

Abstract
Cannabis is the most commonly used psychotropic drug in the United States, after alcohol. Despite its apparent sedative and calming effects, cannabis and its main psychoactive constituent, Δ9-tetrahydrocannabinol (THC) can produce serious adverse effects including tachycardia and anxiety. These effects can be especially pronounced in women, who remain underrepresented in clinical cannabinoid research. The present study is one of the first to characterize the effects of single doses of oral THC on autonomic nervous system function in healthy adult women. Occasional female cannabis users participated in three laboratory sessions in which they received oral THC (7.5 mg and 15 mg) and placebo. Autonomic measures included heart rate (HR), blood pressure (BP), pre-ejection period (PEP) a measure of cardiac sympathetic functioning, and high frequency heart rate variability (HF-HRV) a measure of parasympathetic cardiac control. Autonomic responses were examined in relation to subjective drug effects. THC dose-dependently increased HR, decreased HF-HRV, and increased ratings of feeling a drug effect, cannabis-like intoxication, and anxiety. Although the drug did not significantly affect BP or PEP, HR was negatively related to both PEP and HF-HRV. HF-HRV, the measure of parasympathetic activity, was significantly negatively related to subjective measures of cannabis intoxication (but not anxiety) at the 15 mg dose only. PEP was not significantly related to any subjective measure. These results extend our knowledge of the autonomic effects of THC in relation to subjective drug experience. This and future studies will help us to understand risk factors related to cannabis use.
1. Introduction
Cannabis is the most commonly used psychotropic drug in the United States, after alcohol (SAMHSA, 2019). Due to ongoing state legalization of medicinal and, in some cases, recreational cannabis, both accessibility and use of the drug are increasing. Despite its apparent sedative and calming effects, cannabis and its main psychoactive constituent, Δ9-tetrahydrocannabinol (THC), can also produce serious adverse effects including tachycardia and anxiety (Zeiger et al., 2010; Crean et al., 2011). These effects can be especially pronounced in women (Sholler et al., 2020; Williamson & Evans, 2000). Preclinical studies suggest ovarian hormones may underlie the increased prevalence of adverse responses to cannabinoids in women (Riebe et al., 2010). As women are often excluded from clinical cannabinoid research (Kim & Menon, 2009; Greenfield et al. 2010), there is a need for additional systematic controlled studies of women to improve our understanding of gender - related physiological and subjective effects of THC, and possible adverse responses. The present study focused on the effects of single doses of oral THC on autonomic cardiac function in healthy naturally cycling adult women.
We examined the acute effects of THC on the autonomic nervous system by measuring changes in heart rate (HR) and blood pressure (BP) as well as indices of sympathetic and parasympathetic cardiac control. The sympathetic and parasympathetic systems act in concert to regulate brain and bodily functions, including those associated with mood and psychiatric symptoms (Berntson et al., 2008; Berntson et al., 1997). Sympathetic cardiac control was measured via pre-ejection period (PEP), a well validated measure of cardiac contractility (Berntson et al., 2007; Gibson, 1978). Increased sympathetic cardiac control, which is inferred from a decrease in PEP, has been related to anxiety and depressed mood as well as to anger, disgust, and fear (Cacioppo et al., 2002; Koschke et al., 2009; Light, Kothandapani, & Allen, 1998). Parasympathetic cardiac control was measured via high frequency heart rate variability (HF-HRV). Decreased parasympathetic cardiac control, which is inferred from a decrease in HF-HRV, has previously been associated with anxiety, negative mood, and emotion regulation (Berntson et al., 1997; Beauchaine & Thayer, 2015; Chalmers et al., 2014; Gorka et al., 2013; Kemp et al., 2012; Hofmann et al., 2005; 2010; Friedman, 2007). Although certain cardiovascular effects of cannabis and THC have been well documented (Jones, 2002), their effects on these particular indices of sympathetic and parasympathetic cardiac control have not been examined either specifically in women, or in relation to the subjective effects of the drug.
The acute subjective effects of cannabis and THC vary across individuals, and the drugs can produce both anxiolytic and anxiogenic effects. Although many cannabis users report that the drug decreases tension and anxiety (Ogborne et al., 2000), it can also cause acute adverse effects including paranoia, fear, and anxiety (Hindley et al., 2020; Sholler et al., 2020; Freeman et al., 2015; Karila et al., 2014; Martin-Santos et al., 2012; Hollister, 1986; Thomas, 1996). In rodents, cannabinoids activate the hypothalamic-pituitary-adrenal (HPA) axis, increase sympathetic activity, decrease parasympathetic activity, and elicit anxiety-like behaviors (Bloom & Kiernan, 1980; Patel et al. 2004). Further, studies have shown that females are more sensitive to cannabinoids (Fattore et al., 2007; Fattore et al., 2010; Craft & Leitl, 2008; Wakley & Craft, 2011) and that adverse or anxiogenic responses to cannabis and THC occur more readily in women than men (Scholler et al., 2020; Williamson & Evans, 2000). Based on these findings we would expect some women to experience anxiety after ingestion of cannabinoids, and that this will be related to increased sympathetic activity and decreased parasympathetic activity.
In this study, we examined the relationship between autonomic cardiac regulation and subjective drug response following single doses of THC, in healthy naturally cycling women. We hypothesized the drug would dose dependently increase HR, without affecting BP, and that it would increase sympathetic cardiac control and decrease parasympathetic cardiac control. Further, we hypothesized these autonomic changes would be associated with drug-induced anxiety, positively with HR and sympathetic activity and negatively with parasympathetic activity. This study will extend our knowledge of the autonomic effects of THC in relation to subjective drug experience and help us to understand risk factors related to cannabis use.
2. Method
2.1. Design
In this within-subjects study, 37 healthy females, whom were occasional cannabis users, participated in three laboratory sessions in which they received oral THC (7.5 mg, and 15 mg) and placebo. We included participants who reported using cannabis at least four times throughout their lifetime but less than 11 occasions in the past thirty days. Their subjective and cardiovascular responses to the drug were assessed during the 4-hour sessions. The primary outcome measures for this analysis were HR, BP, HF-HRV, PEP, and subjective measures of feeling the drug effect, cannabis-specific intoxication, and state anxiety. These results were collected as part of a larger study investigating the influence of menstrual cycle phase and ovarian hormones on responses to oral THC. In the larger study, subjects were randomly assigned two groups, whose sessions were scheduled during either the early follicular phase of their cycle (between days 1 to 6; Group EF, N=17) or the late follicular phase (days 9 to 14; Group LF, N=20). Although initial inspection of the data indicates that the groups did not differ in their responses to THC, we have retained the two groups as a factor in the analyses.
2.2. Participants
Healthy female recreational cannabis users (18-35 years, >4 times lifetime use and <11 uses of cannabis in past month) were recruited by posters, advertisements, and word-of-mouth referrals. Potential participants underwent a semi-structured clinical psychiatric interview (American Psychiatric Association, 2013) and provided information about current and lifetime history of drug use. Individuals taking any prescription medications, or with serious psychiatric disorders such as psychosis, generalized anxiety disorder, major depressive disorder, severe post-traumatic stress disorder or obsessive-compulsive disorder were excluded. Other exclusionary criteria were moderate or severe substance use disorder, BMI less than 19 or more than 26, abnormal resting-state ECG or HR, or pregnant or planning to be pregnant. To be included in the study, participants were required to have regular menstrual cycles and not be using hormonal contraceptives. Participants were instructed to refrain from alcohol and over-the-counter drug use for 24 hours before and 12 hours after the session, from cannabis use 7 days before and 24 hours after the session, and from all other recreational drugs 48 hours before and 24 hours after the session. Compliance was verified using breath (Alcosensor III, Intoximeters Inc., St. Louis, MO) and urine tests (ToxCup, Branan Medical Corporation, Irvine, CA). The study was approved by the local institutional review board.
2.3. Procedure
Participants first attended a pre-study orientation session to provide informed consent and become familiar with study procedures. Then they attended three 4-hour laboratory sessions, one for each drug dose condition. Participants received THC (7.5 or 15 mg) or placebo, in mixed order, under double blind conditions. Sessions were scheduled during the follicular phase of the subjects’ menstrual cycle, and were conducted in the early afternoon, separated by at least 3 days. Upon arrival at each session, participants provided urine and breath tests to confirm drug abstinence and completed baseline mood and subjective drug questionnaires. Participants provided urine samples for pregnancy and blood samples for hormone analyses (not reported here). Then, skin areas were cleaned with an alcohol prep pad for electrocardiogram (ECG) electrode placement. Disposable electrodes, made of 1/16” thick polyethylene foam and containing 7% chloride wet gel (Mindware Technologies, Gahanna, Ohio), were placed in a standard lead II configuration (Berntson et al., 2008) for the measurement of ECG and in tetrapolar electrode configuration for impedance cardiography (Sherwood et al., 1990). Signals were recorded continuously using a Mindware Mobile device at a sampling rate of 500Hz throughout the entire 4-hour experimental session. Half an hour after arrival, participants ingested a capsule containing either THC (7.5 or 15 mg THC with dextrose filler) or placebo (dextrose only) under double-blind conditions, in counterbalanced order. BP was measured using portable monitors (Omron 10 Plus, Omron Healthcare) and recorded throughout the session (−15, 30, 60, 90, 120, 180 minutes post capsule). Participants also completed subjective drug effect questionnaires at regular intervals throughout the session (−15, 30, 60, 90, 120, and 180 minutes post capsule).
2.4. Subjective Drug Effect Measures
Three measures were used to assess subjective responses to THC. To assess overall rating of a drug effect, subjects completed the Drug Effects Questionnaire (DEQ; Morean et al., 2013), indicating whether they felt a drug effect (“Feel”) on a 100 mm line labeled “not at all” (0) to “extremely” (100). To assess cannabis-specific effects, we included the Addiction Research Center Inventory (ARCI; Martin et al., 1971; Chait et al., 1985). The ARCI consisted of 53 true-false questions measuring typical effects from several classes of drugs. The scores are the number of items endorsed. For our analysis we focused on the M (marijuana) subscale which assesses cannabis (marijuana) effects. It includes 12 items such as “I have difficulty in remembering”, “My mouth feels very dry”, “I notice that my heart is beating faster”, and “My thoughts seem to come and go”. Scores range from 0 to 12 and specify the magnitude of cannabis specific intoxication symptoms a participant was experiencing. To assess anxiety, we included the Profile of Mood States (POMS, McNair et al., 1971). The POMS consists of 72 adjectives which the subjects’ rate on a 5-point scale from “not at all” (0) to “extremely” (4). These adjectives are factor analyzed into 8 scales based on the average scores rated. We focused our analyses on the Anxiety subscale, which included 9 items and a score range of 0 to 36, with a larger score indicating a greater magnitude of state anxiety.
2.5. ECG and Impedance Cardiography Signal Analysis
ECG and thoracic impedance (Z0) signals were processed and analyzed using Mindware Heart Rate Variability Analysis Software (version 3.1.1) and Cardiac Impedance Software (version 3.1.5) respectively. The ECG waveform was passed through a band pass filter from 0.25 to 40 Hz to eliminate muscle noise, a notch filter at 60 Hz to eliminate ambient electrical noise, and then visually inspected for artifacts. If movement artifacts were identified as visible disturbances in the waveform that prevented the algorithm from identifying the R-peaks, the peaks were then manually corrected in accordance with standardized guidelines (Berntson et al., 1997). From the resultant clean waveform we derived HR in beats per minute (BPM) as well as HF-HRV. In order to derive HF-HRV, the software first prepared the interbeat interval (IBI) series for spectral analysis as follows: each IBI series was interpolated and sampled at 4 Hz to ensure adequate resolution of the appropriate frequencies and equal intervals between samples, and then de-trended with a quadratic function to ensure stationarity (full details of this procedure in Berntson et al., 1997). This signal was brought into the frequency domain using a fast Fourier transform, and integrating the power over the respiratory frequency band (0.12 to 0.40 Hz) and then natural log transformed to provide the measurement we report as HF-HRV. The impedance signal was passed through the same noise filters and then the derivation was taken in order to produce a dZ/dt waveform for analysis. The dZ/dt waveform was then ensemble averaged with the ECG waveform to provide an estimate of PEP in milliseconds (ms). PEP is measured as the time between the electrical innervation of the left ventricle (Q-point on the ECG waveform) and the opening of the aortic valve (B-notch on the dZ/dt waveform). The Q-point and B-notch were then calculated using standardized procedures (Berntson et al., 2004; Lozano et al., 2007). As previously described (Berntson et al., 1997), autonomic measures were scored minute-by-minute and then collapsed into 5-minute epochs every 30 minutes throughout the 4-hour session.
2.6. Statistical Analyses
2.6.1. Time course of autonomic and subjective drug effects.
Due to errors in impedance cardiography signal collection, 8 participants did not have complete PEP data. Effects of oral THC across the 4-hour session on autonomic measures (HR, Systolic BP, Diastolic BP, HF-HRV, PEP) and subjective measures (“feel drug”, M scale, state anxiety) were analyzed using covariance pattern models with Toeplitz covariance structures. Time (Linear and quadratic) effects were included to allow for analysis of linear or curvilinear trends across time. All analyses were completed in IBM SPSS statistical software (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp). Mixed effects models offer significant advantages relative to traditional repeated-measures ANOVA in handling of missing data, relaxation of assumptions of homogeneity of variance, and increased statistical power for smaller sample sizes. All autonomic effects models (HR, Systolic BP, Diastolic BP, HF-HRV, PEP) and subjective effects models (“feel drug”, M Scale, state anxiety) included the effect of drug and time (linear and quadratic) effects as independent fixed variables. The effect of drug in all models were contrasts between placebo and 7.5 mg THC and placebo and 15 mg THC. All models also accounted for age, BMI, race (Caucasian, African American, Other), average daily caffeine and nicotine consumption within the past month, lifetime cannabis use and menstrual cycle phase (early follicular vs. late follicular) as potential covariates. Effect sizes are reported as unstandardized coefficients (B) with standard errors (SE).
2.6.3. Relationships between autonomic and subjective effects of the drug.
Cronbach’s alpha analyses were conducted to determine internal consistency among the 12 ARCI items included in the M scale and the 9 POMS items included in the Anxiety scale. Summary measures of peak change from baseline score (PCS) were calculated for each subject’s autonomic and subjective measures. PCS’s were calculated by subtracting the pre-capsule measure from the highest or lowest value after drug administration. Placebo session PCS’s were subtracted from THC conditions (7.5 and 15 mg) to yield peak change difference scores (PCDS). Relationships between autonomic and subjective outcome measures were examined by conducting linear regression analyses, separately for the 7.5 mg and 15 mg doses. Potential covariates, age, BMI, race, average daily caffeine and nicotine consumption within the past month, lifetime cannabis use and menstrual cycle phase (early follicular vs. late follicular) were evaluated in each regression and only reported if significant. Effect sizes are reported as unstandardized coefficients (B) with standard errors (SE).
3. Results
3.1. Participant Characteristics
Demographic data for the participants can be found in Table 1.
Table 1.
Participant characteristics, including demographic characteristics and recent drug use history. All subjects were female. Values shown are mean and standard deviation
| Age | 23.6 (4.5) |
| Education (years) | 15.2 (2.1) |
| Physical | |
| Body mass index (BMI) | 22.9 (2.5) |
| Weight (lbs.) | 138.9 (19.2) |
| Height (inches) | 64.6 (3.3) |
| Race | |
| Caucasian | 56.8% |
| African American | 21.6% |
| Asian | 10.8% |
| Other / More than one race | 10.8% |
| Recent (past month) substance use, mean (SD) | |
| Caffeine (cups/day) n=35 | 1.6 (0.8) |
| Tobacco cigarettes (cigs/day) n=7 | 6.1 (6.5) |
| Alcohol (days/week) n=35 | 2.0 (1.3) |
| Cannabis (times/month) n=24 | 3.8 (6.0) |
Note. Results presented as mean (SD) unless otherwise noted.
3.2. Autonomic Drug Effects
At both the 7.5 mg and 15 mg THC condition, HR significantly increased across session time compared to placebo (BTime*7.5 mg = 0.95, SE = 0.46, p = 0.04, 95% CI [0.03, 1.88]; BTime*15 mg = 1.88, SE = 0.58, p = 0.002, 95% CI [0.72, 3.04]; Figure 1A). BMI was the only significant covariate within the HR model (BBMI = −0.90, SE = 0.44, p = 0.05, 95% CI [−1.77, −0.02]). Follow up Bonferroni corrected t-tests comparing drug to placebo at each time point indicated that the 15 mg dose increased HR from 90-180 minutes post-capsule. THC did not significantly affect systolic or diastolic BP across session time, at either dose, compared to placebo. At both doses, THC decreased HF-HRV across session time compared to placebo (BTime*7.5 mg = −0.10, SE = 0.04, p = 0.009, 95% CI [−0.18, −0.03]; BTime*15 mg = −0.17, SE = 0.05, p = 0.002, 95% CI [−0.27, −0.07]; Figure 1B). Follow up t-tests indicated that the 15 mg dose decreased HF-HRV compared to placebo from 60-180 minutes post-capsule. Neither the 7.5 mg nor 15 mg dose significantly affected PEP across session time compared to placebo. Autonomic effects of THC were not related to menstrual cycle phase. The summary PCDS measures for the two doses are presented in Table 2.
Figure 1.
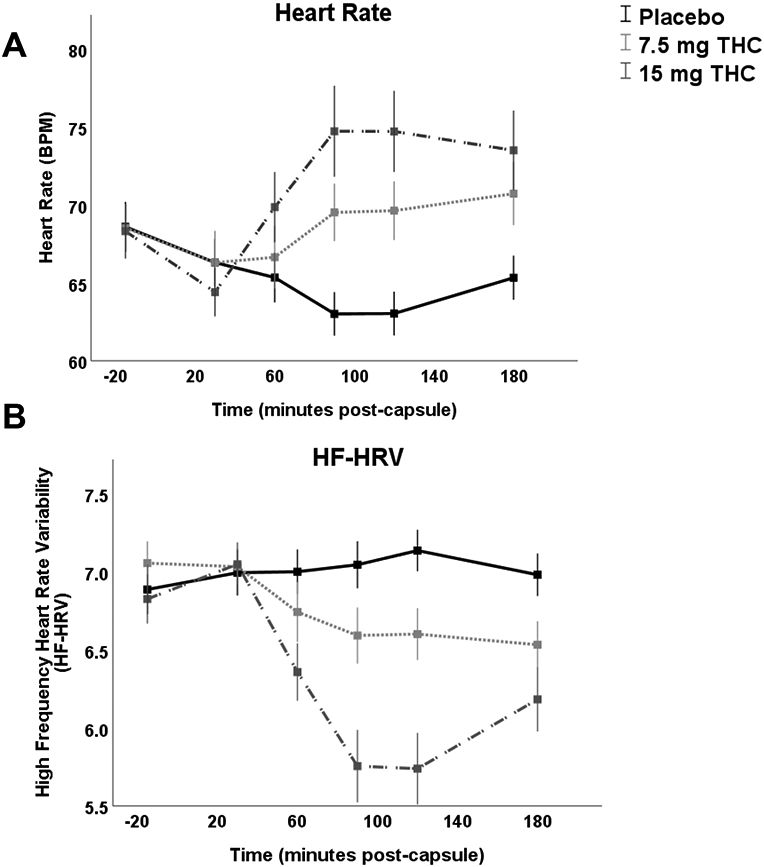

THC dose-dependently increased HR (A) and decreased HF-HRV (B), with no consistent effect on PEP (C), reported as means with standard error of the mean (SEM).
Table 2.
Peak change difference scores for autonomic and subjective effects
| Measure | Mean Placebo PCS (SD) |
Mean 7.5 mg THC PCS (SD) |
Mean 15 mg THC PCS (SD) | Mean 7.5 mg – Placebo PCDS (SD) |
Mean 15 mg – Placebo PCDS (SD) |
|---|---|---|---|---|---|
| HR | −6.2 (9.2) |
1.9
*
(13.9) |
9.6
**
(14.3) |
8.1 (17.6) |
15.8 (18.9) |
| HF-HRV | 0.2 (1.1) |
−1.0
**
(1.0) |
−1.5
**
(1.6) |
−1.2 (1.6) |
−1.7 (2.2) |
| PEP | −0.7 (16.1) | 0.6 (24.3) | −2.9 (19.4) | 1.8 (23.2) | −2.2 (20.9) |
| DEQ “Feel” | 13.9 (20.1) |
56.6
**
(28.3) |
74.0
**
(27.9) |
42.8 (30.8) |
60.1 (37.4) |
| ARCI M Scale | 0.9 (1.6) |
5.0
**
(2.8) |
6.3
**
(2.4) |
4.2 (2.9) |
5.5 (2.7) |
| POMS Anxiety | 0.1 (2.5) |
2.1 (5.3) |
6.8
*
(9.3) |
1.9 (5.7) |
6.7 (9.6) |
Note. HR = heart rate, HF-HRV = high frequency heart rate variability, DEQ = Drug Effects Questionnaire (score range: 0 – 100), ARCI = Addiction Research Center Inventory (M scale score range: 0 – 12; α = 0.85), POMS = Profile of Mood States (Anxiety scale score range: 0 – 36, α = 0.85), PCS = Peak Change Score, SD = standard deviation
p < 0.05
p < 0.005 significant relative to Placebo
3.3. Subjective Drug Effects
At both doses, THC increased DEQ ratings of “Feel” across session time compared to placebo (BTime*7.5 mg = 6.67, SE = 0.82, p < 0.0001, 95% CI [4.91, 8.23]; BTime*15 mg = 8.36, SE = 0.89, p < 0.0001, 95% CI [6.58, 10.13]; Figure 2A) compared to placebo. BMI, average daily cigarettes in the last month, and menstrual cycle phase were all significant covariates within this model (BBMI = −0.12, SE = 0.05, p = 0.024, 95% CI [−0.23, −0.02]; BRecentCigs = 0.10, SE = 0.04, p = 0.01; BPhase = 0.67, SE = 0.26, p = 0.01, 95% CI [0.14, 1.19]). Follow up t-tests indicate that both the 7.5 and 15 mg THC doses increased “feel” ratings from 90-180 minutes post-capsule. The 12 items of the ARCI M scale had a Cronbach’s alpha of 0.85, indicating a high level of internal consistency. At both doses, THC increased ARCI: M Scale scores across session time (BTime*7.5 mg = 0.66, SE = 0.08, p < 0.0001, 95% CI [0.51, 0.82]; BTime*15 mg = 0.84, SE = 0.09, p < 0.0001, 95% CI [0.67, 1.02]; Figure 2B). Age and lifetime cannabis use were both significant covariates within this model (BAge = 0.04, SE = 0.02, p = 0.005, 95% CI [0.01, 0.08]; BLifetimeCanna = −0.001, SE = 0.0002, p = 0.004, 95% CI [−0.001, −0.0002]). Follow up t-tests indicate that both the 7.5 and 15 mg THC doses increased M scale scores from 90-180 minutes post-capsule. The 9 items of the POMS Anxiety scale had a Cronbach’s alpha of 0.85, indicating a high level of internal consistency. At the 15 mg THC condition only, POMS Anxiety scale score significantly increased across session time compared to placebo (BTime*15 mg = 0.69, SE = 0.17, p < 0.0001, 95% CI [0.56, 1.01]; Figure 2C). Average daily caffeine within the past month was a significant covariate within this model (BRecentCaff = 0.68, SE = 0.19, p = 0.001, 95% CI [0.03, 1.06]). Follow up t-tests indicate that the 15 mg dose increased anxiety from 90-180 minutes post-capsule. The summary PCDS measures for the two doses are presented in Table 2.
Figure 2.

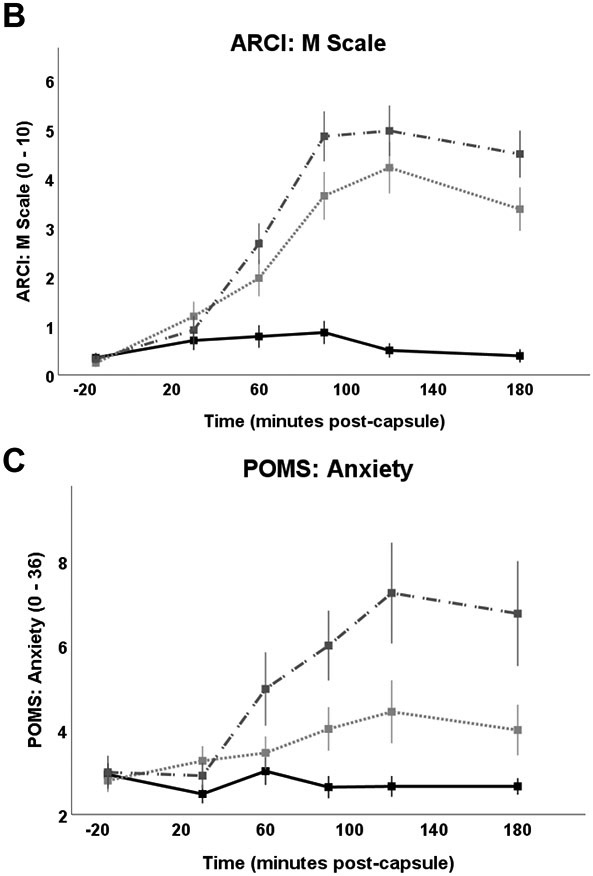
THC dose-dependently increased ratings of DEQ: “Feel” (A), ARCI: M Scale (B) and POMS: Anxiety Scale ratings (C), reported as means with standard error of the mean (SEM).
3.4. Relationships between Autonomic Response and Subjective Effects
As expected, HR was a significant predictor of HF-HRV at both the 7.5 and 15 mg THC doses (B7.5 mg = −0.05, SE = 0.03, p < 0.0001, 95% CI [−0.08, −0.03]; B15 mg = −0.08, SE = 0.01, p < 0.0001, 95% CI [−0.10, −0.05]). At the 15 mg dose only, both HR (B15 mg = −0.78, SE = 0.15, p < 0.0001, 95% CI [−1.90, −0.47]) and HF-HRV (B15 mg = 5.39, SE = 1.42, p = 0.001, 95% CI [2.46, 8.32]) were significant predictors of PEP. HR and PEP were not significantly related to any of the subjective measures at either dose. HF-HRV (B15 mg = −0.51, SE = 0.21, p = 0.02, 95% CI [−0.93, −0.078] significantly predicted ARCI: M scale scores at the 15 mg dose only (Figure 3).
Figure 3.

Regression of autonomic and subjective measures peak change difference scores (PCDS) between the 15 mg THC condition and placebo (PLC) condition. HF-HRV was a significant predictor of ARCI: Mar Scale scores at the 15 mg THC dose only.
4. Discussion
The present analysis had two main goals: to examine the acute effects of oral THC on autonomic nervous system cardiac activity in healthy naturally cycling women, and to determine whether these physiological effects were associated with subjective measures of drug response, especially anxiety. THC dose-dependently increased HR and decreased HF-HRV, indicating an effect on parasympathetic cardiac activity. It did not affect BP or PEP, the measure of sympathetic cardiac activity. THC produced its typical subjective effects, including dose-dependently increasing ratings of feeling a drug effect, cannabis-like intoxication effects, and it produced modest increases in state anxiety. As expected, HR was a significant predictor of both PEP and HF-HRV across session time. Although PEP was not a significant predictor of any subjective measures, HF-HRV significantly predicted ratings on the ARCI M scale (ARCI) at the 15 mg dose. HF-HRV and PEP were not related to anxiety at either dose and autonomic measures were not related to any subjective effects at the 7.5 mg dose. These findings suggest that parasympathetic autonomic responses to higher doses of THC are related to cannabis-specific subjective intoxication effects, but not anxiety.
The dose dependent effect of THC on HR, and lack of effect on BP, in our study is consistent with past reports of cannabinoids increasing HR without significantly affecting BP (Ghasemiesfe et al., 2019; Hunault et al., 2008; Wachtel et al., 2002; Ashton et al., 2001; Lex et al., 1984; Kanakis et al., 1976; Beaconsfield et al., 1972). Our findings are also consistent with reports that the degree of tachycardia is related to the dosage of THC in both smoked cannabis (Hunault et al., 2008; Johnson & Domino, 1971) and after oral THC (Pabon & de Wit, 2019; Wachtel et al., 2002; Kirk & de Wit, 1999).
Our findings of THC-induced changes in parasympathetic cardiac activity are consistent with and extend previous findings. Zuurman et al. (2008) assessed low and high frequency HRV in healthy men with a history of mild cannabis use after cumulative doses of inhaled THC (2, 4, 6 and 8 mg at 90-min intervals). The two higher doses increased low frequency heart rate variability and decreased HF-HRV 37 minutes after consumption. The authors argued their findings indicated a THC-induced peripheral reduction in vagal tone. Instead of cumulative doses of inhaled THC, our study administered oral THC to a larger sample of women in separate dose conditions. We also found THC dose dependently decreased HF-HRV and we were able to capture these effects over a longer time course. In addition, Zuurman et al. reported the increase in low frequency heart rate variability indicated a THC-induced increase in sympathetic activity. Our study did not replicate this result using a more sensitive measure of sympathetic activity, PEP. The lack of a drug effect on PEP in our study contrasts results from two older studies (Weiss et al., 1972; Kanakis et al., 1976). Weiss et al. found orally administrated THC (0.3 mg per kilogram) shortened PEP in eight male volunteers. Kanakis et al. found intravenous THC (25 μg/kg) shortened PEP in ten male volunteers. The discrepancy between these findings and the present ones may be due to sample differences, including size and gender. Taken together, the present study adds to prior literature by replicating THC-induced decreases in parasympathetic activity, extending findings to a larger sample and to women, and reporting no significant effect of oral THC on PEP, a measure of sympathetic cardiac activity, in women.
In the present study, effects of THC on subjective measures were only moderately related to autonomic measures. Although neither HR nor PEP PCDS were related to subjective measures, HF-HRV PCDS was a significant predictor of ARCI: M scale scores at the 15 mg dose. Previous findings on this topic are variable. In one study, the effects of cannabis (cigarette 1.8% THC) in female smokers on HR were significantly correlated with increased subjective levels of intoxication and confusion scores, but not with anxiety (Lex et al., 1984). Similar results were reported in earlier studies of male cannabis smokers (Babor et al., 1975; Mendelson et al., 1976). However, other studies have failed to detect significant linear relationships between physiological response and subjective drug experience (Galanter et al., 1972; Ohlsson et al., 1980; Hollister et al., 1981; Guy & Robson, 2004a, 2004b). These mixed findings may be due to pharmacokinetic factors affecting individuals’ differences in drug absorption, resulting in variable plasma concentrations of THC. The lack of association between PEP and subjective drug experience in our study may be due to the relatively high variability and lack of consistent drug effect on PEP. Known sources of variability in physiological and subjective responses to THC include sex, body mass index (BMI), age and prior cannabis use (D’Souza et al., 2004; Pope & Yurgelun-Todd, 1996; Wiley & Burston, 2014). Even after accounting for these within our analyses we still did not observe an effect of oral THC on PEP across time. The high variability and lack of drug effect on PEP explains why we detected an association between subjective drug experience and HF-HRV, but not PEP. This suggests subjective drug experience may be more closely related to parasympathetic cardiac activity than sympathetic cardiac activity. Contrary to some previous reports, we did not find significant associations between either autonomic measure or subjective anxiety. Shortened PEP and low HF-HRV have been associated with difficulties regulating anxiety (Gorka et al., 2013; Thayer et al., 1996), and either increased sympathetic activity or reductions in parasympathetic activity may be associated with anxiety. At the doses of THC used here, it appears that HF-HRV is more closely associated with cannabis-specific measures of subjective intoxication, rather than anxiety. However, the doses used here are modest compared to the concentrations attained in high potency cannabis (Chandra et al., 2019), leaving open the possibility that the sympathetic system would be more involved at higher doses.
There is preclinical evidence of ovarian hormones, especially estradiol, modulating responses to cannabinoids in animals. However, the present analysis found little evidence for this in naturally cycling women. In rats, estrogen increases cannabinoid receptor binding site density in the amygdala (Riebe et al., 2010). We found in the present sample that effects of oral THC were not significantly different between the early and late follicular phase, when estradiol levels are low (early) or elevated (late). Neither the autonomic effects nor the anxiogenic effects differed between the two phases, although there was some indication that cycle phase may potentially modulate ratings of “feeling” a drug effect on the DEQ. With a larger sample of participants we will continue to investigate the influence of menstrual cycle phase on responses to oral THC.
The present study had limitations. First, the sample was not powered to detect smaller associations between autonomic function and subjective experience. Additionally, since our study was conducted in a controlled laboratory setting, both the physiological drug effects and subjective drug experience in the laboratory may not be reflective of that in a natural setting. Future studies should investigate the effect of social context on the autonomic and subjective effects of oral THC or smoked cannabis. Another important variable is dose: THC levels in cannabis have increased markedly in recent years, and it is likely users are exposed to higher concentrations of the drug than those attained in the present study. Finally, this study focused on women only during the follicular phase of their menstrual cycle, and it will be important to determine if similar effects are detected in women during the luteal phase, in women taking exogenous hormones, or in men.
The present study provided a novel profile of the autonomic effects of two oral doses of THC in women, and provided insight on how physiological drug response is related to subjective drug response. THC dose-dependently increased HR, sympathetic cardiac activity, and ratings of subjective intoxication, and it decreased parasympathetic cardiac activity. Further, at the higher dose of THC, HF-HRV was significantly associated with ratings of subjective cannabis intoxication. Thus, individuals who experience greater intoxicating effects of THC exhibit greater decreases in parasympathetic cardiac activity. Surprisingly, anxiety was not related to drug-induced autonomic activity. Future studies investigating related effects at higher doses, with other cannabinoids and combinations of cannabinoids as found in the plant, in heterogeneous populations including men, drug users or individuals with psychiatric symptoms will extend the findings. Further, studies of individual differences in response to acute THC will build the foundation for safer cannabis or THC use guidelines. Ultimately, this kind of research will aid in decreasing the public health risk associated with adverse responses to cannabis or THC.
Funding Sources
This research was funded by the National Institute on Drug Abuse R01DA002812 (PI: HdW). EP was supported by 5T32DA0043469 and F31DA049391 (PI: EP).
Footnotes
Conflict of Interest Statement
The authors declare that there are no conflicts of interest.
References
- American Psychiatric Association (APA). (2013). Substance-related and addictive disorders. In Diagnostic and statistical manual of mental disorders (5th ed.). 10.1176/appi.books.9780890425596.dsm16 [DOI] [Google Scholar]
- Ashton C (2001). Pharmacology and effects of cannabis: A brief review. British Journal of Psychiatry, 178(2), 101–106. 10.1192/bjp.178.2.101 [DOI] [PubMed] [Google Scholar]
- Babor TF, Mendelson JH, Greenberg I, & Kuehnle JC (1975). Marijuana consumption and tolerance to physiological and subjective effects. Archives of general psychiatry, 32(12), 1548–1552. 10.1001/archpsyc.1975.01760300086007 [DOI] [PubMed] [Google Scholar]
- Beaconsfield P, Ginsburg J, Rainsbury R (1972). Marihuana Smoking – Cardiovascular Effects in Man and Possible Mechanisms. N Engl J Med, 287, 209–212. 10.1056/NEJM197208032870501 [DOI] [PubMed] [Google Scholar]
- Beauchaine TP, Thayer JF. Heart rate variability as a transdiagnostic biomarker of psychopathology. (2015) Int J Psychophysiol. 98 (2 Pt 2):338–350. 10.1016/j.ijpsycho.2015.08.004 [DOI] [PubMed] [Google Scholar]
- Berntson GG, Bigger JT JR., Eckberg D, Grossman P, Kaufmann PG, Malik M Nagaraja HN, Porges SW, Saul JP, Stone PH, Van Der Molen MW (1997). Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology, 34(6), 623–648. 10.1111/j.1469-8986.1997.tb02140.x [DOI] [PubMed] [Google Scholar]
- Berntson GG, Lozano DL, Chen YJ, & Cacioppo JT (2004). Where to Q in PEP. Psychophysiology, 41(2), 333–337. 10.1111/j.1469-8986.2004.00156.x [DOI] [PubMed] [Google Scholar]
- Berntson GG, Norman GJ, Hawkley LC, & Cacioppo JT (2008). Cardiac autonomic balance versus cardiac regulatory capacity. Psychophysiology, 45(4), 643–652. 10.1111/j.1469-8986.2008.00652.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berntson GG, Quigley KS, & Lozano D (2007). Cardiovascular psychophysiology. In Cacioppo JT, Tassinary LG, & Berntson GG (Eds.), Handbook of psychophysiology (pp. 182–210). Cambridge, NY: Cambridge University Press. 10.1017/CBO9780511546396 [DOI] [Google Scholar]
- Bloom AS, Kiernan CJ (1980). Interaction of ambient temperature with the effects of Δ 9 on brain catecholamine synthesis and plasma corticosterone levels. Psychopharmacology 67, 215–219. 10.1007/BF00431259 [DOI] [PubMed] [Google Scholar]
- Cacioppo JT, Berntson GG, Binkley PF, Quigley KS, Uchino BN, & Fieldstone A (1994). Autonomic cardiac control. II. Noninvasive indices and basal response as revealed by autonomic blockades. Psychophysiology, 31(6), 586–598. 10.1111/j.1469-8986.1994.tb02351.x [DOI] [PubMed] [Google Scholar]
- Cacioppo JT, Hawkley LC, Crawford LE, Ernst JM, Burleson MH, Kowalewski RB, Malarkey WB, Van Cauter E, & Berntson GG (2002). Loneliness and health: potential mechanisms. Psychosomatic medicine, 64(3), 407–417. 10.1097/00006842-200205000-00005 [DOI] [PubMed] [Google Scholar]
- Cacioppo JT, & McGuigan FJ (1980). Cognitive Psychophysiology: Principles of Covert Behavior. The American Journal of Psychology, 93(1), 173. 10.2307/1422117 [DOI] [Google Scholar]
- Chait LD, Fischman MW, Schuster CR (1985). ‘Hangover’ effects the morning after marijuana smoking. Drug and Alcohol Dependence 15, 229–238. 10.1016/0376-8716(85)90002-X [DOI] [PubMed] [Google Scholar]
- Chalmers JA, Heathers JAJ, Abbott MJ, Kemp AH, & Quintana DS (2016). Worry is associated with robust reductions in heart rate variability: A transdiagnostic study of anxiety psychopathology. BMC Psychology, 4(1). 10.1186/s40359-016-0138-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chalmers JA, Quintana DS, Abbott MJ, & Kemp AH (2014). Anxiety Disorders are Associated with Reduced Heart Rate Variability: A Meta-Analysis. Frontiers in psychiatry, 5, 80. 10.3389/fpsyt.2014.00080 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chandra S, Radwan MM, Majumdar CG, Church JC, Freeman TP, & ElSohly MA (2019). New trends in cannabis potency in USA and Europe during the last decade (2008-2017). European archives of psychiatry and clinical neuroscience, 269(1), 5–15. 10.1007/s00406-019-00983-5 [DOI] [PubMed] [Google Scholar]
- Clark SC, Greene C, Karr GW, MacCannell KL, & Milstein SL (1974). Cardiovascular effects of marihuana in man. Canadian journal of physiology and pharmacology, 52(3), 706–719. 10.1139/y74-090 [DOI] [PubMed] [Google Scholar]
- Craft RM, & Leitl MD (2008). Gonadal hormone modulation of the behavioral effects of Delta9-tetrahydrocannabinol in male and female rats. European journal of pharmacology, 578(1), 37–42. 10.1016/j.ejphar.2007.09.004 [DOI] [PubMed] [Google Scholar]
- Crean RD, Crane NA, & Mason BJ (2011). An Evidence Based Review of Acute and Long-Term Effects of Cannabis Use on Executive Cognitive Functions. Journal of Addiction Medicine, 5(1), 1–8. 10.1097/ADM.0b013e31820c23fa [DOI] [PMC free article] [PubMed] [Google Scholar]
- D'Souza DC, Perry E, MacDougall L, Ammerman Y, Cooper T, Wu YT, Braley G, Gueorguieva R, & Krystal JH (2004). The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: implications for psychosis. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology, 29(8), 1558–1572. 10.1038/sj.npp.1300496 [DOI] [PubMed] [Google Scholar]
- Fattore L, & Fratta W (2010). How important are sex differences in cannabinoid action?. British journal of pharmacology, 160(3), 544–548. 10.1111/j.1476-5381.2010.00776.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fattore L, Spano MS, Altea S, Angius F, Fadda P, & Fratta W (2007). Cannabinoid self-administration in rats: sex differences and the influence of ovarian function. British journal of pharmacology, 152(5), 795–804. 10.1038/sj.bjp.0707465 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freeman D, Dunn G, Murray RM, Evans N, Lister R, Antley A, Slater M, Godlewska B, Cornish R, Williams J, Di Simplicio M, Igoumenou A, Brenneisen R, Tunbridge EM, Harrison PJ, Harmer CJ, Cowen P, Morrison PD. How cannabis causes paranoia: using the intravenous administration of Δ9-tetrahydrocannabinol (THC) to identify key cognitive mechanisms leading to paranoia (2015). Schizophr Bull., 41(2), 391–9. 10.1093/schbul/sbu098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedman BH (2007). An autonomic flexibility—neurovisceral integration model of anxiety and cardiac vagal tone. Biological Psychology. 74(2) 185–199. 10.1016/j.biopsycho.2005.08.009 [DOI] [PubMed] [Google Scholar]
- Galanter M, Wyatt RJ, Lemberger L, Weingartner H, Vaughan TB, Roth WT (1972). Science, 176(4037), 934–936. 10.1126/science.176.4037.934 [DOI] [PubMed] [Google Scholar]
- Garfinkle EJ (2017). The associations between marijuana use, emotion dysregulation, and heart rate variability among healthy young adults. RUcore: Rutgers University Community Repository. https://doi.org/doi: 10.7282/T3T43X5G [DOI] [Google Scholar]
- Ghasemiesfe M, Ravi D, Casino T et al. Acute Cardiovascular Effects of Marijuana Use. J GEN INTERN MED 35, 969–974 (2020). 10.1007/s11606-019-05235-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson DG (1978). Use of the systolic time intervals in clinical pharmacology. British journal of clinical pharmacology, 6(2), 97–102. 10.1111/j.1365-2125.1978.tb00832.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gorka SM, McGowan SK, Campbell ML, Nelson BD, Sarapas C, Bishop JR, Shankman SA (2013). Association between respiratory sinus arrhythmia and reductions in startle responding in three independent samples. Biological Psychology, 93(2), 334–341. 10.1016/j.biopsycho.2013.03.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenfield SF, Back SE, Lawson K, & Brady KT (2010). Substance Abuse in Women. The Psychiatric Clinics of North America, 33(2), 339–355. 10.1016/j.psc.2010.01.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guy GW, Robson PJ (2004a). A phase I, double blind, three-way crossover study to assess the pharmacokinetic profile of Cannabis Based Medicine Extract (CBME) administered sublingually in variant cannabinoid ratios in normal healthy male volunteers. J. Cannabis Ther 3, 121–152. 10.1300/J175v03n04_02 [DOI] [Google Scholar]
- Guy GW, Robson PJ (2004b). A phase I, open label, four-way crossover study to compare the pharmacokinetic profiles of a single dose of 20 mg of a Cannabis Based Medicine Extract (CBME) Administered on 3 different areas of the buccal mucosa and to investigate the pharmacokinetics of CBME per Oral in Healthy Male and Female Volunteers (GWPK0112). J. Cannabis Ther 3, 79–120. 10.1300/J175v03n04_01 [DOI] [Google Scholar]
- Hampson E (2020). A brief guide to the menstrual cycle and oral contraceptive use for researchers in behavioral endocrinology. Hormones and behavior, 119, 104655. 10.1016/j.yhbeh.2019.104655 [DOI] [PubMed] [Google Scholar]
- Hindley G, Beck K, Borgan F, Ginestet CE, McCutcheon R, Kleinloog D, Ganesh S, Radhakrishnan R, D’Souza DC, Howes OD. (2020). Psychiatric symptoms caused by cannabis constituents: a systematic review and meta-analysis. Lancet Psychiatry, 7(4), 344–353. 10.1016/S2215-0366(20)30074-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofmann SG, Moscovitch DA, Litz BT, Kim HJ, Davis L, Pizzagalli DA (2005). The worried mind: autonomic and prefrontal activation during worrying. Emotion 5, 464–475. 10.1037/1528-3542.5.4.464 [DOI] [PubMed] [Google Scholar]
- Hofmann SG, Schulz SM, Heering S, Muench F, & Bufka LF (2010). Psychophysiological correlates of generalized anxiety disorder with or without comorbid depression. International journal of psychophysiology: official journal of the International Organization of Psychophysiology, 78(1), 35–41. 10.1016/j.ijpsycho.2009.12.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hollister LE (1986). Health aspects of cannabis. Pharmacological Reviews, 38(1), 1–20. PMID: 3520605 10.1016/0378-8741(87)90030-4 [DOI] [PubMed] [Google Scholar]
- Hollister LE, Gillespie HK, Ohlsson A, Lindgren J-E, Wahlen A, Agurell S (1981). Do plasma concentrations of delta-9-tetrahydrocannabinol reflect the degree of intoxication? The Journal of Clinical Pharmacology, 21(1), 171–177. 10.1002/j.1552-4604.1981.tb02593.x [DOI] [PubMed] [Google Scholar]
- Hunault CC, Mesinga TT, de Vries I. et al. (2008). Delta-9-tetrahydrocannabinol (THC) serum concentrations and pharmacological effects in males after smoking a combination of tobacco and cannabis containing up to 69 mg THC. Psychopharmacology 201, 171–181, 10.1007/s00213-008-1260-2 [DOI] [PubMed] [Google Scholar]
- Johnson S, & Domino EF (1971). Some cardiovascular effects of marihuana smoking in normal volunteers. Clinical pharmacology and therapeutics, 12(5), 762–768. 10.1002/cpt1971125762 [DOI] [PubMed] [Google Scholar]
- Jones RT (2002), Cardiovascular System Effects of Marijuana. The Journal of Clinical Pharmacology, 42: 58S–63S. 10.1002/j.1552-4604.2002.tb06004.x [DOI] [PubMed] [Google Scholar]
- Kanakis C Jr., Pouget JM, Rosen KM (1976). The effects of delta-9-tetrahydrocannabinol (cannabis) on cardiac performance with and without beta blockade. Circulation, 53, 703–707. 10.1161/01.CIR.53.4.703 [DOI] [PubMed] [Google Scholar]
- Kao LC, Liu YW, Tzeng NS, Kuo TB, Huang SY, Chang CC, & Chang HA (2016). Linking an Anxiety-Related Personality Trait to Cardiac Autonomic Regulation in Well-Defined Healthy Adults: Harm Avoidance and Resting Heart Rate Variability. Psychiatry investigation, 13(4), 397–405. 10.4306/pi.2016.13.4.397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karila L, Roux P, Rolland B, Benyamina A, Reynaud M, Aubin HJ, & Lançon C (2014). Acute and long-term effects of cannabis use: a review. Current pharmaceutical design, 20(25), 4112–4118. 10.2174/13816128113199990620 [DOI] [PubMed] [Google Scholar]
- Karschner EL, Darwin WD, McMahon RP, Wright S, Goodwin RS, Huestis MA (2011). Subjective and physiological effects after controlled sativex and oral THC administration. Clinical Pharmacology & Therapeutics 89(3), 400–407. 10.1038/clpt.2010.318 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kemp AH, Quintana DS, Felmingham KL, Matthews S, Jelinek HF (2012). Depression, Comorbid Anxiety Disorders, and Heart Rate Variability in Physically Healthy, Unmedicated Patients: Implications of Cardiovascular Risk. Plos One, 7(2): e30777. 10.1371/journal.pone.0030777 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim ESH, & Menon V (2009). Status of Women in Cardiovascular Clinical Trials. Arteriosclerosis, Thrombosis, and Vascular Biology, 29(3), 279–283. 10.1161/ATVBAHA.108.179796 [DOI] [PubMed] [Google Scholar]
- Kirk JM, de Wit H (1999). Responses to oral delta-9-tetrahydrocannabinol in frequent and infrequent marijuana users. Pharmacology Biochemistry and Behavior, 63(1) 137–142. 10.1016/S0091-3057(98)00264-0 [DOI] [PubMed] [Google Scholar]
- Kirkpatrick MG, de Wit H (2013). In the company of others: social factors alter acute alcohol effects. Psychopharmacology 230, 215–226. 10.1007/s00213-013-3147-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koschke M, Boettger MK, Schulz S, Berger S, Terhaar J, Voss A, Yeragani VK, & Bär KJ (2009). Autonomy of autonomic dysfunction in major depression. Psychosomatic medicine, 71(8), 852–860. 10.1097/PSY.0b013e3181b8bb7a [DOI] [PubMed] [Google Scholar]
- Lex BW, Mendelson JH, Bavli S et al. (1984). Effects of acute marijuana smoking on pulse rate and mood states in women. Psychopharmacology 84, 178–187 10.1007/BF00427443 [DOI] [PubMed] [Google Scholar]
- Light KC, Kothandapani RV, & Allen MT (1998). Enhanced cardiovascular and catecholamine responses in women with depressive symptoms. International journal of psychophysiology: official journal of the International Organization of Psychophysiology, 28(2), 157–166. 10.1016/s0167-8760(97)00093-7 [DOI] [PubMed] [Google Scholar]
- Lozano DL, Norman G, Knox D, Wood BL, Miller BD, Emery CF, & Berntson GG (2007). Where to B in dZ/dt. Psychophysiology, 44(1), 113–119. 10.1111/j.1469-8986.2006.00468.x [DOI] [PubMed] [Google Scholar]
- Martin WR, Sloan JW, Sapira JD, Jasinski DR, 1971. Physiologic, subjective, and behavioral effects of amphetamine, methamphetamine, ephedrine, phenmetrazine, and methylphenidate in man. Clin. Pharmacol. Ther 12, 245–258. 10.1002/cpt1971122part1245 [DOI] [PubMed] [Google Scholar]
- Martin-Santos R, Crippa JA, Batalla A, Bhattacharyya S, Atakan Z, Borgwardt S, Allen P, Seal M, Langohr K, Farré M, Zuardi AW, & McGuire PK (2012). Acute effects of a single, oral dose of d9-tetrahydrocannabinol (THC) and cannabidiol (CBD) administration in healthy volunteers. Current Pharmaceutical Design, 18(32), 4966–4979. 10.2174/138161212802884780 [DOI] [PubMed] [Google Scholar]
- Martz R, Brown DJ, Forney RB, Bright TP Kiplinger GR, Rodda BE (1972). Propranolol antagonism of marihuana induced tachycardia. Life Sciences, 11(21), 999–1005. 10.1016/0024-3205(72)90179-8 [DOI] [Google Scholar]
- McNair D, Lorr M, Droppleman L (1971). Profile of mood states. Educational and Industrial Testing Service, San Diego, California. [Google Scholar]
- Mendelson JH, Babor TF, Kuehnle JC, Rossi AM, Bernstein JG, Mello NK, Greenberg I (1976). Behavioral and biologic aspects of marijuana use. Annals of NY Acad Sci, 282, 186–210. 10.1111/j.1749-6632.1976.tb49899.x [DOI] [PubMed] [Google Scholar]
- Morean ME, de Wit H, King AC, Sofuoglu M, Rueger SY, & O'Malley SS (2013). The drug effects questionnaire: psychometric support across three drug types. Psychopharmacology, 227(1), 177–192. 10.1007/s00213-012-2954-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmalenberger KM, Tauseef HA, Barone JC, Owens SA, Lieberman L, Jarczok MN, Girdler SS, Kiesner J, Ditzen B, & Eisenlohr-Moul TA (2021). How to study the menstrual cycle: Practical tools and recommendations. Psychoneuroendocrinology, 123, 104895. 10.1016/j.psyneuen.2020.104895 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA). (2019). 2019 National Survey on Drug Use and Health: Methodological summary and definitions. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/data/ [Google Scholar]
- Ohlsson A, Lindgren J-E, Wahlen A, Agurell S, Hollister LE, Gillespie HK (1980). Plasma delta-9-tetrahydrocannabiol concentrations and clinical effects after oral and intravenous administration and smoking. Clinical Pharmacology & Therapeutics, 28, 409–416. 10.1038/clpt.1980.181 [DOI] [PubMed] [Google Scholar]
- Ogborne AC, Smart RG, Weber T, Birchmore-Timney C (2000) Who is Using Cannabis as a Medicine and Why: An Exploratory Study. Journal of Psychoactive Drugs, 32:4, 435–443, 10.1080/02791072.2000.10400245 [DOI] [PubMed] [Google Scholar]
- Pabon E, de Wit H (2019). Developing a phone-based measure of impairment after acute oral delta-9-tetrahydrocannabinol. Journal of Psychopharmacology, 33(9), 1160–1169. 10.1177/0269881119862533 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patel S, Roelke CT, Rademacher DJ, Cullinan WE, Hillard CJ (2004) Endocannabinoid Signaling Negatively Modulates Stress-Induced Activation of the Hypothalamic-Pituitary-Adrenal Axis, Endocrinology, 145(12) 5431–5438, 10.1210/en.2004-0638 [DOI] [PubMed] [Google Scholar]
- Pope HG Jr, & Yurgelun-Todd D (1996). The residual cognitive effects of heavy marijuana use in college students. JAMA, 275(7), 521–527. 10.1001/jama.1996.03530310027028 [DOI] [PubMed] [Google Scholar]
- Riebe CJ, Hill MN, Lee TT, Hillard CJ, & Gorzalka BB (2010). Estrogenic regulation of limbic cannabinoid receptor binding. Psychoneuroendocrinology, 35(8), 1265–1269. 10.1016/j.psyneuen.2010.02.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Renault PF, Schuster CR, Heinrich R, Freeman D (1971). Science, 174(4009), 589–591. 10.1126/science.174.4009.589 [DOI] [PubMed] [Google Scholar]
- Sherwood A, Allen MT, Fahrenberg J, Kelsey RM, Lovallo WR, van Doornen LJP (1990). Methodological Guidelines for Impedance Cardiography. Psychophysiology, 27(1). 10.1111/j.1469-8986.1990.tb02171.x [DOI] [PubMed] [Google Scholar]
- Sholler DJ, Strickland JC, Spindle TR, Weerts EM, & Vandrey R (2020). Sex differences in the acute effects of oral and vaporized cannabis among healthy adults. Addiction biology, e12968. Advance online publication. 10.1111/adb.12968 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thayer JF, Friedman BH, & Borkovec TD (1996). Autonomic characteristics of generalized anxiety disorder and worry. Biological psychiatry, 39(4), 255–266. 10.1016/0006-3223(95)00136-0 [DOI] [PubMed] [Google Scholar]
- Thomas H (1996). A community survey of adverse effects of cannabis use. Drug and Alcohol Dependence, 42(3), 201–207, 10.1016/S0376-8716(96)01277-X [DOI] [PubMed] [Google Scholar]
- Vollman RF (1977). The menstrual cycle. Major problems in obstetrics and gynecology, 7, 1–193. [PubMed] [Google Scholar]
- Wachtel S, ElSohly M, Ross S et al. (2002). Comparison of the subjective effects of Δ9-tetrahydrocannabinol and marijuana in humans. Psychopharmacology 161, 331–339 10.1007/s00213-002-1033-2 [DOI] [PubMed] [Google Scholar]
- Wakley AA, & Craft RM (2011). Antinociception and sedation following intracerebroventricular administration of Δ9-tetrahydrocannabinol in female vs. male rats. Behavioural brain research, 216(1), 200–206. 10.1016/j.bbr.2010.07.037 [DOI] [PubMed] [Google Scholar]
- Weiss JL, Watanabe AM, Lemberger L, Tamarkin NR, & Cardon PV (1972). Cardiovascular effects of delta-9-tetrahydrocannabinol in man. Clinical pharmacology and therapeutics, 13(5), 671–684. 10.1002/cpt1972135part1671 [DOI] [PubMed] [Google Scholar]
- Wiley JL, & Burston JJ (2014). Sex differences in Δ(9)-tetrahydrocannabinol metabolism and in vivo pharmacology following acute and repeated dosing in adolescent rats. Neuroscience letters, 576, 51–55. 10.1016/j.neulet.2014.05.057 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williamson EM, & Evans FJ (2000). Cannabinoids in clinical practice. Drugs, 60(6), 1303–1314. 10.2165/00003495-200060060-00005 [DOI] [PubMed] [Google Scholar]
- Zeiger JS, Haberstick BC, Corley RP, Ehringer MA, Crowley TJ, Hewitt JK, Hopfer CJ, Stallings MC, Young SE, & Rhee SH (2010). Subjective effects to marijuana associated with marijuana use in community and clinical subjects. Drug and Alcohol Dependence, 109(1), 161–166. 10.1016/j.drugalcdep.2009.12.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zuurman L, deKam ML, Cohen AF, van Gerven JMA, Burggraaf J (2008). Evaluation of THC-induced tachycardia in humans using heart rate variability. In Clinical Pharmacology of Cannabinoids in Early Phase Drug Development, Doctoral Thesis. Pg 87–96 [Google Scholar]