
Figure 2.
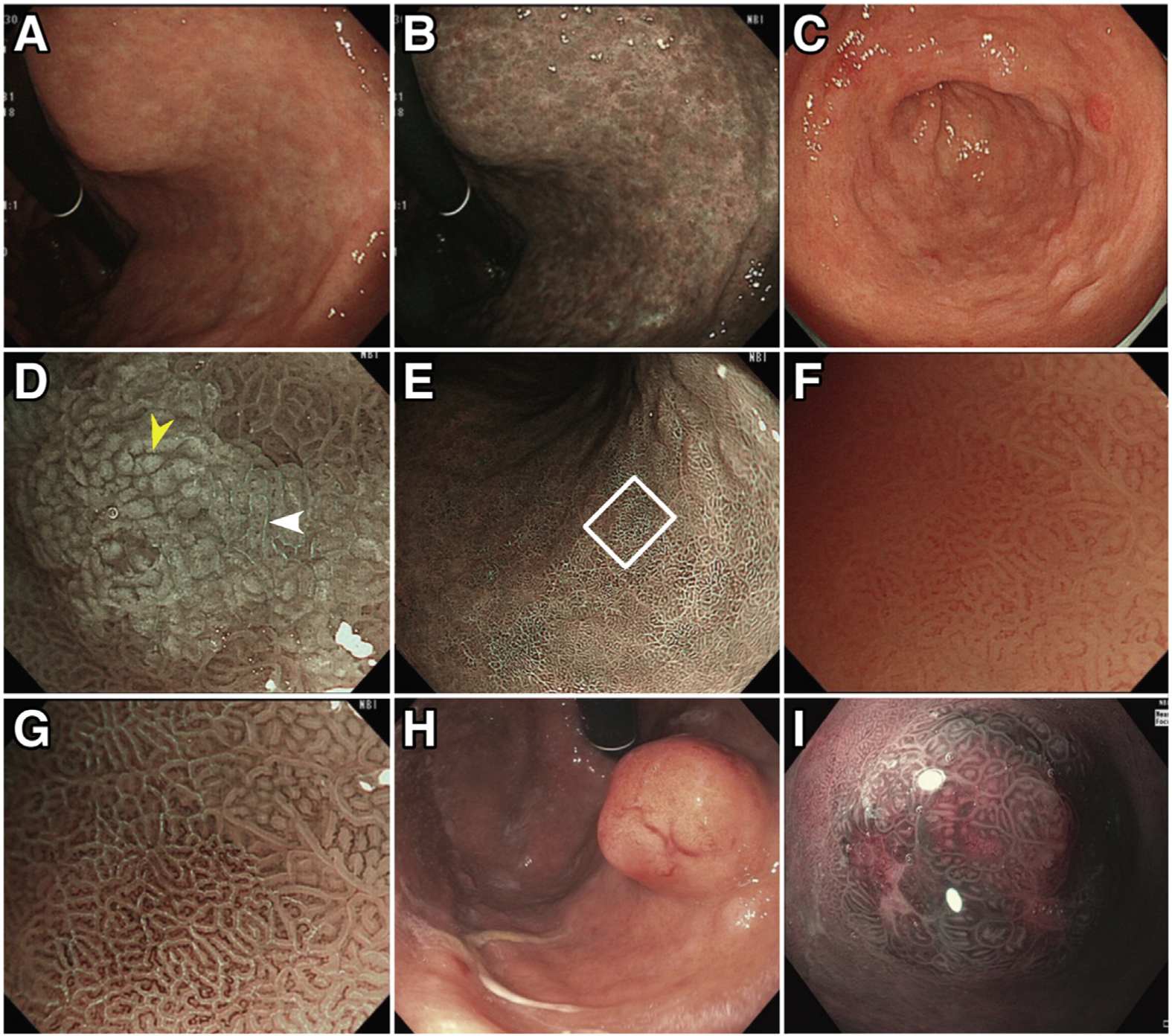
Typical endoscopic appearance of chronic AG, IM, and gastric NET. Characteristic endoscopic features of chronic AG include pale appearance of mucosa, loss of gastric rugal folds, and prominence of submucosal blood vessels due to thinning of the atrophied gastric epithelium, as shown in (A) HD-WLE and (B) NBI. Changes representing IM are frequently found in chronic AG (C–G). On HD-WLE, the areas with IM typically appear mildly nodular (C). On magnifying NBI (D), characteristic signs of IM include the LBC (white arrowhead) and white opaque field (WOF, yellow arrowhead) (or white opaque substance [WOS]). The LBC sign refers to the fine, blue-white lines on the crests of the epithelial surface, which correspond to histologic finding of the brush border (microvilli). The WOF (or WOS) is caused by light scattering at microscopic lipid droplets that accumulate in the mucosa of IM. Both LBC and WOF/WOS signs are best visualized using magnifying NBI. IM in the flat gastric mucosa is shown in (E) (nonmagnifying NBI image). (F, G) Magnified views of IM (white square [E]) with and without NBI, respectively, with abundant LBCs visible in (G). Note that areas of IM with LBC coexist with non-IM mucosa (right upper corner of [G]). (H) and (I) demonstrate endoscopic appearance of gastric NETs on HD-WLE (H) and near-focus NBI (I).