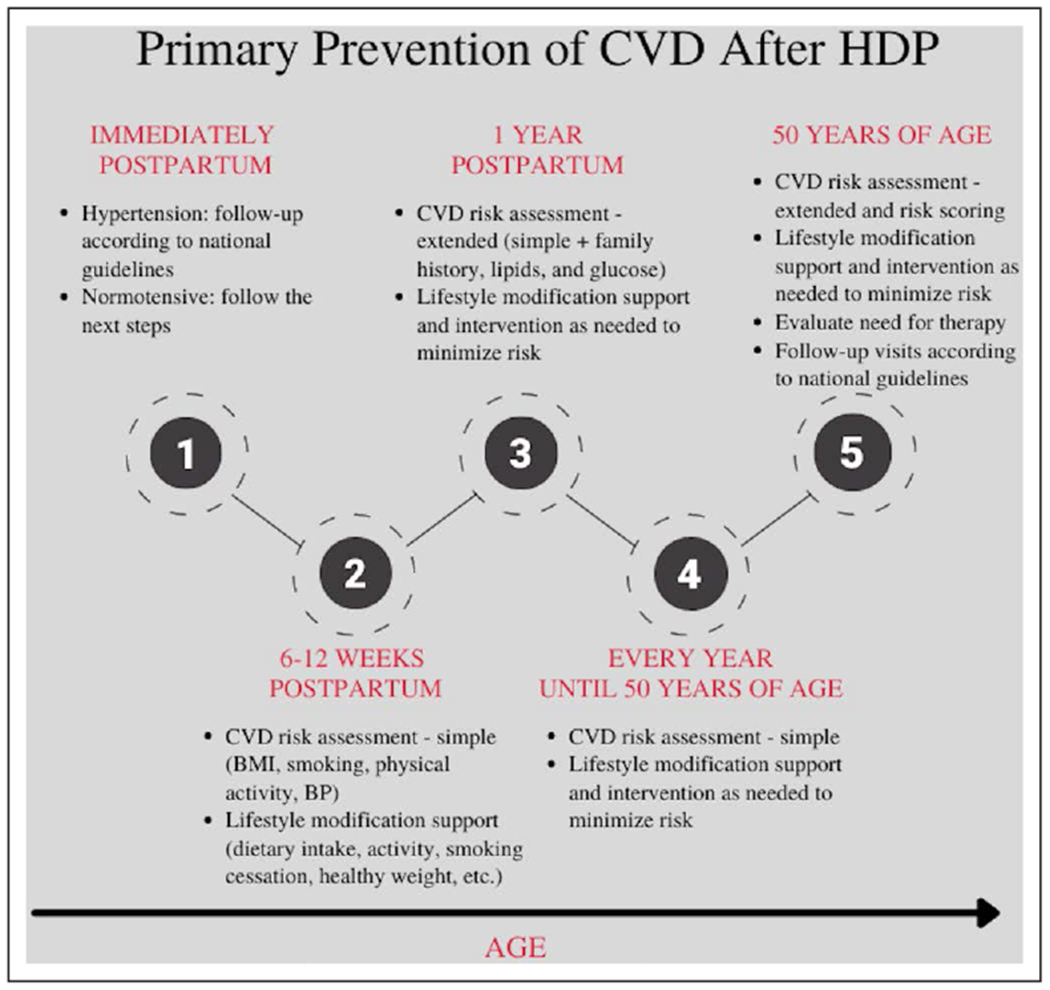
Primary prevention of CVD should start early in the postpartum period and continue throughout the women’s life. BMI indicates body mass index; BP, blood pressure; CVD, cardiovascular disease; and HDP, hypertensive disorders of pregnancy (Adapted from the Obstetrics Guidelines 2020 of the Norwegian Society of Gynecology and Obstetrics102 with permission).
Increase Awareness Among Care Providers and Patients
Providers have historically been unaware of the increased CVD risk following HDP.65,66 An HDP patient focus group reported a barrier to earlier preventative efforts was lack of CVD risk awareness among providers.67,68 Obstetrics-gynecology clinics with minority patient populations are more attuned to the risk of CVD in women with HDP.69 This finding suggests that increased CVD and multicultural competency training may increase CVD risk awareness following HDP.
Increased awareness among patients may also improve preventative efforts. We recommend that patients with HDP be educated during pregnancy, upon diagnosis, after delivery and before discharge, about their elevated risks and the importance of postpartum follow-up.68,70
Uninterrupted Postpartum Health Care
Women frequently become disconnected from ongoing medical care after delivery and may not seek care again until mid-life after CVD risks have manifested.71 Postpartum follow-up programs may allow earlier initiation of CVD preventative measures. Guidelines remain inconsistent for postpartum follow-up recommendations. The American College of Obstetricians and Gynecologists recommends that all women affected by HDP have initial contact with an obstetric care provider within 3 weeks postpartum, followed by a comprehensive postpartum visit by 12 weeks postpartum, and annual cardiovascular follow ups thereafter.72,73 The American Stroke Association74 and European Society of Hypertension75 recommend formal cardiovascular risk assessment annually after HDP but do not give immediate postpartum recommendations. Finally, the National Institute for Health and Care Excellence recommends follow-up at 6 to 8 weeks and 3 months postpartum but does not specify long-term follow-up intervals.76 The American Heart Association recommends frequent cardiovascular follow-up after an HDP but does not give a specific timeline.6 Regardless of visit timings, guidelines should stress the importance of early follow-up. We propose a plan based on follow-up within first 2 weeks postpartum, 6 to 12 weeks postpartum with specialty follow-up for residual hypertension, proteinuria, or hyperglycemia at delivery discharge, and annually thereafter for all women with HDP (Figure S1 in the Data Supplement).41
Proposed strategies for encouraging follow-up include scheduling visits at the time of delivery discharge, standardizing antihypertensive regimens, and immediate referrals to cardiology and/or primary care.41,71 Telehealth including home BP telemonitoring may also help address the deficiency in postpartum hypertension management.77 Although few studies have examined home BP telemonitoring use among patients following HDP,78–80 this technology improved BP control in nonpregnant patients.81
Racial disparities persist after delivery, with up to 60% of Black women not receiving postpartum follow-up.71,82 Factors associated with lower follow-up include Black race and <5 prenatal visits.82 Reducing follow-up barriers may improve racial disparities in postpartum morbidity and mortality. Specifically, a combination of patient and provider education, a standardized postpartum care protocols, and dedicated postpartum hypertension clinics improved follow-up and BP control among high-risk Black women, and may be useful for CVD risk reduction.83
Another barrier to postpartum follow-up is access to health insurance coverage. A recent focus group identified loss of insurance postpartum as a barrier to CVD risk reduction following HDP.68,84 In a 2016 study of 6000 patients, Medicaid or no insurance coverage was associated with 40% higher nonattendance at postpartum follow-up.85 Currently, health care coverage in the United States is not guaranteed beyond 6 weeks postpartum, which disproportionately affects Black, Hispanic, and American Indian and Alaska Native women. States with expanded Medicaid coverage under the Affordable Care Act reported a 50% reduction in infant mortality, relative to nonexpansion states, suggesting access to care may improve outcomes in women at high risk for HDP-associated CVD.86,87 In support, the state of Illinois recently expanded Medicaid benefits from 60 days to 12 months postpartum.88
Earlier Risk Identification
Recognition of the link between HDP and postpartum CVD has led to increased use of HDP-related metrics in cardiovascular risk assessment. Earlier identification of preeclampsia using biomarkers such as the sFlt1-to-PlGF ratio was discussed earlier. A 2016 study25 of 207 patients also found preeclampsia-specific antiangiogenic protein levels correlated with subclinical myocardial dysfunction during the third trimester. Other studies have observed similar findings.89–91 Adoption of these metrics may be particularly important for Black women, who have higher rates of early-onset preeclampsia, as discussed earlier.
Emerging evidence suggests that HDP-related biomarkers may also identify patients at high risk of postpartum cardiac morbidity.92 Activin A is an ongoing marker of cardiac dysfunction for at least 1-year postpartum and possibly up to 8 years after preeclampsia.37,39,93 Future work will clarify how best to use this biomarker in risk stratification and therapeutic intervention. Moreover, American College of Cardiology/American Heart Association guidelines now include gestational hypertension and preeclampsia in their CVD risk assessment.94
Evidence-Based Interventions
Although existing evidence is incomplete, postpartum BP control is associated with lower stroke risk.95 One effective intervention for postpartum BP control is furosemide.96 Observational studies suggest breastfeeding may be associated with lower postpartum BP.97 However, current evidence is insufficient to identify optimal antihypertensive medication as well as BP targets for CVD reduction. In women with diabetes, strict BP control reduces stroke and diabetes-related mortality risks,98 but the effect of BP management on HDP-related morbidity and mortality remains unclear.
Evidence supporting the use of other long-term lifestyle interventions to reduce long-term CVD risk is also lacking. National Institute for Health and Care Excellence guidelines recommend keeping body mass index between 18.5 and 24.9 before the next pregnancy for those with a history of preeclampsia,99 due to excess risk for CHTN with higher body mass index following HDP.100 The Diabetes Prevention Program, consisting of weight reduction, reduced caloric intake, and exercise, achieved comparable long-term effects on CVD risk factors as the use of metformin.101 Currently, annual BP, lipid, body mass index, and fasting glucose monitoring are recommended following HDP until the age of 50 years, after which international cardiovascular prevention guidelines apply (Figure 2).102
CONCLUSIONS
HDP are associated with an increased risk of early CVD. Although the mechanism is unclear, pregnancy may unmask latent subclinical cardiovascular risk factors in the form of pregnancy complications such as HDP. Emerging evidence suggests that HDP also independently induces cardiovascular dysfunction. Development of CVD-associated risk factors occur early after delivery and the most vulnerable period for developing CVD events occurs in the decade postpartum, before current cardiovascular screening guidelines. CVD prevention strategies must be initiated as soon as possible after delivery and before traditional CVD screening in general population.
Cardiovascular risk reduction following a HDP should involve increased education, empowerment, and awareness among patients and their providers; earlier CVD diagnosis or risk stratification; standardized postpartum care and better BP control; and evidence-based interventions to lower postpartum CVD risk and mortality (Figure 1 and Figure 2). These strategies must be implemented focused on racial and socioeconomic equity to decrease postpartum CVD burden. In addition, research is needed to clarify the pathophysiology of CVD after HDP, identify appropriate BP targets postpartum, create CVD risk stratification tools that include pregnancy history and biomarkers, and identify preventive interventions (Figure S2).
Supplementary Material
Nonstandard Abbreviations and Acronyms
- BP
blood pressure
- CHTN
chronic hypertension
- CVD
cardiovascular disease
- HDP
hypertensive disorders of pregnancy
- PlGF
placental growth factor
- sFlt1
soluble fms-like tyrosine kinase 1
- TNF-α
tumor necrosis factor-alpha
Footnotes
The Data Supplement is available with this article at https://www.ahajournals.org/doi/suppl/10.1161/HYPERTENSIONAHA.121.16506.
Disclosures
None.
REFERENCES
- 1.Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G, Ahmed M, Aksut B, Alam T, Alam K, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70:1–25. doi: 10.1016/j.jacc.2017.04.052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Levine DM, Linder JA, Landon BE. Characteristics of Americans with primary care and changes over time, 2002-2015. JAMA Intern Med. 2020;180:463–466. doi: 10.1001/jamainternmed.2019.6282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.American College of O, Gynecologists’ Committee on Practice B-O. Gestational hypertension and preeclampsia: ACOG practice bulletin, number 222. Obstet Gynecol. 2020;135:e237–e260. doi: 10.1097/AOG.0000000000003891 [DOI] [PubMed] [Google Scholar]
- 4.Ray JG, Vermeulen MJ, Schull MJ, Redelmeier DA. Cardiovascular health after maternal placental syndromes (CHAMPS): population-based retrospective cohort study. Lancet. 2005;366:1797–1803. doi: 10.1016/S0140-6736(05)67726-4 [DOI] [PubMed] [Google Scholar]
- 5.Männistö T, Mendola P Vääräsmäki M, Jävelin MR, Hartikainen AL, Pouta A, Suvanto E. Elevated blood pressure in pregnancy and subsequent chronic disease risk. Circulation. 2013;127:681–690. doi: 10.1161/CIRCULATIONAHA.112.128751 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd-Jones DM, Newby LK, Piña IL, Roger VL, Shaw LJ, et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women-2011 update: a guideline from the american heart association. Circulation. 2011;123:1243–1262. doi: 10.1161/CIR.0b013e31820faaf8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:1269–1324. doi: 10.1161/HYP0000000000000066 [DOI] [PubMed] [Google Scholar]
- 8.Rana S, Lemoine E, Granger JP, Karumanchi SA. Preeclampsia: pathophysiology, challenges, and perspectives. Circ Res. 2019;124:1094–1112. doi: 10.1161/CIRCRESAHA.118.313276 [DOI] [PubMed] [Google Scholar]
- 9.Molvarec A, Jermendy A, Nagy B, Kovács M, Várkonyi T, Hupuczi P Prohászka Z, Rigó J Jr. Association between tumor necrosis factor (TNF)-alpha G-308A gene polymorphism and preeclampsia complicated by severe fetal growth restriction. Clin Chim Acta. 2008;392:52–57. doi: 10.1016/j.cca.2008.03.009 [DOI] [PubMed] [Google Scholar]
- 10.Rieber-Mohn AB, Sugulle M, Wallukat G, Alnæs-Katjavivi P Leite Størvold G, Bolstad N, Redman CW, Dechend R, Staff AC. Auto-antibodies against the angiotensin II type I receptor in women with uteroplacental acute atherosis and preeclampsia at delivery and several years postpartum. J Reprod Immunol. 2018;128:23–29. doi: 10.1016/j.jri.2018.05.008 [DOI] [PubMed] [Google Scholar]
- 11.Jaskolka D, Retnakaran R, Zinman B, Kramer CK. Fetal sex and maternal risk of pre-eclampsia/eclampsia: a systematic review and meta-analysis. BJOG. 2017;124:553–560. doi: 10.1111/1471-0528.14163 [DOI] [PubMed] [Google Scholar]
- 12.McGinnis R, Steinthorsdottir V, Williams NO, Thorleifsson G, Shooter S, Hjartardottir S, Bumpstead S, Stefansdottir L, Hildyard L, Sigurdsson JK, et al. ; FINNPEC Consortium; GOPEC Consortium. Variants in the fetal genome near FLT1 are associated with risk of preeclampsia. Nat Genet. 2017;49:1255–1260. doi: 10.1038/ng.3895 [DOI] [PubMed] [Google Scholar]
- 13.Gray KJ, Kovacheva VP Mirzakhani H, Bjonnes AC, Almoguera B, DeWan AT, Triche EW, Saftlas AF, Hoh J, Bodian DL, et al. Gene-centric analysis of preeclampsia identifies maternal association at PLEKHG1. Hypertension. 2018;72:408–416. doi: 10.1161/HYPERTENSIONAHA.117.10688 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yong HEJ, Murthi P Brennecke SP Moses EK. Genetic approaches in preeclampsia. Methods Mol Biol. 2018;1710:53–72. doi: 10.1007/978-1-4939-7498-6_5 [DOI] [PubMed] [Google Scholar]
- 15.Redman CW, Sargent IL. Latest advances in understanding preeclampsia. Science. 2005;308:1592–1594. doi: 10.1126/science.1111726 [DOI] [PubMed] [Google Scholar]
- 16.Stanek J Histological features of shallow placental implantation unify early-onset and late-onset preeclampsia. Pediatr Dev Pathol. 2019;22:112–122. doi: 10.1177/1093526618803759 [DOI] [PubMed] [Google Scholar]
- 17.Heydarian M, McCaffrey T, Florea L, Yang Z, Ross MM, Zhou W, Maynard SE. Novel splice variants of sFlt1 are upregulated in preeclampsia. Placenta. 2009;30:250–255. doi: 10.1016/j.placenta.2008.12.010 [DOI] [PubMed] [Google Scholar]
- 18.Tomimatsu T, Mimura K, Matsuzaki S, Endo M, Kumasawa K, Kimura T. Preeclampsia: maternal systemic vascular disorder caused by generalized endothelial dysfunction due to placental antiangiogenic factors. Int J Mol Sci. 2019;20:E4246. doi: 10.3390/ijms20174246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Failla CM, Carbo M, Morea V. Positive and negative regulation of angiogenesis by soluble vascular endothelial growth factor receptor-1. Int J Mol Sci. 2018;19:E1306. doi: 10.3390/ijms19051306 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, Schisterman EF, Thadhani R, Sachs BP, Epstein FH, et al. Circulating angiogenic factors and the risk of preeclampsia. N Engl J Med. 2004;350:672–683. doi: 10.1056/NEJMoa031884 [DOI] [PubMed] [Google Scholar]
- 21.Rana S, Powe CE, Salahuddin S, Verlohren S, Perschel FH, Levine RJ, Lim KH, Wenger JB, Thadhani R, Karumanchi SA. Angiogenic factors and the risk of adverse outcomes in women with suspected preeclampsia. Circulation. 2012;125:911–919. doi: 10.1161/CIRCULATIONAHA.111.054361 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Chappell LC, Duckworth S, Seed PT, Griffin M, Myers J, Mackillop L, Simpson N, Waugh J, Anumba D, Kenny LC, et al. Diagnostic accuracy of placental growth factor in women with suspected preeclampsia: a prospective multicenter study. Circulation. 2013;128:2121–2131. doi: 10.1161/CIRCULATIONAHA.113.003215 [DOI] [PubMed] [Google Scholar]
- 23.Zeisler H, Llurba E, Chantraine F, Vatish M, Staff AC, Sennström M, Olovsson M, Brennecke SP Stepan H, Allegranza D, et al. Predictive value of the sFlt-1:PlGF ratio in women with suspected preeclampsia. N Engl J Med. 2016;374:13–22. doi: 10.1056/NEJMoa1414838 [DOI] [PubMed] [Google Scholar]
- 24.Dröge LA, Perschel FH, Stütz N, Gafron A, Frank L, Busjahn A, Henrich W, Verlohren S. Prediction of preeclampsia-related adverse outcomes with the sFlt-1 (Soluble fms-Like Tyrosine Kinase 1)/PlGF (Placental Growth Factor)-ratio in the clinical routine: a real-world study. Hypertension. 2021;77:461–471. doi: 10.1161/HYPERTENSIONAHA.120.15146 [DOI] [PubMed] [Google Scholar]
- 25.Shahul S, Medvedofsky D, Wenger JB, Nizamuddin J, Brown SM, Bajracharya S, Salahuddin S, Thadhani R, Mueller A, Tung A, et al. Circulating antiangiogenic factors and myocardial dysfunction in hypertensive disorders of pregnancy. Hypertension. 2016;67:1273–1280. doi: 10.1161/HYPERTENSIONAHA.116.07252 [DOI] [PubMed] [Google Scholar]
- 26.Ramadan H, Rana S, Mueller A, Bajracharya S, Zhang D, Salahuddin S, Nasim R, Perdigao JL, Minhaj M, Tung A, et al. Myocardial performance index in hypertensive disorders of pregnancy: the relationship between blood pressures and angiogenic factors. Hypertens Pregnancy. 2017;36:161–167. doi: 10.1080/10641955.2017.1280048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kalafat E, Thilaganathan B. Cardiovascular origins of preeclampsia. Curr Opin Obstet Gynecol. 2017;29:383–389. doi: 10.1097/GCO.0000000000000419 [DOI] [PubMed] [Google Scholar]
- 28.Thilaganathan B, Kalafat E. Cardiovascular system in preeclampsia and beyond. Hypertension. 2019;73:522–531. doi: 10.1161/HYPERTENSIONAHA.118.11191 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hecht JL, Zsengeller ZK, Spiel M, Karumanchi SA, Rosen S. Revisiting decidual vasculopathy. Placenta. 2016;42:37–43. doi: 10.1016/j.placenta.2016.04.006 [DOI] [PubMed] [Google Scholar]
- 30.Mongraw-Chaffin ML, Cirillo PM, Cohn BA. Preeclampsia and cardiovascular disease death: prospective evidence from the child health and development studies cohort. Hypertension. 2010;56:166–171. doi: 10.1161/HYPERTENSIONAHA.110.150078 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wu P Haththotuwa R, Kwok CS, Babu A, Kotronias RA, Rushton C, Zaman A, Fryer AA, Kadam U, Chew-Graham CA, et al. Preeclampsia and future cardiovascular health: a systematic review and meta-analysis. Circ Cardiovasc dual Outcomes. 2017;10:e003497. doi: 10.1161/CIRCOUTCOMES.116.003497 [DOI] [PubMed] [Google Scholar]
- 32.Williams D Pregnancy: a stress test for life. Curr Opin Obstet Gynecol. 2003;15:465–471. doi: 10.1097/00001703-200312000-00002 [DOI] [PubMed] [Google Scholar]
- 33.Rich-Edwards JW, McElrath TF, Karumanchi SA, Seely EW. Breathing life into the lifecourse approach: pregnancy history and cardiovascular disease in women. Hypertension. 2010;56:331–334. doi: 10.1161/HYPERTENSIONAHA.110.156810 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Osol G, Bernstein I. Preeclampsia and maternal cardiovascular disease: consequence or predisposition? J Vasc Res. 2014;51:290–304. doi: 10.1159/000367627 [DOI] [PubMed] [Google Scholar]
- 35.Black KD, Horowitz JA. Inflammatory markers and preeclampsia: a systematic review. Nurs Res. 2018;67:242–251. doi: 10.1097/NNR.0000000000000285 [DOI] [PubMed] [Google Scholar]
- 36.Hubel CA, Wallukat G, Wolf M, Herse F, Rajakumar A, Roberts JM, Markovic N, Thadhani R, Luft FC, Dechend R. Agonistic angiotensin II type 1 receptor autoantibodies in postpartum women with a history of preeclampsia. Hypertension. 2007;49:612–617. doi: 10.1161/01.HYP0000256565.20983.d4 [DOI] [PubMed] [Google Scholar]
- 37.Hobson SR, Acharya R, Lim R, Chan ST, Mockler J, Wallace EM. Role of activin a in the pathogenesis of endothelial cell dysfunction in preeclampsia. Pregnancy Hypertens. 2016;6:130–133. doi: 10.1016/j.preghy.2016.03.001 [DOI] [PubMed] [Google Scholar]
- 38.Roh JD, Hobson R, Chaudhari V, Quintero P Yeri A, Benson M, Xiao C, Zlotoff D, Bezzerides V, Houstis N, et al. Activin type II receptor signaling in cardiac aging and heart failure. Sci Transl Med. 2019;11:eaau8680. doi: 10.1126/scitranslmed.aau8680 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Shahul S, Ramadan H, Nizamuddin J, Mueller A, Patel V, Dreixler J, Tung A, Lang RM, Weinert L, Nasim R, et al. Activin A and late postpartum cardiac dysfunction among women with hypertensive disorders of pregnancy Hypertension. 2018;72:188–193. doi: 10.1161/HYPERTENSIONAHA.118.10888 [DOI] [PubMed] [Google Scholar]
- 40.deMartelly VA, Dreixler J, Tung A, Mueller A, Heimberger S, Fazal AA, Naseem H, Lang R, Kruse E, Yamat M, et al. Long-term postpartum cardiac function and its association with preeclampsia. J Am Heart Assoc. 2021;10:e018526. doi: 10.1161/JAHA.120.018526 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Staff AC, Redman CW, Williams D, Leeson P Moe K, Thilaganathan B, Magnus P, Steegers EA, Tsigas EZ, Ness RB, et al. ; Global Pregnancy Collaboration (CoLab). Pregnancy and long-term maternal cardiovascular health: progress through harmonization of research cohorts and biobanks. Hypertension. 2016;67:251–260. doi: 10.1161/HYPERTENSIONAHA.115.06357 [DOI] [PubMed] [Google Scholar]
- 42.Romundstad PR, Magnussen EB, Smith GD, Vatten LJ. Hypertension in pregnancy and later cardiovascular risk: common antecedents? Circulation. 2010;122:579–584. doi: 10.1161/CIRCULATIONAHA.110.943407 [DOI] [PubMed] [Google Scholar]
- 43.Lykke JA, Langhoff-Roos J, Sibai BM, Funai EF, Triche EW, Paidas MJ. Hypertensive pregnancy disorders and subsequent cardiovascular morbidity and type 2 diabetes mellitus in the mother. Hypertension. 2009;53:944–951. doi: 10.1161/HYPERTENSIONAHA.109.130765 [DOI] [PubMed] [Google Scholar]
- 44.Wen C, Metcalfe A, Anderson TJ, Johnson JA, Sigal RJ, Nerenberg KA. Measurement of lipid profiles in the early postpartum period after hypertensive disorders of pregnancy. J Clin Lipidol. 2019;13:1008–1015. doi: 10.1016/j.jacl.2019.10.002 [DOI] [PubMed] [Google Scholar]
- 45.Vikse BE, Irgens LM, Leivestad T, Skjaerven R, Iversen BM. Preeclampsia and the risk of end-stage renal disease. N Engl J Med. 2008;359:800–809. doi: 10.1056/NEJMoa0706790 [DOI] [PubMed] [Google Scholar]
- 46.Behrens I, Basit S, Melbye M, Lykke JA, Wohlfahrt J, Bundgaard H, Thilaganathan B, Boyd HA. Risk of post-pregnancy hypertension in women with a history of hypertensive disorders of pregnancy: nationwide cohort study. BMJ. 2017;358:j3078. doi: 10.1136/bmj.j3078 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Veerbeek JH, Hermes W, Breimer AY van Rijn BB, Koenen SV, Mol BW, Franx A, de Groot CJ, Koster MP Cardiovascular disease risk factors after early-onset preeclampsia, late-onset preeclampsia, and pregnancy-induced hypertension. Hypertension. 2015;65:600–606. doi: 10.1161/HYPERTENSIONAHA.114.04850 [DOI] [PubMed] [Google Scholar]
- 48.Chen KH, Chen LR. Provoking factors for postpartum chronic hypertension in women with preceding gestational hypertension/preeclampsia: a longitudinal cohort study of 22,798 pregnancies. Int J Med Sci. 2020;17:543–548. doi: 10.7150/ijms.39432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Egeland GM, Skurtveit S, Staff AC, Eide GE, Daltveit AK, Klungsøyr K, Trogstad L, Magnus PM, Brantster AL, Haugen M. Pregnancy-related risk factors are associated with a significant burden of treated hypertension within 10 years of delivery: findings from a population-based Norwegian cohort. J Am Heart Assoc. 2018;7:e008318. doi: 10.1161/JAHA.117008318 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Cirillo PM, Cohn BA. Pregnancy complications and cardiovascular disease death: 50-year follow-up of the child health and development studies pregnancy cohort. Circulation. 2015;132:1234–1242. doi: 10.1161/CIRCULATIONAHA.113.003901 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Leon LJ, McCarthy FP, Direk K, Gonzalez-Izquierdo A, Prieto-Merino D, Casas JP, Chappell L. Preeclampsia and cardiovascular disease in a large UK pregnancy cohort of linked electronic health records: a CALIBER study. Circulation. 2019;140:1050–1060. doi: 10.1161/CIRCULATIONAHA.118.038080 [DOI] [PubMed] [Google Scholar]
- 52.Breetveld NM, Ghossein-Doha C, van Kuijk SM, van Dijk AP, van der Vlugt MJ, Heidema WM, van Neer J, van Empel V, Brunner-La Rocca HP, Scholten RR, et al. Prevalence of asymptomatic heart failure in formerly pre-eclamptic women: a cohort study. Ultrasound Obstet Gynecol. 2017;49:134–142. doi: 10.1002/uog.16014 [DOI] [PubMed] [Google Scholar]
- 53.McDonald SD, Malinowski A, Zhou Q, Yusuf S, Devereaux PJ. Cardiovascular sequelae of preeclampsia/eclampsia: a systematic review and meta-analyses. Am Heart J. 2008;156:918–930. doi: 10.1016/j.ahj.2008.06.042 [DOI] [PubMed] [Google Scholar]
- 54.Brouwers L, van der Meiden-van Roest AJ, Savelkoul C, Vogelvang TE, Lely AT, Franx A, van Rijn BB. Recurrence of pre-eclampsia and the risk of future hypertension and cardiovascular disease: a systematic review and meta-analysis. BJOG. 2018;125:1642–1654. doi: 10.1111/1471-0528.15394 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Bellamy L, Casas JP, Hingorani AD, Williams DJ. Pre-eclampsia and risk of cardiovascular disease and cancer in later life: systematic review and meta-analysis. BMJ. 2007;335:974. doi: 10.1136/bmj.39335.385301.BE [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Riise HKR, Sulo G, Tell GS, Igland J, Nygård O, Iversen AC, Daltveit AK. Association between gestational hypertension and risk of cardiovascular disease among 617 589 Norwegian women. J Am Heart Assoc. 2018;7:e008337. doi: 10.1161/JAHA.117008337 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Skjaeiven R, Wilcox AJ, Klungsøyr K, Irgens LM, Vikse BE, Vatten LJ, Lie RT. Cardiovascular mortality after pre-eclampsia in one child mothers: prospective, population based cohort study. BMJ. 2012;345:e7677 doi: 10.1136/bmj.e7677 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Irgens HU, Reisaeter L, Irgens LM, Lie RT. Long term mortality of mothers and fathers after pre-eclampsia: population based cohort study. BMJ. 2001;323:1213–1217. doi: 10.1136/bmj.323.7323.1213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Johnson JD, Louis JM. Does race or ethnicity play a role in the origin, patho-physiology, and outcomes of preeclampsia? An expert review of the literature. Am J Obstet Gynecol. 2020;10:30769–9. doi: 10.1016/j.ajog.2020.07038 [DOI] [PubMed] [Google Scholar]
- 60.Shahul S, Tung A, Minhaj M, Nizamuddin J, Wenger J, Mahmood E, Mueller A, Shaefi S, Scavone B, Kociol RD, et al. Racial disparities in comorbidities, complications, and maternal and fetal outcomes in women with preeclampsia/eclampsia. Hypertens Pregnancy. 2015;34:506–515. doi: 10.3109/10641955.2015.1090581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Petersen EE, Davis NL, Goodman D, Cox S, Syverson C, Seed K, Shapiro-Mendoza C, Callaghan WM, Barfield W. Racial/ethnic disparities in pregnancy-related deaths - United States, 2007-2016. MMWR Morb Mortal Wkly Rep. 2019;68:762–765. doi: 10.15585/mmwr.mm6835a3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Zhang M, Wan P, Ng K, Singh K, Cheng TH, Velickovic I, Dalloul M, Wlody D. Preeclampsia among African American pregnant women: an update on prevalence, complications, etiology, and biomarkers. Obstet Gynecol Surv. 2020;75:111–120. doi: 10.1097/OGX.0000000000000747 [DOI] [PubMed] [Google Scholar]
- 63.Suglia SF, Staudenmayer J, Cohen S, Enlow MB, Rich-Edwards JW, Wright RJ. Cumulative stress and cortisol disruption among black and hispanic pregnant women in an urban cohort. Psychol Trauma. 2010;2:326–334. doi: 10.1037/a0018953 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Fasanya HO, Hsiao CJ, Armstrong-Sylvester KR, Beal SG. A critical review on the use of race in understanding racial disparities in preeclampsia. J Appl Lab Med. 2021;6:247–256. doi: 10.1093/jalm/jfaa149 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Young B, Hacker MR, Rana S. Physicians’ knowledge of future vascular disease in women with preeclampsia. Hypertens Pregnancy. 2012;31:50–58. doi: 10.3109/10641955.2010.544955 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Wilkins-Haug L, Celi A, Thomas A, Frolkis J, Seely EW. Recognition by women’s health care providers of long-term cardiovascular disease risk after preeclampsia. Obstet Gynecol. 2015;125:1287–1292. doi: 10.1097/AOG.0000000000000856 [DOI] [PubMed] [Google Scholar]
- 67.Seely EW, Celi AC, Chausmer J, Graves C, Kilpatrick S, Nicklas JM, Rosser ML, Rexrode KM, Stuart JJ, Tsigas E, et al. Cardiovascular health after preeclampsia: patient and provider perspective. J Womens Health (Larchmt). 2021;30:305–313. doi: 10.1089/jwh.2020.8384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Sandsæter HL, Horn J, Rich-Edwards JW Haugdahl HS. Preeclampsia, gestational diabetes and later risk of cardiovascular disease: women’s experiences and motivation for lifestyle changes explored in focus group interviews. BMC Pregnancy Childbirth. 2019;19:448. doi: 10.1186/s12884-019-2591-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Jones KM, Carter MM, Schulkin J. Racial and ethnic disparities in cardiovascular disease: an assessment of obstetrician-gynecologists’ knowledge, attitudes, and practice patterns. J Racial Ethn Health Disparities. 2015;2:256–266. doi: 10.1007/s40615-015-0088-9 [DOI] [PubMed] [Google Scholar]
- 70.Spratling PM, Pryor ER, Moneyham LD, Hodges AL, White-Williams CL, Martin JN Jr. Effect of an educational intervention on cardiovascular disease risk perception among women with preeclampsia. J Obstet Gynecol Neonatal Nurs. 2014;43:179–189. doi: 10.1111/1552-6909.12296 [DOI] [PubMed] [Google Scholar]
- 71.Bennett WL, Chang HY Levine DM, Wang L, Neale D, Werner EF, Clark JM. Utilization of primary and obstetric care after medically complicated pregnancies: an analysis of medical claims data. J Gen Intern Med. 2014;29:636–645. doi: 10.1007/s11606-013-2744-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.ACOG Committee Opinion No. 736: Optimizing Postpartum Care. Obstet Gynecol 2018;131:e140–e150. doi: 10.1097/A0G.0000000000002633 [DOI] [PubMed] [Google Scholar]
- 73.Hypertension in pregnancy. Report of the American College of Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013;122:1122–1131. doi: 10.1097/01.A0G.0000437382.03963.88 [DOI] [PubMed] [Google Scholar]
- 74.Bushnell C, McCullough LD, Awad IA, Chireau MV, Fedder WN, Furie KL, Howard VJ, Lichtman JH, Lisabeth LD, Piña IL, et al. ; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Epidemiology and Prevention; Council for High Blood Pressure Research. Guidelines for the prevention of stroke in women: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45:1545–1588. doi: 10.1161/01.str.0000442009.06663.48 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Regitz-Zagrosek V,Roos-Hesselink JW,Bauersachs J,Blomström-Lundqvist C, Crfková R, De Bonis M, lung B, Johnson MR, Kintscher U, Kranke P et al. ; ESC Scientific Document Group. 2018 ESC guidelines for the management of cardiovascular diseases during pregnancy. Eur Heart J. 2018;39:3165–3241. doi: 10.1093/eurheartj/ehy340 [DOI] [PubMed] [Google Scholar]
- 76.National Institute for Health and Care Excellence. (2019). Hypertension in pregnancy: diagnosis and management. [NG133]. https://www.nice.org.uk/guidance/ng133. [PubMed]
- 77.Hauspurg A, Lemon LS, Quinn BA, Binstock A, Larkin J, Beigi RH, Watson AR, Simhan HN. A postpartum remote hypertension monitoring protocol implemented at the hospital level. Obstet Gynecol. 2019;134:685–691. doi: 10.1097/A0G.0000000000003479 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Ganapathy R, Grewal A, Castleman JS. Remote monitoring of blood pressure to reduce the risk of preeclampsia related complications with an innovative use of mobile technology. Pregnancy Hypertens. 2016;6:263–265. doi: 10.1016/j.preghy.2016.04.005 [DOI] [PubMed] [Google Scholar]
- 79.Hirshberg A, Downes K, Srinivas S. Comparing standard office-based follow-up with text-based remote monitoring in the management of postpartum hypertension: a randomised clinical trial. BMJ Qual Saf. 2018;27:871–877. doi: 10.1136/bmjqs-2018-007837 [DOI] [PubMed] [Google Scholar]
- 80.Hirshberg A, Sammel MD, Srinivas SK. Text message remote monitoring reduced racial disparities in postpartum blood pressure ascertainment. Am J Obstet Gynecol. 2019;221:283–285. doi: 10.1016/j.ajog.2019.05.011 [DOI] [PubMed] [Google Scholar]
- 81.Margolis KL, Asche SE, Dehmer SP Bergdall AR, Green BB, Sperl-Hillen JM, Nyboer RA, Pawloski PA, Maciosek MV, Trower NK, et al. Long-term outcomes of the effects of home blood pressure telemonitoring and pharmacist management on blood pressure among adults with uncontrolled hypertension: follow-up of a cluster randomized clinical trial. JAMA Netw Open. 2018;1:e181617. doi: 10.1001/jamanetworkopen.2018.1617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Levine LD, Nkonde-Price C, Limaye M, Srinivas SK. Factors associated with postpartum follow-up and persistent hypertension among women with severe preeclampsia. J Perinatol. 2016;36:1079–1082. doi: 10.1038/jp.2016.137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Suresh SC, Duncan C, Kaur H, et al. Improved postpartum follow up with Systematic Treatment And Management of PostPartum Hypertension (STAMPP HTN). Obstetrics & Gynecology. 2021; 135:145S. doi: 10.1097/01.A0G.0000664860.13656.f6 [DOI] [PubMed] [Google Scholar]
- 84.Seely EW, Celi AC, Chausmer J, Graves C, Kilpatrick S, Nicklas JM, Rosser ML, Rexrode KM, Stuart JJ, Tsigas E, et al. Cardiovascular health after preeclampsia: patient and provider perspective. J Womens Health (Larchmt). 2021;30:305–313. doi: 10.1089/jwh.2020.8384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Wilcox A, Levi EE, Garrett JM. Predictors of non-attendance to the postpartum follow-up visit. Matern Child Health J. 2016;20(suppl 1):22–27. doi: 10.1007/s10995-016-2184-9 [DOI] [PubMed] [Google Scholar]
- 86.Searing, Adam, and Donna Cohen Ross. 2019, Medicaid Expansion Fills Gaps in Maternal Health Coverage Leading to Healthier Mothers and Babies, ccf.georgetown.edu/wp-content/uploads/2019/05/Maternal-Health-3a.pdf.
- 87.Comfort AB, Peterson LA, Hatt LE. Effect of health insurance on the use and provision of maternal health services and maternal and neonatal health outcomes: a systematic review. J Health Popul Nutr. 2013;31 (4 suppl 2):81–105. [PubMed] [Google Scholar]
- 88.Pritzker Administration Announces Illinois Is First State to Extend Full Medicaid Benefits to Mothers 12 Months Postpartum. Illinois.gov, Office of the Governor of Illinois, April 13, 2021. www2.illinois.gov/Pages/news-item.aspx?ReleaseID=23111. [Google Scholar]
- 89.Patten IS, Rana S, Shahul S, Rowe GC, Jang C, Liu L, Hacker MR, Rhee JS, Mitchell J, Mahmood F, et al. Cardiac angiogenic imbalance leads to peripartum cardiomyopathy. Nature. 2012;485:333–338. doi: 10.1038/nature11040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Garrido-Gimenez C, Mendoza M, Cruz-Lemini M, Galian-Gay L, Sanchez-Garcia O, Granato C, Rodriguez-Sureda V, Rodriguez-Palomares J, Carreras-Moratonas E, Cabero-Roura L, et al. Angiogenic factors and long-term cardiovascular risk in women that developed preeclampsia during pregnancy. Hypertension. 2020;76:1808–1816. doi: 10.1161/HYPERTENSI0NAHA.120.15830 [DOI] [PubMed] [Google Scholar]
- 91.Cong J, Fan T, Yang X, Shen J, Cheng G, Zhang Z. Maternal cardiac remodeling and dysfunction in preeclampsia: a three-dimensional speckle-tracking echocardiography study. Int J Cardiovasc Imaging. 2015;31:1361–1368. doi: 10.1007/s10554-015-0694-y [DOI] [PubMed] [Google Scholar]
- 92.Moe K, Sugulle M, Dechend R, Angel K, Staff AC. Functional and structural vascular biomarkers in women 1 year after a hypertensive disorder of pregnancy. Pregnancy Hypertens. 2020;21:23–29. doi: 10.1016/j.preghy.2020.04.008 [DOI] [PubMed] [Google Scholar]
- 93.Williamson RD, O’Keeffe GW, Kenny LC. Activin signalling and preeclampsia: from genetic risk to pre-symptomatic biomarker. Cytokine. 2015;71:360–365. doi: 10.1016/j.cyto.2014.11.017 [DOI] [PubMed] [Google Scholar]
- 94.Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, Himmelfarb CD, Khera A, Lloyd-Jones D, McEvoy JW, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140:e596–e646. doi: 10.1161/CIR.0000000000000678 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Clark SL, Christmas JT, Frye DR, Meyers JA, Perlin JB. Maternal mortality in the United States: predictability and the impact of protocols on fatal postcesarean pulmonary embolism and hypertension-related intracranial hemorrhage. Am J Obstet Gynecol. 2014;211:32 e31–39. doi: 10.1016/j.ajog.2014.03.031 [DOI] [PubMed] [Google Scholar]
- 96.Lopes Perdigao J, Lewey J, Hirshberg A, Koelper N, Srinivas SK, Elovitz MA, Levine LD. Furosemide for accelerated recovery of blood pressure postpartum in women with a hypertensive disorder of pregnancy: a randomized controlled trial. Hypertension. 2021;77:1517–1524. doi: 10.1161/HYPERTENSI0NAHA.120.16133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Bonifacino E, Schwartz EB, Jun H, Wessel CB, Corbelli JA. Effect of lactation on maternal hypertension: a systematic review. Breastfeed Med. 2018;13:578–588. doi: 10.1089/bfm.2018.0108 [DOI] [PubMed] [Google Scholar]
- 98.Mansia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, et al. ; European Society of Hypertension; European Society of Cardiology. 2007 ESH-ESC Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Blood Press. 2007;16:135–232. doi: 10.1080/08037050701461084 [DOI] [PubMed] [Google Scholar]
- 99.National Institute for Health and Care Excellence. NICE guideline: Weight management before, during and after pregnancy Accessed July, 28 2010. Available at: https://www.nice.org.uk/guidance/ph27/resources/weight-management-before-during-and-after-pregnancy-pdf-199624204640. In.
- 100.Gudmundsdottir H, Høieggen A, Stenehjem A, Waldum B, Os I. Hypertension in women: latest findings and clinical implications. Ther Adv Chronic Dis. 2012;3:137–146. doi: 10.1177/2040622312438935 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Orchard TJ, Temprosa M, Barrett-Con nor E, Fowler SE, Goldberg RB, Mather KJ, Marcovina SM, Montez M, Ratner RE, Saudek CD, et al. ; Diabetes Prevention Program 0utcomes Study Research Group. Long-term effects of the Diabetes Prevention Program interventions on cardiovascular risk factors: a report from the DPP Outcomes Study. Diabet Med. 2013;30:46–55. doi: 10.1111/j.1464-5491.2012.03750.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Norwegian Society for Gynecology and 0bstetrics. Preeclampsia patient information. Available at: https://www.legeforeningen.no/contentassets/b70edd0f6781472db2478b210cbf6e2e/pasientinfo_engelsk_preeklampsi.pdf.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.