

Abstract
Background:
Over the last 20 years, internet-delivered cognitive behavior therapy (ICBT) has been tested in a large number of randomized controlled trials, often with positive results. However, it is not widely known about the efficacy of ICBT as compared to face-to-face cognitive behavior therapy (CBT).
Methods:
In the present systematic review and meta-analysis, ICBT for treatment of anxiety disorders was directly compared to face- to-face CBT within the same trial. This study aimed to reinvestigate the effect of ICBT compared to face-to-face CBT for anxiety disorders. A total of 8 studies out of the 236 articles screened met all the inclusion criteria. The included studies targeting five different anxiety disorders, social anxiety disorder, adolescent anxiety, panic disorder, spider phobia, and fear of public speaking, had been carried out in Australia, Spain, and Sweden. The total number of participants was 348 in ICBT and 316 in face-to-face conditions.
Results:
The results of our meta-analysis are interesting both from theoretical and practical standpoints, which showed a pooled effect size posttreatment with Hedges' g = 0.01 (95% CI: −0.16 to 0.18),
Conclusions:
ICBT and face-to-face CBT created equivalent overall effects. in treatment of anxiety disorders. Since there have been similar systematic reviews about anxiety disorders so far, and in majority of them, ICBT has not been compared against face-to-face treatment. More research is needed to establish the general equivalence of the two treatment formats. Also, understanding what makes ICBT work is a challenge for future research.
Keywords: Anxiety Disorders, cognitive behavior therapy, internet, meta-analysis
Introduction
Internet-based cognitive-behavior therapy (ICBT) is almost the same as conventional cognitive-behavior therapy (CBT), but delivered through the internet in which a client completes some materials and modules through a website.[1] The patient is also guided by an online therapist who provides support through clarifying information, monitoring the progress, giving feedback to homework, and allowing the patient access to the sequential treatment steps.[1] ICBT has many advantages compared to classic treatment: it requires less therapist time (in adults, about 85% less therapist time per week) and it is not limited to the office hours; it can also be performed without the limitation of distances between therapist and patient, which can decrease the possible risk of stigma in visiting a therapist; and children and their parents can be involved in the therapy program without missing school or work.[2]
Several forms of ICBT are designed by researchers from all around the world. Most have a therapist, guiding the patient during treatment. Treatments are structured, usually including up to 15 training modules, which are roughly equivalent to the number of face-to-face CBT sessions.[3] These treatments are different from many aspects such as technical solutions, the amount of therapist's support, and diagnostic processes.[4] They also have some features in common; for example, all are based on cognitive behavior approach including the components of face-to-face CBT such as exposure, psychoeducation, and treatment during 8-15 weeks. Most of these programs use text messages as the main form of communication between the patient and the therapist. They have an integrated assessment system and assignment in the internet-based therapy program.[3]
Since the early treatment researches on ICBT that were done in the late 1990s,[5] more than 200 randomized controlled trials have been conducted, often with hopeful outcomes showing that ICBT is clinically effective when compared to controls without any disorder.[6] Also, some long-term, follow-up studies have indicated that the ICBT effects are kept for 5 years posttreatment.[7] Despite obtaining promising outcomes in control trials, in which ICBT is often compared with waiting list control groups, an important question is how well-guided ICBT compares against face-to-face treatment.[8] This was studied in a meta-analysis that consisted of 13 studies (N = 1053) published till June 2013. The results indicated a pooled effect size posttreatment with Hedges' g = −0.01 (95% Cl: −0.13 to 0.12), suggesting that ICBT and face-to-face treatment result in equal overall effects for psychiatric and somatic disorders.[9] This study was updated in 2018 with 20 studies (N = 1418). The results showed the same effects of CBT and ICBT for the psychiatric and somatic disorders. This approach offers a reasonable alternative to clinic-based therapy with advantages of low cost, reduced therapist time, and greater accessibility for the families that have difficulty accessing clinic-based CBT.[10,11]
One of the most important areas that were well researched on ICBT is anxiety disorders.[12] Several studies showed that internet-based treatments have the same effects as face-to-face therapies for different types of anxiety disorders. More specifically, CBT and ICBT are equally effective in anxiety disorders in adolescents,[11] spider phobia,[13] social anxiety,[7] panic disorder,[14] and fear of public speaking.[15]
Although studies in the last decade have consistently shown that ICBT is an effective treatment for anxiety disorders[7] with the same outcomes in comparison to face-to-face treatment, many people never receive treatment or get it after years of pain.[2,12] Also, according to some studies, anxiety disorders, despite being extremely prevalent, have a little possibility of being treated than other psychiatric disorders.[2] On the other hand, the efficacy of ICBT in different types of disorders may vary due to their characteristics;[12] therefore, there is a crucial need to do more researches specifically focusing on the efficacy of ICBT in anxiety disorders comparing to face-to-face therapy the present review can study results show the equality of these two treatments.
As this area is moving ahead quickly and many new studies have been published, and also to the best of our knowledge, no earlier review has targeted anxiety disorders for comparing internet-based and face-to-face CBT, there is a need for a systematic review and meta-analysis focusing on this area. This study aimed to compare the efficacy of internet-based vs. face-to-face CBT for anxiety disorders including social anxiety disorder, adolescent anxiety, panic disorder, spider phobia, and fear of public speaking. Therefore, the research question is whether the impact of face-to-face vs. internet-based CBT for anxiety disorders is the same or not. We conducted a systematic review and meta-analysis of studies directly comparing the two treatment formats. According to strong research literature, we hypothesized that ICBT and face-to-face CBT would produce equivalent treatment effects.
Methods
Data sources and search strategy
To identify the studies published until 2019, systematic searches in PubMed, Scopus, ProQuest, Emerald, and Science direct were conducted, starting from 2019. The search strategy employed a combination of search terms related to anxiety disorders (anxiety, anxiety disorders, fear, panic disorder, social phobia, social anxiety, generalized anxiety disorder, posttraumatic stress disorder, specific phobia, obsessive-compulsive disorder), internet (internet, online, web, computer, computerized, internet-based, internet-delivered, internet delivery), and CBT (behavior, cognitive, therapy, treatment). The complete search strings can be viewed in Figure 1.
Figure 1.
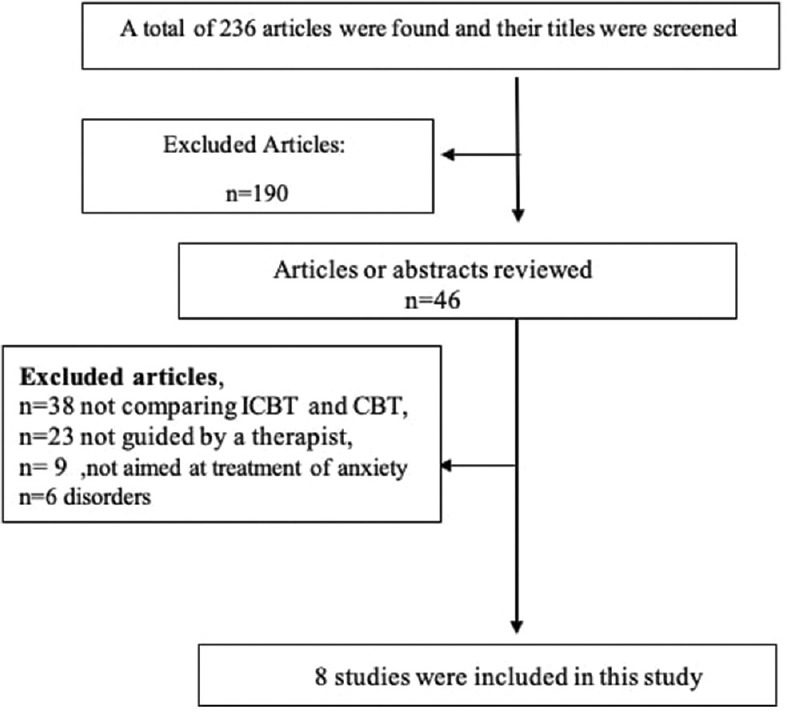
Study inclusion process throughout the review
Study selection
Articles were included if a) they compared therapist-guided ICBT to face-to-face treatment using a randomized controlled design; b) they used interventions aimed at the treatment of anxiety disorders (and not, e.g., prevention or mere psychoeducation); c) they investigated a form of ICBT where internet treatment was the main component and not a secondary complement to other therapies; d) the internet treatment group was supported by an online therapist; and e) they were written in English. There were no restrictions regarding age.
Each article was independently assessed by the first and corresponding authors at title, abstract, and full-text levels to evaluate its inclusion or exclusion according to the criteria presented above. In the cases where there was disagreement on inclusion decision, the full-text level was reviewed for reaching consensus.
Data extraction
The following variables were extracted from the studies included for further analysis: country, first author, publication year, type of disorder, participant age interval, sample size in both internet-based and face-to-face groups, outcome measure, type of outcome measure (categorized as “clinician-rated,” “self-rated,” “parent-rated,” or a “physiological measure”), pre- and posttreatment means and standard deviations of outcome measures, number of modules and sessions, weeks of therapy in both groups, and assessment of study quality.
Assessment of study quality
All included studies were assessed using a quality assessment instrument,[16] a scale of study quality on 23 different characteristics, each assessed on a 3-point scale (0 = poor, 1 = fair, 2 = good) including the ratings on appropriate sample size, study design, statistical analyses, and presentation of outcomes. In the original article, the mean ratings of 30 mental health trials were between 16.3 (SD = 6.3) and 20.9 (SD = 9.0) and the interrater reliability was in a good range (r = 0.75-0.86).[16] Each article was evaluated independently by two authors. Both authors' scores are reported in [Tables 1 and 2]. The interrater reliability of these scores was good (r = 0.85).
Table 1.
Overview of included studies (part 1)
| Number | Country | Year | Anxiety type | Age | N INT | N FTF | Dropouts (%) | Measures | Outcome Informant |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Sweden | 2005 | Panic | 18-60 | 25 | 24 | 12 | BSQ | Self-rated |
| 2 | Sweden | 2009 | Spider phobia | 18-65 | 15 | 15 | 10 | BAT | Self-rated |
| 3 | Spain | 2010 | Public speaking | +18 | 62 | 36 | 55 | FPSQ | Self-rated |
| 4 | Sweden | 2010 | Panic | +18 | 53 | 60 | 18 | PDSS | Clinical rated |
| 5 | Sweden | 2011 | Social | 18-64 | 64 | 62 | 12 | LSAS | Self-rated |
| 6 | Australia | 2011 | General | 12-18 | 44 | 44 | SCAS | Clinical rated | |
| 7 | Australia | 2011 | Social | Mean 31 | 23 | 14 | 32 | SIAS | Self-rated |
| 8 | Sweden | 2014 | Social | 18-64 | 64 | 62 | 18 | LSAS | Self-rated |
BAT=Behavioral Approach Test, BSQ=The Body Sensations Questionnaire, FPSQ=Fear of Public Speaking Questionnaire, LSAS=Leibowitz Social Anxiety Scale, PDSS=Panic Disorder Severity Scale, SCAS: C/P=Spence Children Anxiety Scale: Child and Parent version, SIAS=Social Interaction Anxiety Scale, w=Weeks
Table 2.
Overview of included studies (part 2)
| Number | Mean (SD) INT pre | Mean (SD) INT post | Mean (SD) FTF pre | Mean (SD) FTF post | Type of therapy (sessions; duration) | Study quality Rater 1 | Study quality Rater 2 |
|---|---|---|---|---|---|---|---|
| 1 | 48.7 (11.7) | 31.8 (11.6) | 52.6 (10.8) | 31.3 (9.1) | INT: CBT (10;10 w) | 36 | |
| FTF: CBT (10;10 w) | 31 | ||||||
| 2 | 10.5 (1.5) | 11.1 (1.2) | INT: CBT (4;5 w) | 31 | |||
| FTF: CBT (2;1 w) | 24 | ||||||
| 3 | 53.3 (14.3) | 39.7 (15.5) | 50.5 (11.9) | 39.3 (13) | INT: CBT (8; - w) | 37 | |
| FTF: CBT (8;16 w) | 36 | ||||||
| 4 | 14.1 (4.3) | 6.3 (4.7) | 14.2 (4) | 6.3 (5.6) | INT: CBT (10;10 w) | 35 | |
| FTF: GCBT (10;10 w) | 35 | ||||||
| 5 | 68.4 (21) | 39.4 (19.9) | 9.71 (22.9) | 48.5 (25) | INT: CBT (15;15 w) | 36 | |
| FTF: GCBT (15;15 w) | 36 | ||||||
| 6 | 5.91 | 3.85 (2.12) | 6.5 | 4.8 (3.4) | INT: CBT (10;10 w) | 37 | |
| FTF: CBT (10;10 w) | 41 | ||||||
| 7 | 54.5 (12.4) | 44 (15.9) | 57.8 (43.9) | 43.9 (18.7) | INT: CBT (8;6 w) | 21 | |
| FTF: GCBT (7;7 w) | 21 | ||||||
| 8 | 65 (23.6) | 34.9 (21.1) | 74 (21.5) | 40.7 (23.6) | INT: CBT (15;15 w) | 37 | |
| FTF: GCBT (15;15 w) | 41 |
CBT=Cognitive behavior therapy, FTF=Face-to-face treatment, GCBT=Group cognitive behavior therapy, INT=Internet treatment, w=Weeks
Statistical analysis
Data were analyzed using Cochrane Review Manager (RevMan) version 5.3.[17] Using the chosen outcome in each study, a random-effects meta-analysis was carried out [Tabls 1 and 2]. In the primary meta-analysis, we evaluated the effect of ICBT compared to face-to-face treatment using the standardized mean difference posttreatment (Hedges' g) as the outcome, meaning that the difference between treatments was divided by the pooled standard deviation. If both intention-to-treat and per-protocol data were presented, the earlier estimation was used in the meta-analysis. Estimates of treatment effects were conducted using all included studies as well as separately for each anxiety disorder (e.g., social anxiety). Possible differences in dropout rates between ICBT and face-to-face treatment were analyzed using meta-analytic logistic regression. All pooled analyses were conducted in a random-effects model framework, assuming variation in true effects in the included studies and accounting for the hypothesized distribution of effects.[8] Forest plots were also inspected to assess variation in effects across studies.
Results
Systematic review
Included studies
The database search that covered the period from Sept 2019 to Oct 2019 resulted in 236 articles; on screening, 8 of them met all the inclusion criteria and were included in the study [Figure 1]. One of them[18] was a long-term follow-up of another study[19] and was not reported separately. Thus, eight studies were included in the systematic review of the meta-analysis (n = 537). A total of eight studies investigated ICBT against some form of CBT (individual format, n = 4 or group format, n = 4).
In terms of disorder studied, three of the studies targeted social anxiety,[18,19,20] two of them panic disorder,[14,21] one adolescence anxiety,[11] one spider phobia,[13] and one fear of public speaking.[15] The total number of participants was 348 in ICBT and 316 in face-to-face conditions. The studies were carried out in Australia, Spain, and Sweden. The smallest study had 47 participants and the largest had 126. All studies were published between the years 2005 and 2014. The characteristics of each study are presented in Table 1.
Duration and intensity
ICBT interventions included between 4 and 15 treatment modules (M = 10, Md = 10) that were to be completed in 5-15 weeks (M = 10.87, Md = 10). Face-to-face treatments consisted of 2 and 15 sessions that were held between 1 and 15 weeks. Five interventions had “once a week” format with approximately the same number of treatment modules and weeks. One intervention had more weeks than modules in ICBT[20] and two had more modules than weeks.[13,15]
Treatment adherence
Treatment adherence was not systematically reported. Three studies reported the mean number of modules completed in ICBT and sessions attended in CBT within the treatment period,[11,14,20] and three studies reported both the average number of completed modules and sessions and also the proportion that completed all modules.[18,19,21] One study reported the number of dropouts,[15] and one study presented no clear definition of treatment adherence.[13]
Outcome informant
Two out of eight studies used clinician-rated symptom severity as the primary outcome[11,14] and the other six used self-rated measures.[13,15,18,19,20]
Overall study quality
The included studies had a total score on the Moncrieff rating scale ranging from 21 to 37 points (M = 33.75, SD = 36). For total rating of, each study see Table 1. One out of eight studies reported a power calculation with full details (study 6), and two studies mentioned power calculation without details. Seven of eight studies had a specified primary outcome measure (studies 1, 2, 3, 4, 5, 6, and 8). Six of the studies used blind assessors (studies 1, 4, 5, 6, 7, and 8), but testing of blinding was reported in three of them (studies 5, 6, and 8). Half of the trials included a representative sample (e.g., all consecutive admissionsat a clinic against volunteers; studies 4, 5, 7, and 8). Seven of the studies presented their results from intention-to-treat analyses (1, 2, 4, 5, 6, 7, and 8).
Meta-analysis
Main findings: ICBT vs. face-to-face treatment
All studies
A forest plot displaying the effect sizes of studies is presented in Figure 2. As shown in theresults, an effect size estimate (g) below 0 favors ICBT, while an effect size above 0 represents larger effects for face-to-face CBT. The pooled between-group effect size posttreatment across all eight studies was g = 0.01 (95% CI: −0.16 to 0.18), showing that ICBT and face-to-face treatment produced equivalent overall effects. Two studies[11,12] were excluded from the meta-analysis because the SD of pre-tests was not reported. The results are presented separately below.
Figure 2.

Forest plot displaying effect sizes of studies comparing internet-based treatment with face-to-face treatment
Social anxiety disorder
The pooled between-group effect size in the three studies targeting social anxiety disorder[18,19,20] was g = 0.04 (95% CI: −0.19 to 0.27) in line with the notion of equivalent effects.
Panic disorder
The pooled between-group effect size in the two studies targeting panic disorder[14,21] was g = −0.17 (95% CI: −0.48 to 0.14), which represents a nonsignificant effect in favor of ICBT. However, the sample size in the first study[21] was small.
Fear of public speaking
The pooled between-group effect size in one study targeting fear of public speaking[15] was g = 0.25 (95% CI: −0.16 to 0.67) in favor of face-to-face treatment; but given the smaller size of the face-to-face group, the finding was not significant.
Publication bias
Figure 3 displays a funnel plot relating effect sizes on the main outcomes of the studies to the standard errors of the estimates. As shown in Figure 3, the effect size was evenly distributed around the averaged effect. The lower left section of the funnel plot includes studies suggesting that there is no major bias of the pooled effect estimate. This is due to small unpublished studies with results favoring internet treatment.
Figure 3.

Funnel plot to assess for publication bias by relating effect sizes of studies to standard errors. SMD = standardized mean difference
Test of heterogeneity
Tests showed significant heterogeneity (χ2 = 8.97; I2 = 44%; P = 0.11), as found in Figure 2. This heterogeneity was largely driven by the study of ICBT vs. face-to-face CBT for panic disorder by Carlbring et al. (2005).[21] If this study was removed from the analysis, I2 dropped from 44 to 27 and heterogeneity would decrease significantly. The pooled effect size across all studies changed marginally from g = 0.01 (95% CI: −0.16 to 0.18) to g = −0.06 (95% CI: −0.11 to 0.24) if this study was removed from the analysis.
Discussion
The main findings showed that both internet-based and face-to-face CBT are equally effective in treating five different anxiety disorders. The meta-analysis showed that dropouts did not systematically favor one treatment format over the other.
Although there were no special effects in favor of either ICBT or face-to-face treatment, there were some fascinating nonsignificant results in reverse direction, depending on the disorder. Most noticeable was the nonsignificant superiority of internet over face-to-face therapy. A possible cause for this is that in one study with g = −0.17, the sample size of face-to-face group was smaller than the internet group[20] and in another study with g = −0.51, the sample size was small in general.[21] In two studies, there were effect sizes in favor of face-to-face treatment, which could be explained by the high effectiveness of the gold standard face-to-face treatment.[8] The other important difference was that in the treatment of social anxiety disorder, the results were moderately in favor of ICBT.[18,20] Probably, this non significant finding can be accepted in light of the possibility that the therapist itself could be a phobic object and the therapeutic relationship would increase anxiety in these patients. Also, in face-to-face treatment, the patient's self-focus will be raised, and therefore, his/her ability to completely concentrate on the therapy might be prevented.[8]
The quality of the studies differed both in terms of accuracy and sample size. However, study quality did not influence the outcome significantly, although the number of studies was too small to reach this conclusion with confidence. Moreover, there was no major bias of the pooled effect estimate. The current meta-analysis had some strong points, including a persistent result across studies concerning the effectiveness of ICBT compared to face-to-face CBT and the reasonably high quality of the trials included. Nevertheless, the study also had limitations. First, there was a possible problem with heterogeneity. Since this was driven by a single extreme value on the panic disorder[21] that favored ICBT, we decided to report the findings both with and without that study included in the analysis. However, the relative effect of that study on the pooled effect size across all studies was insignificant, with g = 0.01 changing to g = −0.06 if it was excluded.
Second, it has been pointed out that internet interventions have high potential for reducing emotional distress, enhancing mental health, and promoting well-being, but there could also be negative impacts related to treatment, though a meta-analysis found that the condition of 5.8% of participants involved in ICBT worsened.[22] This number compares well with the 5%–10% found in face-to-face treatments[23] and is much lower than the 17.4% of the control group participants in internet-delivered trials.[22] In a recent study that investigated the remission rates in ICBT, symptom severity seems to be predictive of outcome inversely, while having more symptoms and being a female increase the chance of improvement.[24]
Third, the treatment review is based only on CBT, which makes it hard to generalize to other treatment approaches. Whereas the great majority of present treatments are based on cognitive-behavior platforms, there are other forms of internet-delivered psychotherapy, such as psychodynamic psychotherapy,[25] physical exercise,[26] and different forms of ICBT, including attention bias modification,[27] problem-solving therapy,[28] and acceptance and commitment therapy.[29] These internet-based intervention programs were not included in the analysis since they generally do not make a direct comparison with face-to-face psychotherapy. Although these clinical approaches are not as popular as CBT in online interventions, since psychodynamic treatment has been found to work in a few trials, it is suggested to study this intervention as well. However, for most conditions such as anxiety disorders and health problems, they are very few, if any, other psychotherapy orientations tested and CBT is unchallenged.[30]
Fourth, we have compared ICBT to face-to-face therapy regardless of whether it was delivered in an individual or a group setting. To resolve the relative efficacy of individual and group settings, head-to-head comparisons need to be conducted.[8]
Fifth, we analyzed only the primary outcome measures in the studies (e.g., Leibowitz Social Anxiety Scale [LSAS]); we did not include the secondary outcomes (e.g., The Spence Children's Anxiety Scale [SCAS]). We cannot, at this point and with the few studies available for each condition, conclude that ICBT and face-to-face therapy are equally effective in all conditions. For example, there are very few studies on gaining knowledge following CBT and even fewer on ICBT,[31] and the therapy formats may vary in this regard. Moreover, patient characteristics such as cognitive flexibility[32] have not been considered. This is possibly important since studies are suggesting that different predictors of outcome are relevant when comparing face-to-face treatment vs. internet treatment.[33] Therefore, we suggest future reviews to analyze secondary outcomes as well and also consider different variables such as cognitive flexibility in the study.
Finally, most of the studies recruited participants only across self-referral or using a combination of self-referral and clinical recruitment. It has been proposed that recruiting through sources that suggest more active treatment-seeking behaviors (e.g., Google searches, viewing postings on mental health websites) leads to participants with more severe anxiety than those recruited through more passive sources of information.[8] So, it is suggested that future researches recruit through the digital footprint of users all over the world to find out who is seeking therapy.
The results of our meta-analysis are interesting both from theoretical and practical standpoints. In terms of theories about change in psychotherapeutic interventions, the findings suggest that the role of a face-to-face therapist may not be as essential as suggested in the previous literature for producing large treatment effects.[34] Even if factors such as therapeutic alliance are established in guided ICBT, they are hardly important for its outcome.[35] Indeed, understanding what makes ICBT work is a challenge for future research, as only a few studies to date have examined the mediators of outcome.[36,37,38]
Conclusions
The results show that the two treatment formats are equally effective in treating social anxiety disorder, adolescent anxiety, panic disorder, spider phobia, and fear of public speaking.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Andersson E, Ljótsson B, Hedman E, Kaldo V, Paxling B, Andersson G, et al. Internet-based cognitive behavior therapy for obsessive compulsive disorder: A pilot study. BMC Psychiatry. 2011:11. doi: 10.1186/1471-244X-11-125. doi: 10.1186/1471-244X-11-125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Vigerland S, Lenhard F, Bonnert M, Lalouni M, Hedman E, Ahlen J, et al. Internet-delivered cognitive behavior therapy for children and adolescents: A systematic review and meta-analysis. Clin Psychol Rev. 2016;50:1–10. doi: 10.1016/j.cpr.2016.09.005. [DOI] [PubMed] [Google Scholar]
- 3.Guided internet-based treatments in psychiatry. Place of publication not identified: Springer International PU. New York, NY: Springer Berlin Heidelberg; 2016. ISBN 978-3-319-06082-8. [Google Scholar]
- 4.Lindefors N, Hedman E, Ljótsson B. Internet-based cognitive behavior therapy for anxiety and depression. In: Zohar J, editor. Anxiety and Depression: The Möbius. Strip Neuilly-sur-Seine: Laboratoires Servier; 2012. [Google Scholar]
- 5.Andersson G, Carlbring P, Lindefors N. History and current status of ICBT. In: Lindefors N, Andersson G, editors. Guided Internet-Based Treatments in Psychiatry. New York, NY: Springer; 2016. pp. 1–16. [Google Scholar]
- 6.Andersson G, Carlbring P, Hadjistavropoulos HD. Internet-based cognitive behavior therapy. In: Hofmann SG, Asmundson GJG, editors. The Science of Cognitive Behavioral Therapy. San Diego, CA: Academic Press; 2017. pp. 531–49. [Google Scholar]
- 7.Hedman E, Furmark T, Carlbring P, Ljótsson B, Ruck C, Lindefors N, et al. A 5-year follow-up of Internet-based cognitive behavior therapy for social anxiety disorder. J Med Internet Res. 2011;13:e39. doi: 10.2196/jmir.1776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Carlbring P, Andersson G, Cuijpers P, Riper H, Hedman-Lagerlöf E. Internet-based vs.face-to-face cognitive behavior therapy for psychiatric and somatic disorders: An updated systematic review and meta-analysis. Cogn Behav Ther. 2017;47:1–18. doi: 10.1080/16506073.2017.1401115. [DOI] [PubMed] [Google Scholar]
- 9.Andersson G, Cuijpers P, Carlbring P, Riper H, Hedman E. Guided Internet-based vs.face-to-face cognitive behavior therapy for psychiatric and somatic disorders: A systematic review and meta-analysis. World Psychiatry. 2014;13:288–95. doi: 10.1002/wps.20151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Boettcher J, Carlbring P, Renneberg B, Berger T. Internet-based interventions for social anxiety disorder-an overview. Verhaltenstherapie. 2013;23:160–8. [Google Scholar]
- 11.Spence SH, Donovan CL, March S, Gamble A, Anderson RE, Prosser S, et al. A randomized controlled trial of online versus clinic-based CBT for adolescent anxiety. J Consult Clin Psychol. 2011;79:629–42. doi: 10.1037/a0024512. [DOI] [PubMed] [Google Scholar]
- 12.Andersson G. Using the Internet to provide cognitive behaviour therapy. Behav Res Ther. 2009;47:175–80. doi: 10.1016/j.brat.2009.01.010. [DOI] [PubMed] [Google Scholar]
- 13.Andersson G, Waara J, Jonsson U, Malmaeus F, Carlbring P, Ost LG. Internet-based self-help versus one-session exposure in the treatment of spider phobia: A randomized controlled trial. Cogn Behav Ther. 2009;38:114–20. doi: 10.1080/16506070902931326. [DOI] [PubMed] [Google Scholar]
- 14.Bergström J, Andersson G, Ljótsson B, Ruck C, Andreewitch S, Karlsson N, et al. Internet-versus group-administered cognitive behaviour therapy for panic disorder in a psychiatric setting: A randomised trial. BMC Psychiatry. 2010:10. doi: 10.1186/1471-244X-10-54. doi: 10.1186/1471-244X-10-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Botella C, Gallego M, Garcia-Palacios A, Guillen V, Banos RM, Quero S, et al. An Internet-based self-help treatment for fear of public speaking: A controlled trial. Cyberpsychol Behav Soc Netw. 2010;13:407–21. doi: 10.1089/cyber.2009.0224. [DOI] [PubMed] [Google Scholar]
- 16.Moncrieff J, Churchill R, Drummond DC, Mcguire H. Development of a quality assessment instrument for trials of treatments for depression and neurosis. Int J Methods Psychiatr Res. 2001;10:126–33. [Google Scholar]
- 17.Higgins JPT, Green S. Newark: John Wiley and Sons; 2011. Cochrane Handbook for Systematic Reviews of Interventions. ISBN 978-0470057964. [Google Scholar]
- 18.Hedman E, Alaoui SE, Lindefors N, Andersson E, Ruck C, Ghaderi A, et al. Clinical effectiveness and cost-effectiveness of Internet- vs.group-based cognitive behavior therapy for social anxiety disorder: 4-Year follow-up of a randomized trial. Behav Res Ther. 2014;59:20–9. doi: 10.1016/j.brat.2014.05.010. [DOI] [PubMed] [Google Scholar]
- 19.Hedman E, Andersson E, Ljótsson B, Andersson G, Rück C, Lindefors N. Cost-effectiveness of Internet-based cognitive behavior therapy vs. cognitive behavioral group therapy for social anxiety disorder: Results from a randomized controlled trial. Behav Res Ther. 2011;49:729–36. doi: 10.1016/j.brat.2011.07.009. [DOI] [PubMed] [Google Scholar]
- 20.Andrews G, Davies M, Titov N. Effectiveness randomized controlled trial of face to face versus Internet cognitive behaviour therapy for social phobia. Aust N Z J Psychiatry. 2011;45:337–40. doi: 10.3109/00048674.2010.538840. [DOI] [PubMed] [Google Scholar]
- 21.Carlbring P, Nilsson-Ihrfelt E, Waara J, Kollenstam C, Buhrman M, Kaldo, et al. Treatment of panic disorder: Live therapy vs.self-help via the Internet. Behav Res Ther. 2005;43:1321–33. doi: 10.1016/j.brat.2004.10.002. [DOI] [PubMed] [Google Scholar]
- 22.Rozental A, Magnusson K, Boettcher J, Andersson G, Carlbring P. For better or worse: An individual patient data meta-analysis of deterioration among participants receiving Internet-based cognitive behavior therapy. J Consult Clin Psychol. 2017;85:160–77. doi: 10.1037/ccp0000158. [DOI] [PubMed] [Google Scholar]
- 23.Hansen NB, Lambert MJ, Forman EM. The psychotherapy dose-response effect and its implications for treatment delivery services. Clinical Psychology: Science and Practice. 2006;9:329–43. [Google Scholar]
- 24.Andersson G, Carlbring P, Rozental A. Response and remission rates in Internet-based cognitive behavior therapy: An individual patient data meta-analysis. Front Psychiatry. 2019;10:749. doi: 10.3389/fpsyt.2019.00749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Johansson R, Ekbladh S, Hebert A, Lindström M, Möller S, Petitt E, et al. Psychodynamic guided self-help for adult depression through the Internet: A randomised controlled trial. PLoS One. 2012;7:e38021. doi: 10.1371/journal.pone.0038021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Nyström MB, Stenling A, Sjöström E, Neely G, Lindner P, hassmén P, et al. Behavioral activation versus physical activity via the Internet: A randomized controlled trial. J Affect Disord. 2017;215:85–93. doi: 10.1016/j.jad.2017.03.018. [DOI] [PubMed] [Google Scholar]
- 27.Carlbring P, Apelstrand M, Sehlin H, Amir N, Rousseau A, Hofmann S, et al. Internet-delivered attention bias modification training in individuals with social anxiety disorder-A double blind randomized controlled trial? BMC Psychiatry. 2012;12:1–9. doi: 10.1186/1471-244X-12-66. doi: 10.1186/1471-244X-12-66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Warmerdam L, Straten AV, Twisk J, Riper H, Cuijpers P. Internet-based treatment for adults with depressive symptoms: Randomized controlled trial. J Med Internet Res. 2008:10. doi: 10.2196/jmir.1094. doi: 10.2196/jmir.1094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ivanova E, Lindner P, Ly KH, Dahlin M, Vernmark k, Andersson G, et al. Guided and unguided acceptance and commitment therapy for social anxiety disorder and/or panic disorder provided via the Internet and a smartphone application: A randomized controlled trial. J Anxiety Disord. 2016;44:27–35. doi: 10.1016/j.janxdis.2016.09.012. [DOI] [PubMed] [Google Scholar]
- 30.Andersson G. The Internet and CBT: A Clinical Guide. Boca Raton: CRC Press; 2015. ISBN 9781444170214. [Google Scholar]
- 31.Andersson G, Carlbring P, Furmark T. Therapist experience and knowledge acquisition in Internet-delivered CBT for social anxiety disorder: A randomized controlled trial. PLoS One. 2012;7:e37411. doi: 10.1371/journal.pone.0037411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lindner P, Carlbring P, Flodman E, Hebert A, Poysti S, Hagkvist, et al. Does cognitive flexibility predict treatment gains in Internet-delivered psychological treatment of social anxiety disorder, depression, or tinnitus? Peer J. 2016;4:e1934. doi: 10.7717/peerj.1934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ebert DD, Donkin L, Andersson G, Andrews G, Berger T, Carlbring P, et al. Does Internet-based guided-self-help for depression cause harm? An individual participant data meta-analysis on deterioration rates and its moderators in randomized controlled trials. Psychol Med. 2016:46. doi: 10.1017/S0033291716001562. 2679-93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wampold BE. Mahwah, NJ: Lawrence Erlbaum; 2001. The Great Psychotherapy Debate: Models, Methods, and Findings. ISBN 10: 0805832017. ISBN 13: 9780805832013. [Google Scholar]
- 35.Andersson G, Paxling B, Wiwe M, Vernmark K, Felix CB, Lundborg L, et al. Therapeutic alliance in guided internet-delivered cognitive behavioral treatment of depression, generalized anxiety disorder and social anxiety disorder. Behav Res Ther. 2012;50:544–50. doi: 10.1016/j.brat.2012.05.003. [DOI] [PubMed] [Google Scholar]
- 36.Hedman E, Andersson E, Andersson G, Lindefors N, Lekander M, Rück C, et al. Mediators in internet-based cognitive behavior therapy for severe health anxiety. PLoS One. 2013:8. doi: 10.1371/journal.pone.0077752. doi: 10.1371/journal.pone.0077752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hesser H, Westin VZ, Andersson G. Acceptance as a mediator in internet-delivered acceptance and commitment therapy and cognitive behavior therapy for tinnitus. J Behav Med. 2014;37:756–67. doi: 10.1007/s10865-013-9525-6. [DOI] [PubMed] [Google Scholar]
- 38.Karyotaki E, Kleiboer A, Smit F, Turner DT, Pastor AM, Andersson G, et al. Predictors of treatment dropout in self-guided web-based interventions for depression: An ‘individual patient data’ meta-analysis. Psychol Med. 2015;45:2717–26. doi: 10.1017/S0033291715000665. [DOI] [PubMed] [Google Scholar]