
Figure 3. Primary, Secondary, and Nonprespecified and Post Hoc Outcomes Comparing Omega-3 Fatty Acids and Placeboa.
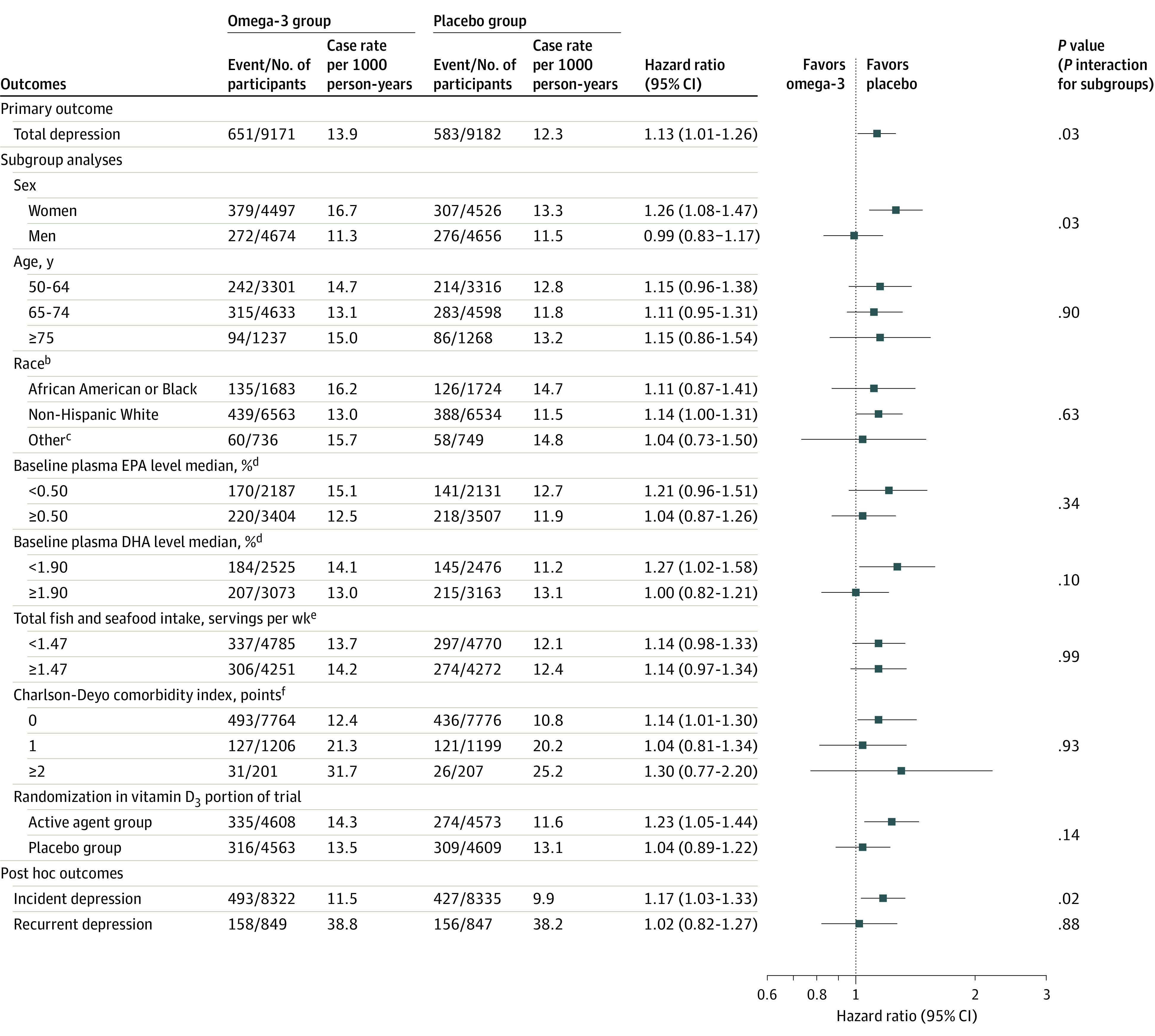
aAnalyses to compute hazard ratios (HRs) and CIs were from Cox regression models that were controlled for age, sex, and vitamin D3 randomization group; for subgroup analyses, interactions were tested using multiplicative interaction terms. Because of the potential for type I error due to multiple comparisons, findings for analyses of secondary end points and subgroups should be interpreted as exploratory. Total depression is the sum of incidence and recurrence of depression or clinically relevant depressive symptoms. Incident depression cases arose from among the 16 657 participants with no history of depression history at baseline. Recurrent depression arose from among the 1696 participants with a prior history of depression but were without clinically relevant symptoms or treatment for depression within the past 2 years at baseline.
bRace and ethnicity were self-reported by participants.
cIncluded Hispanic (not African American), Asian, Native Hawaiian or other Pacific Islander, multiple race, or unknown race or unknown ethnicity.
dBaseline plasma levels of EPA and DHA were expressed as a percent of total phospholipid fatty acids. Intake of food related to omega-3 fatty acids were assessed by modified version of Harvard food frequency questionnaire.
eThe combined category included intake of mackerel, salmon, sardines, bluefish, swordfish, canned tuna, cod, haddock, or halibut; breaded fish cakes, pieces, or fish sticks; shrimp, lobster, or scallops.
fThe Charlson-Deyo comorbidity index is a weighted comorbidity score derived from the sum of the scores for each of several major medical comorbid conditions; participants were categorized as having 0, 1, or 2 or more points.
DHA indicates docosahexaenoic acid; EPA, eicosapantaenoic acid.