
FIGURE 4.
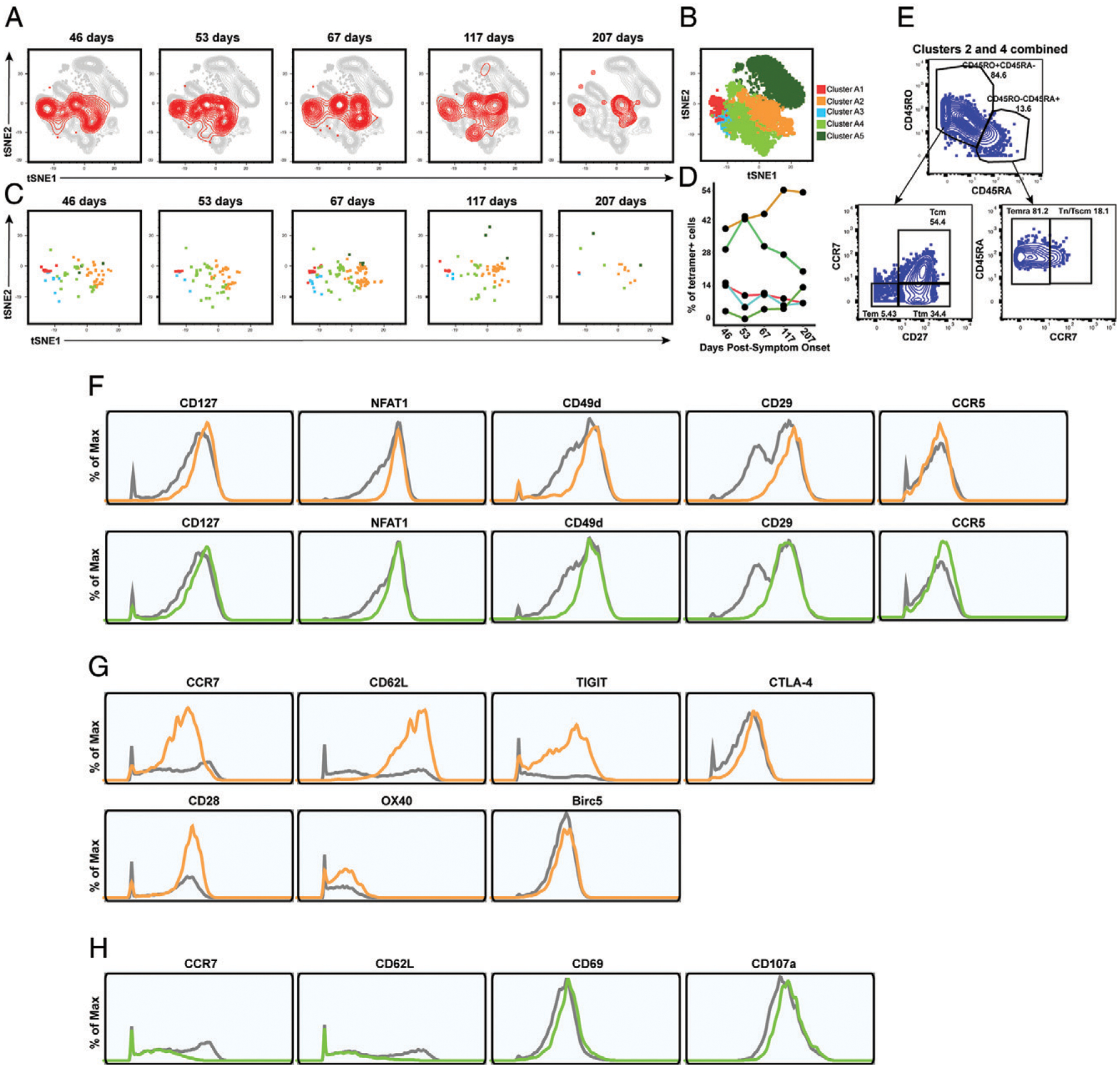
Clusters of Nuc322–331–specific CD8+ T cells from PID4103 exhibit different expansion and contraction. (A) The overall phenotypes of Nuc322–331–specific CD8+ T cells change over the course of convalescence. tSNE plots of total (gray) and tetramer+ (red) CD8+ T cells as a function of time since symptom onset. (B) FlowSOM clusters of CD8+ T cells. Total CD8+ T cells (including the tetramer+ cells) were clustered by FlowSOM to identify five clusters. The location of each cluster is mapped onto the tSNE space depicted in (A). (C) Distribution over time of Nuc322–331–specific CD8+ T cells among the five clusters identified in (B). (D) Proportion of Nuc322–331–specific CD8+ T cells in each cluster as a function of time since symptom onset. The dominant clusters, A2 and A4, increase and decrease over time, respectively. (E) Clusters A2 and A4 include multiple cellular subsets. Gating strategy showing the identification of the Tcm, Tem, Ttm, Temra, and Tn/Tscm subsets, all of which were well-represented among the two dominant clusters. (F) Phenotypic features shared by clusters A2 and A4. Relative to total CD8+ T cells, clusters A2 and A4 expressed high levels of CD127, the transcription factor NFAT1, and the lung-homing receptors CD49d, CD29, and CCR5. Total CD8+ T cells are depicted in gray, cluster A2 cells are depicted in orange, and cluster A4 cells are depicted in green. (G) Phenotypic features exhibited by cluster A2 and not A4. Cluster A2, whose contribution among tetramer+ cells increased over the course of convalescence, expressed high levels of the lymph node–homing receptors CCR7 and CD62L, the checkpoint molecules TIGIT and CTLA4, the costimulatory molecules CD28 and Ox40, and the prosurvival factor BIRC5. Total CD8+ T cells are depicted in gray, and cluster A2 cells are depicted in orange. (H) Phenotypic features exhibited by cluster A4 and not A2. Cluster A4, whose contribution among tetramer+ cells decreased over the course of convalescence, expressed low levels of the lymph node–homing receptors CCR7 and CD62L, high levels of the activation marker CD69, and high levels of the degranulation marker CD107a.