
Fig. 4.
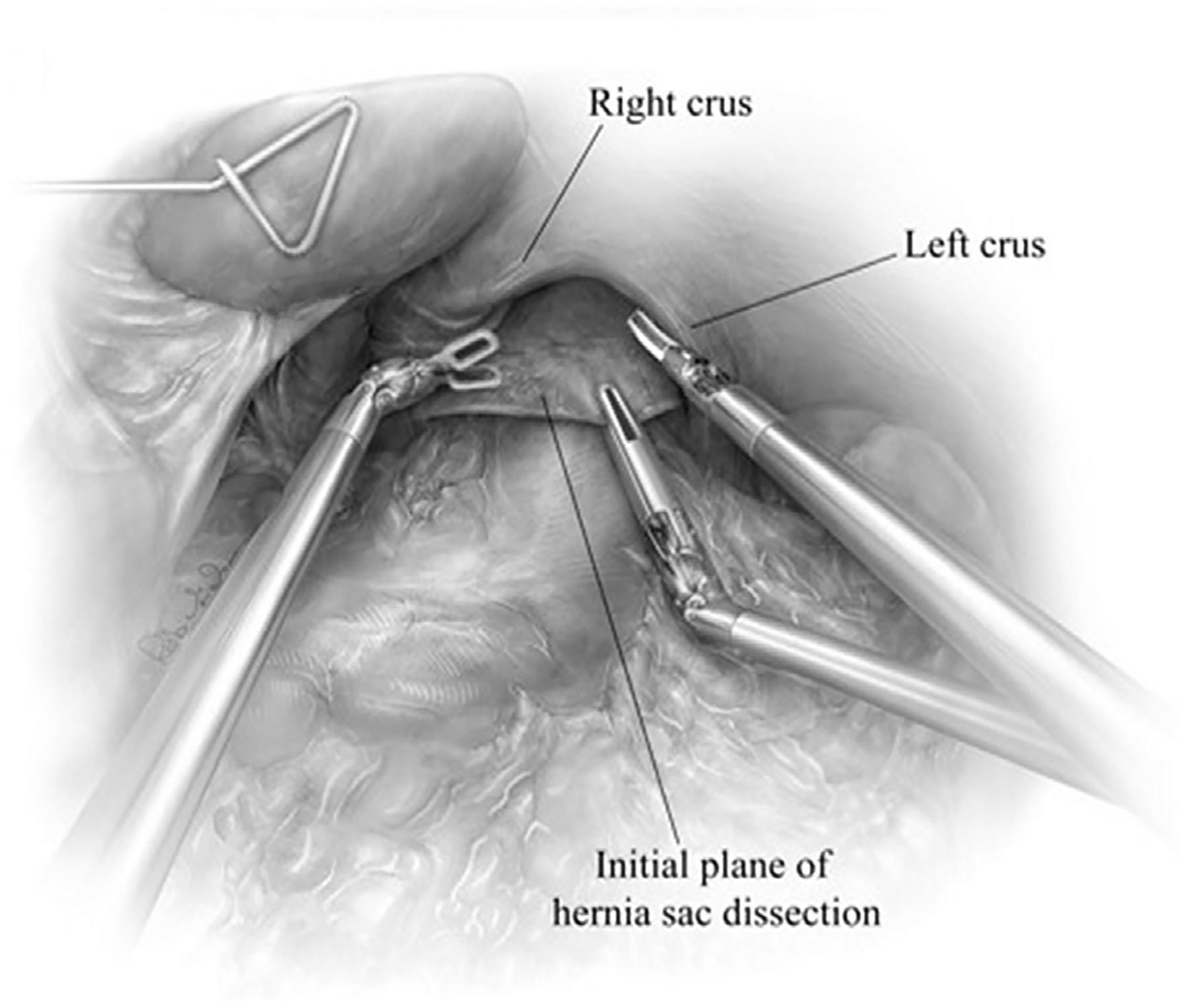
After reducing the herniated contents, the hernial defect can be well-visualized. The hernia sac along is grasped at 12 o’clock and retracted inferiorly therefore, exposing the initial line of dissection between the sac and anterior crura. Sac dissection is initiated by incising the sac just below the anterior crura and developing a plane posterior to the pericardium, with attention to the peritoneal reflection. In most hernias, the areolar plane is mobilized with blunt dissection using the ultrasonic shears. This plane is largely avascular; therefore, there should be minimal blood loss during dissection. (From Karush J, Sarkaria IS. Robotic-assisted giant paraesophageal hernia repair and Nissen fundoplication. Oper Tech Thorac Cardiovasc Surg. 2013;18(3):208; with permission.)