
FIGURE 1.
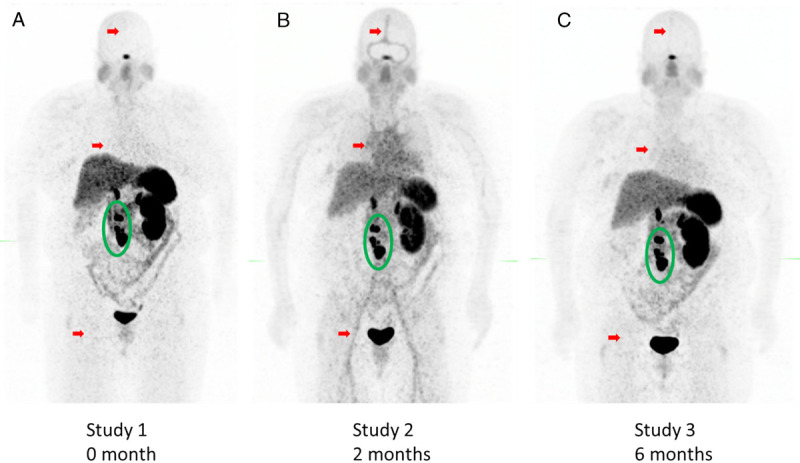
MIP images of serial 68Ga-DOTATATE PET studies of a woman with biopsy-proven metastatic well-differentiated neuroendocrine tumor (WHO grade 1). Initial time point (A) demonstrates 68Ga-DOTATATE–avid retroperitoneal nodal disease (green circle) and typical low blood pool activity (red arrows). Follow-up 68Ga-DOTATATE PET (B) after commencement of lanreotide therapy demonstrates interval increased blood pool uptake (red arrows) and interval decreased uptake in the liver, spleen, and retroperitoneal lymph nodes (green circle). Subsequent 68Ga-DOTATATE PET (C) demonstrated interval resolution of blood pool uptake (red arrows) and increased 68Ga-DOTATATE uptake in retroperitoneal lymph nodes (green circle). As seen here, physiologic biodistribution of 68Ga-DOTATATE includes the pituitary and salivary glands, liver, spleen, kidney, adrenals, pancreas, and some gastrointestinal and marrow uptake.1,2 Increased blood pool component has been described for 67Ga-citrate but not for 68Ga-DOTATATE,3 and 68Ga-DOTATATE has been shown to have high in vitro and in vivo stability at many time points.4,5 However, informal communications with the manufacturer and unpublished work from our radiochemistry department have confirmed that 68Ga can have suboptimal binding to the DOTA cage and may bind to blood products such as transferrin.6 The high blood pool 68Ga uptake in this patient is believed to be unbound 68Ga, as DOTA conjugated 68Ga clears rapidly from the blood.7 The probability of unbound 68Ga is most likely independent of the production of 68Ga, whether via generator or cyclotron.8,9 Preclinical studies demonstrates that 177Lu-DOTATATE has similar binding stability to 68Ga-DOTATATE,10 and thus although rare, incomplete binding of 177Lu-DOTATATE could in theory result in suboptimal treatments.