

Abstract
Non-medical use of prescription and non-prescription drugs is a worldwide epidemic, rapidly growing in magnitude with deaths due to overdose and chronic use. A vast majority of these drugs are stimulants that have various effects on the cardiovascular system including the cardiac rhythm. Drugs, like cocaine and methamphetamine, have measured effects on the conduction system and through several direct and indirect pathways, utilizing multiple second messenger systems, change the structural and electrical substrate of the heart, thereby promoting cardiac dysrhythmias. Substituted amphetamines and cocaine affect the expression and activation kinetics of multiple ion channels and calcium signaling proteins resulting in EKG changes, and atrial and ventricular brady and tachyarrhythmias. Pre-existing conditions cause substrate changes in the heart which decrease the threshold for such drug-induced cardiac arrhythmias. The treatment of cardiac arrhythmias in patients who take drugs of abuse may be specialized and will require an understanding of the unique underlying mechanisms and necessitates a multi-disciplinary approach. The use of primary or secondary prevention defibrillators in drug abusers with chronic systolic heart failure is both sensitive and controversial. This review provides a broad overview of cardiac arrhythmias associated with stimulant substance abuse and their management.
Keywords: cocaine, amphetamines, methamphetamines, ecstasy, stimulant drugs of abuse, arrhythmias
Introduction
Non-medical use of prescription and non-prescription drugs is a worldwide epidemic, growing rapidly, leading to overdose deaths and consequences of chronic misuse. Methamphetamine, a stimulant with high potential for abuse, has quickly become the second most commonly abused illicit drug in the United States, second only to marijuana. Stimulants including cocaine and methamphetamine can produce damaging cardiovascular effects and initiate and perpetuate various arrhythmias.
Expert consensus statements and guidelines do not specifically address this issue. This review explores the current state of stimulant drug use, discusses mechanisms of and critically evaluates evidence behind stimulant drug-induced cardiac arrhythmias, and offers management strategies.
Growing Global Drug Problem:
Approximately 269 million people misused drugs for non-medical purposes in 2018, representing 5.3% of the world’s population aged 15–64 (Figure 1). Amphetamines and cocaine are the most widely used stimulants with 48 million and 19 million people, respectively, using these drugs for non-medical purposes in 20181 (Figures 2 and 3). Cocaine (from plants within the Erythroxylaceae family), administered by inhalation, injection, and smoking has a high potential for abuse.
Figure 1:

Global prevalence of drug use and drug use disorders, 2006–2018, Source: World Drug Report 2020 (United Nations publication, Sales No. E.20.XI.6).
Figure 2:
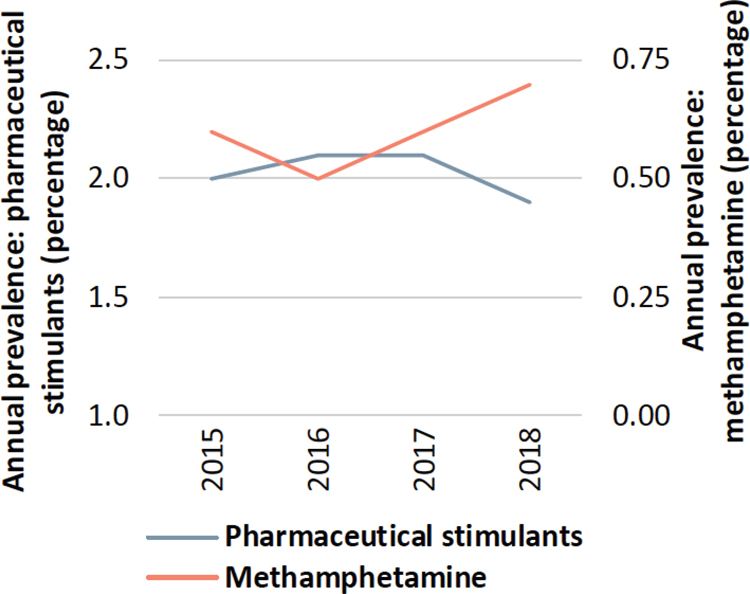
Trends in the misuse of pharmaceutical stimulants and methamphetamines in United States, 2015–2018. Y-axis shows the percentage US population aged 12 and older who misused pharmaceutical stimulants and methamphetamines. While the misuse of pharmaceutical stimulants declined, there was an increase in methamphetamine misuse. Source: World Drug Report 2020 (United Nations publication, Sales No. E.20.XI.6
Figure 3:
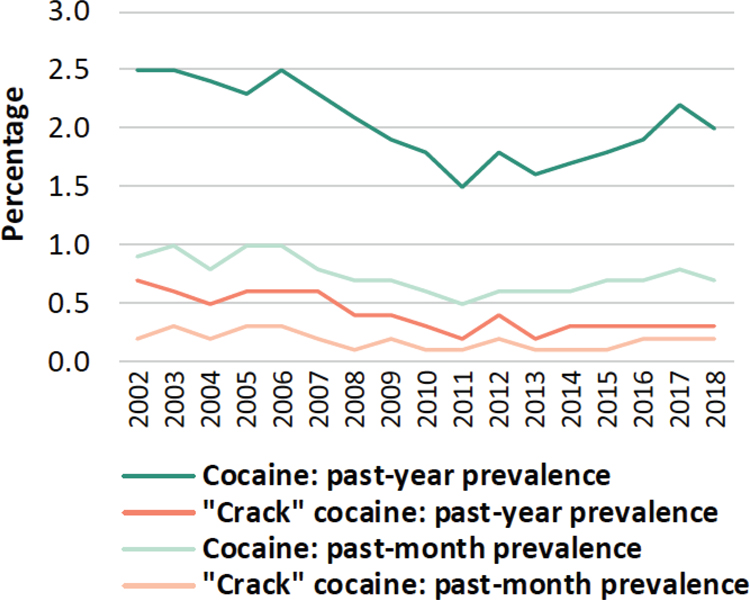
Trends in the use of cocaine and “crack” cocaine, United States, 2002–2018, Y- axis shows the percentage of US population 12 years and older who used cocaine. Source: World Drug Report 2020 (United Nations publication, Sales No. E.20.XI.6).
Medical uses of cocaine include local anesthesia and topical vasoconstriction. Cocaine is classified as a Schedule II drug by the DEA, and its non-medical use is illegal in the United States. Amphetamines represent a class of widely abused central nervous system stimulants. The prototypic drug, amphetamine is medically approved to treat attention deficit hyperactivity disorder (ADHD), narcolepsy, and obesity.
Methamphetamine, an amphetamine derivative, and strong psychostimulant with high potential for misuse, is a schedule II drug, available in powder and pill forms and is administered by injection, smoking, swallowing, and inhalation. “Ecstasy-like” substances, including 3,4-methylenedioxy-methamphetamine (MDMA), are synthesized from the prototypical amphetamine backbone. These drugs produce stimulant (e.g., euphoria), psychedelic (e.g., perceptual changes), and prosocial effects. Ecstasy has no medically accepted use and is classified as a Schedule I drug in the United States. However, the FDA recently gave “breakthrough status” to MDMA for post-traumatic stress disorder, which could speed advancement through clinical trials. (Table 1)
Table 1:
Characteristics of stimulant drugs of abuse
| Drug Name | Street Names | Physical Form | Routes of administration | Estimated prevalence of non-medical use in 2018 |
|---|---|---|---|---|
| Cocaine | Blow, Coca, Coke, Crack, Flake, Snow, Soda Cot | White, crystalline powder | Nasal insufflation, injected, smoked | 19 million |
| Amphetamines (Including amphetamine, methamphetamine phentermine) |
Batu, Bikers Coffee, Black Beauties, Chalk, ChickenFeed, Crank, Crystal, Glass, Go-Fast, Hiropon, Ice, Meth, Methlies Quick, Poor Man’s Cocaine, Shabu, Shards, Speed, Stove Top, Tina, Trash, Tweak, Uppers, Ventana, Vidrio, Yaba, Yellow Bam, Bennies, and Uppers | Pills or powder | Swallowed, nasal insufflation, injected, smoked | 27 million |
| Ecstasy/MDMA | Adam, Beans, Clarity, Disco Biscuit, Ecstasy, Eve, Go, Hug Drug, Lover’s Speed, MDMA, Peace, STP, X, and XTC | Pills, capsules, powder, liquid | Mostly swallowed, sometimes crushed and used for nasal insufflation, occasionally smoked | 21 million |
Pharmacology of Stimulants
Second messenger systems involved in stimulant drug pathophysiology
In the central nervous system (CNS), stimulants interact with monoamine neurons, including dopamine, serotonin, and norepinephrine. At presynaptic terminals, these neurons express specialized plasma membrane proteins transporting neurotransmitters from the extracellular space into the cytoplasm, inactivating neurotransmitter signaling.2 Drugs interacting with transporters are categorized as reuptake inhibitors or substrate-type releasers, based on their mechanism of action. Such compounds stimulate downstream monoamine receptors and signaling systems by increasing extracellular levels of endogenous monoamine neurotransmitters.
Cocaine is a nonselective inhibitor of all three monoamine transporters.3 However, behavioral effects of cocaine associated with abuse liability have been attributed primarily to actions at the dopamine transporter (DAT).4 Neuroimaging studies in human cocaine users correlate levels of DAT occupancy with the magnitude of the “high” following administration of cocaine5 or the DAT inhibitor, methylphenidate.6 Amphetamines, in contrast to cocaine, act as substrate-type releasers allowing intracellular transport through monoamine transporters.
COCAINE
Cocaine and Electrical Remodeling:
The propensity of stimulant drugs to initiate cardiac arrhythmias stems partly from their ability to affect expression or function of cardiac ion channels directly, based on evidence predominantly emanating from their actions on neurons. Direct effects of stimulant drugs on ion channels in isolated cells are independent of catecholaminergic changes that occur in-vivo. (Table 2)
Table 2:
Summary of available evidence of EKG changes in stimulant drugs use
| Study (n = number of patients) | Baseline QTc (means [SD]) | Effect of cocaine and methamphetamine use on QT interval (means [SD]) | Statistically significant (P < 0.05) | |
|---|---|---|---|---|
| Cocaine | Gamouras et al. (n = 45) * | Not reported | QTc in Group I (with chest pain) = 510.0 [84.3] ms QTc Group II (no chest pain) = 459.0 (73.7) ms |
P <0.03 |
| Haigney et al. (n = 29) | Not reported | QTVI† increased within first 5 minutes of cocaine infusion and peaked at 10 minutes. Dose effect seen (higher QTVI for 40mg vs 20mg of cocaine) | P <0.0001 compared with preinfusion | |
| Magnano et al. (n = 14) | 401 [21] ms | QTc = 423 [25] ms | P <0.001 | |
| Chakko et al. (n = 238) | Not reported | QTc prolonged (>440 ms) in 26% of patients admitted for acute cocaine toxicity vs 4% in chronic cocaine users (means 427 [38] vs 404 [19], respectively) | P = 0.00003 | |
| Methamphetamine | Bazmi et al. (n = 230) | Not reported | Sinus tachycardia plus prolonged QT interval in 34.4% of patients | - |
| Haning et al. (n = 158) | Not reported | QTc prolonged (>440ms) in 27.2% of patients | - | |
| Paratz et al. (n = 212) | Not reported | 21.7% of 106 meth users had prolonged QTc‡ with mean of 436.41 [31.61] vs 407.28 [24.38] in control group | P <0.0001 |
ms = milliseconds
Group I consisted of 23 patients with anginal chest pain in addition to cocaine abuse. Group II was composed of 22 patients with cocaine use without a history of chest pain. None of these patients had a prior history of heart disease, nor were any taking antiarrhythmic agents.
QTVI, therefore, is the log ratio between the QT interval and heart rate variability.
As defined by >450 ms for males, >460 ms for females.
The QTc was determined using Bazett’s formula = QT/RR1/2
Cocaine can produce electrical remodeling by altering gating properties of ion channels. Cocaine inhibits several potassium channels. Cocaine blunted action potential duration (APD) shortening effect of ATP-sensitive potassium channel (KATP) openers in murine ventricular myocytes.7 Disruption of the KCNJ11 gene encoding for Kir6, the core forming subunit of KATP channels, augments effects of cocaine on KATP channels.8 A substantial number of cocaine abusers simultaneously, or concurrently, use cocaine and alcohol combinations. Alcohol potentiates actions of cocaine by forming cocaethylene, a metabolite of alcohol and cocaine that inhibits IKr channels.9
Cocaine can inhibit sodium channels in a voltage-dependent fashion, albeit, less than lidocaine.10 Cocaine affects use-dependent inhibition of cardiac sodium channels in two phases (rapid and slower phase).11 Mutations of the interdomain III-IV linker that removed the rapid inactivation selectively abolished these effects of cocaine on sodium channels,12 by binding to a location in the internal vestibule of the sodium channel, blocking the channel pore. Cocaethylene potentiates sodium channel inhibition, mediated by its actions on the extracellular end of the S6 segment of the D4 domain of the sodium channel.13
Cocaine alters function of calcium-related channels and calcium handling proteins. Cocaine blocks the sarcoplasmic reticulum from the cytoplasmic side resulting in reduced current amplitude14 and calcium transients in cocaine-treated rat ventricular myocytes,15 an effect that is accentuated by simultaneous exposure to ethanol and cocaine.16 Cocaine disrupts calcium-dependent oligomerization of calsequestrin 17 by its high affinity binding, thereby affecting sarcoplasmic reticulum calcium storage and release. Finally, cocaine increases calcium calmodulin kinase II activity, which may affect multiple mechanisms of atrial and ventricular arrhythmias.18 Cocaine’s effects on calcium channels and calcium handling proteins is manifested as a dose dependent increase in APD, frequent early afterdepolarizations,19 and field potential duration.20
Cocaine and Structural Remodeling:
Stimulant drugs can cause myocyte cell death and fibrosis resulting in reduced systolic function, increasing the risk of arrhythmias. Cocaine increases the risk of myocardial infarction (MI), heart failure, cardiomyopathy, arrhythmias, aortic dissection, endocarditis, and other cardiovascular diseases.21–24 Cocaine users have a higher overall incidence of MI (odds ratio up to 6.9) versus nonusers,25 with the risk of MI increasing by 24-fold in the first hour after cocaine use.22 Cocaine-induced cardiomyopathy is associated with myocardial inflammation, necrosis, fibrosis,24,26 left ventricular hypertrophy,21 and alterations in gene expression.27 Pre-clinical studies in rabbit models demonstrate regional wall motion abnormalities (mostly anteroseptal) associated with decreased left ventricular fractional shortening and increased systolic dimension with acute cocaine intoxication.28 In mouse models, acute and chronic cocaine-ingestion causes myocardial hypertrophy, contractile dysfunction, and remodeling.29
Cocaine and EKG changes (Table 3):
Table 3:
Effect of Cocaine and Methamphetamines on Ions Channels and EKG
| Cocaine | Methamphetamine | |
|---|---|---|
| Effect of agent on cardiac ion channels | ||
| Na+ (INa) | ⬇ | − |
| K+ | ⬇ (KATP, IKr) | ⬇ (Kto and Kir) |
| Ca2+ | ⬇ & ⬆ (ICa,L =increases with low cocaine concentration, ICa,L = decreases with high cocaine concentrations) | ⬇/⬆ (ICa,L) |
| Effect of agent on EKG | ||
| PR interval | − | − |
| QRS duration | ⬆ | |
| QTc interval | ⬆ | + |
| ST-T wave changes | + | + |
| Atrial dysrhythmias | ||
| Sinus tachycardia | + | + |
| Atrial fibrillation | + | +/− |
| Atrial tachycardias (including SVT) | + | + |
| Ventricular arrhythmias | ||
| Ventricular tachycardia | + | + |
| Ventricular fibrillation | + | ? |
| Torsade de pointes | + | + |
| Bradyarrhythmias | ||
| Bradycardia | + | − |
| Heart block | + | − |
ICa,L = L-type calcium channels
KATP= ATP sensitive potassium channels
IKr= Rapidly activating delayed rectifier potassium channels
Kir= Inwardly rectifying potassium channels
Kto= Transient outward potassium channel
⬆ indicates increase in current or ECG parameter
⬇ indicates decrease in current or ECG parameter
indicates a known effect of the drug on the EKG parameters or cardiac arrhythmias
indicates no effect or unknown effect
indicates unknown or controversial data on effect
Cocaine blocks voltage-dependent potassium channels to prolong QT intervals.30 In addition, cocaine blocks fast inward sodium channels similar to class IC antiarrhythmic drugs31 prolonging QRS duration. Retrospective review of EKGs from 97 cocaine-dependent patients and 8,513 non-using subjects from the Atherosclerosis Risk in Communities study found a notable effect of cocaine on early repolarization (odds ratio=4.92, 95% confidence interval (CI): 2.73–8.87).32 Cocaine’s sympathomimetic effects increased ventricular ectopy.33 Cocaine-induced myocardial ischemia may further promote reentrant tachycardias.34 In patients presenting to the Emergency Department with chest pain, the incidence of cocaine-associated MI was 0.7–6%. EKG abnormalities included ST-elevation, ST-depression, voltage criteria for left ventricular hypertrophy, and non-specific ST and T wave abnormalities.35 Moreover, cocaine-induced Brugada pattern has been described.36,37
Cocaine and Bradyarrhythmias:
While stimulant drugs tend to cause tachyarrhythmias, they can also cause bradyarrhythmias. (Table 2) Various degrees of AV block have been reported with cocaine use.38,39 In animal studies, cocaine can cause rate-dependent conduction delays and prolonged refractoriness in the atria, AV node, His-Purkinje system and ventricular myocardium.40 However, data supporting similar effects in humans is scarce. Sinus bradycardia has been observed with chronic cocaine use 32, 41 the severity of which was related to length of cocaine use. Desensitization of β-adrenergic receptors secondary to repeated cocaine exposure has been postulated.41
Cocaine and Atrial Arrhythmias:
Little evidence implicates a relationship between stimulant drugs and atrial arrhythmias. Sinus tachycardia is the most common arrhythmia that results from cocaine toxicity but supraventricular tachycardia and atrial fibrillation can also occur.31 These tachycardias are primarily due to cocaine’s effect on increasing circulating catecholamines. There is a report of atrial flutter in newborns associated with perinatal maternal cocaine use.42
Cocaine and Ventricular Arrhythmias:
Documentation of ventricular arrhythmias in stimulant drug users is sparse. Patients with cocaine-induced arrhythmias often have additional risk factors for arrhythmias, such as, pre-existing coronary artery disease, myocarditis, or cardiomyopathy (please refer to section on Stimulant Misuse and Co-occurring Risk Factors for Arrhythmias in supplementary material). In cases where these drugs do cause arrhythmias, the patients are usually young, and the heart rhythm usually produces rapid, and erratic death outside the medical system.
Ventricular tachycardia has been reported with cocaine use in patients with myocarditis supported by MRI-proven sub-epicardial scar.43 Reports of frequent premature ventricular contractions (PVCs), non-sustained VT, idioventricular rhythm, sustained VT, VF, torsade de pointes and SCD, have been reported in patients aged 20–44 without underlying ischemia.44 Animal studies indicate post MI episodes of VF after cocaine exposure are reduced by verapamil.45
A prospective study of 10 patients with hypertension and active cocaine use indicated that 1 of 10 patients had non-sustained VT.46 In a study of 45 hospitalized patients for cocaine abuse, those with CP had a longer QTc intervals (510 ms) vs those with no CP (459 ms). Among patients with CP, 13% had sustained ventricular arrhythmias; all had repolarization abnormalities.30 In 7 studies evaluating outcomes of 70,302 patients admitted with cocaine-related CP, 0.8–13%% of those with CP admitted with an MI had sustained ventricular arrhythmias23,47. Brugada syndrome-like EKG changes, ventricular arrhythmias, and sudden cardiac arrest have been reported with cocaine exposure.37
Cocaine and Sudden Arrhythmic Deaths:
Evidence regarding cocaine abuse and SCD stems primarily from autopsy studies. An Australian study48 examined autopsy cases of sudden and unexpected death where cocaine or its metabolites were detected for case circumstances, pathology, toxicology, and coronial findings. The concentration of cocaine was low in 44% deemed to have died from cocaine cardiotoxicity (median age 30, mostly men). Multiple drug use was found with opioids (47%), amphetamines (31%), and ethanol (35%). Coexistent heart disease was present in 31%, with coronary artery disease being most common (73%). Cardiomegaly was present in 33% of cases.48
Another study of 668 SCD patients found 3.1% to be cocaine-related, most with concomitant ethanol use49. Recent cocaine use was significantly associated with an increased risk of SCD due to cardiovascular causes in individuals aged 15–49 years.50 In a pooled autopsy report summarizing 4 studies, only 23 (22%) had coronary artery disease out of 107 deaths related to cocaine. No definitive findings could explain the cause of death in most patients, suggesting an arrhythmia-related SCD.44 In a single-center retrospective study (n=2,578) comparing heart failure patients with and without HIV, cocaine use predicted a 3-fold increase in SCD in patients with HIV, compared to those without HIV.51
Treatment of Arrhythmias in Patients with Cocaine use:
Treatment of cocaine-induced cardiac arrhythmias is multifaceted. General medical conditions, ischemia and hemodynamics of the patient need to be addressed. Treatment of cocaine-induced excitability to stop the catecholaminergic surge and sympathetic tone, could have positive benefit.31 Aside from a baseline EKG and cardiac monitoring,52 electrolyte abnormalities, especially hypokalemia and hypomagnesemia, must be corrected to prevent QT-prolonging and arrhythmogenic effects.
Beta-blocker use in patients with cocaine-induced chest pain and arrhythmias is controversial. Experimental studies and some case reports indicate that beta-blocker use can lead to unopposed alpha-adrenergic actions of cocaine producing severe hypertension, coronary vasospasm, and death. However, a recent meta-analysis reported no difference in outcomes in active cocaine users started on a beta-blocker to treat hypertension, chest pain or tachycardia vs those who were not.53 The authors concluded unopposed alpha-agonistic actions are probably very rare and likely due to myriad effects of cocaine itself rather than concomitant beta-blocker use.54 Use of non- labetalol and carvedilol may be preferred as they can act as alpha blockers as well.54
Prazosin, an alpha-adrenergic receptor antagonist can reduce VF in a cocaine and MI dog model55 but no clinical evidence supports benefit in humans. Calcium-channel blockers can be used safely in cocaine toxicity, although studies show that these drugs do not reduce tachycardia in cocaine users.56 Amiodarone has not been tested for cocaine-induced arrhythmias in humans. Procainamide can inhibit human plasma butyrylcholinesterase, an enzyme essential in the metabolic degradation of cocaine. Although interactions between cocaine and procainamide in the clinical setting has not been well studied, in-vitro studies of these two compounds in pooled human serum samples demonstrated that procainamide profoundly inhibited cocaine and cocaethylene degradation.57
Many cocaine-induced arrhythmias, especially those occurring immediately after cocaine use, are thought to be due to sodium blockade. Translational studies suggest sodium bicarbonate is an antidote for cocaine’s sodium blockade effects based on its ability to reverse QRS prolongation in dog models.58 Case reports show that cocaine toxicity-induced wide-complex tachycardia mimicking flecainide toxicity can be reversed by sodium bicarbonate.32 Sodium bicarbonate has also been cited as the preferred drug of choice for cocaine induced VT by the AHA scientific statement from the Acute Care Committee of the Council of Cardiology.59
However, use of lidocaine to treat cocaine-induced arrhythmias is controversial. Lidocaine can directly inhibit binding of cocaine to sodium channels and shift the concentration-effect curve rightward in animal studies,60,61. The dose of lidocaine required for such effects may be well above that used clinically.62 Lidocaine can reduce seizure threshold and produce increased seizure risk in cocaine-treated animals63. Despite these findings, a study of 29 patients reported that patients hospitalized with cocaine-related MI treated with lidocaine had no seizures64. Another study compared the effects of lidocaine versus sodium bicarbonate in ex-vivo guinea pig hearts exposed to cocaine and found that both were equally effective in reducing cocaine-induced QRS prolongation65.
Finally, monoamine neurotransmitter receptor antagonists, specifically dopamine type 1 receptor antagonists66 and serotonin type 4 receptor antagonists67 have been shown in animal models to reverse cocaine-associated cardiac arrhythmias; however, these drugs have not yet advanced to studies in humans. In contrast to cardiac arrhythmias occurring immediately after cocaine use, thought to be due to direct cardiotoxicity and ion channel actions, ventricular arrhythmias appearing several hours later are predominantly secondary to ischemia.59
SUBSTITUTED AMPHETAMINES:
Substituted amphetamines and Electrical Remodeling:
Methamphetamine can remodel ion channels directly. In-vitro treatment of rat ventricular myocytes with methamphetamine resulted in inhibition of transient outward potassium current (Kto), and inward rectifying potassium current (Kir).68 While actions of methamphetamine on potassium channels are clear, effects on calcium channels are more controversial. Methamphetamine exposure to neonatal rat ventricular myocytes increased intracellular calcium oscillations, cardiomyocyte beating rates, and calcium entry through L-type calcium channels.69 However, methamphetamine can inhibit L-type calcium currents,68 by shifting the recovery curve downwards, making it longer for the channel to recover from inactivation for similar calcium concentrations without altering steady-state activation or inactivation curves of the channel.
Besides altering functions of ion channels, methamphetamine reduced transcription of ion channels. Expression of mRNA and protein levels of CACNA1C, CACNB2, KCNA4, KCNA7, KCNC4, KCND2, KCNJ2, KCNJ12, KCNJ4, and KCNJ14 were reduced in vitro and in vivo following methamphetamine exposure. Changes in ion channel expression reversed with methamphetamine withdrawal70. Methamphetamine can also produce epigenetic DNA methylation, thereby, increasing transcription and translation of L-type calcium channels in animal models of HIV infection, a finding of potential significance in the HIV population that is known to have an increased prevalence of stimulant drug use71.
Amphetamine-derived stimulants, including MDMA, can increase field potential duration of human inducible stem cell-derived cardiomyocytes in a concentration-dependent manner20. In addition, a single dose of MDMA can decrease connexin 43 expression in animal models, leading to a reduction in N-cadherin, and altered calcium oscillation patterns72.
Substituted amphetamines and Structural Remodeling:
Toxicities associated with methamphetamine use include: hypertension, arrhythmias, coronary vasospasm, myocardial infarction, and cardiomyopathy73. Evidence from clinical case studies of methamphetamine users demonstrated reduced left ventricular ejection fraction, left ventricular chamber dilatation, myocardial lesions, cardiac hypertrophy, fibrosis, and inflammation in younger patients (age ≤50) even without cardiac risk factors74,75. Severe left ventricular ejection fraction attenuation with chamber dilatation can occur in methamphetamine users75,76. A routine screening of >4000 patients positive for methamphetamine showed heart failure in 18% patients; >10% patients had abnormal brain natriuretic peptide (BNP) levels77. Autopsies of patients using methamphetamine showed increased collagen deposition and fibrotic remodeling in the perivascular and interstitial spaces of the heart78.
In pre-clinical rodent models, acute and chronic methamphetamine-mediated cardiomyopathy has been reported.79,80 A common methamphetamine use pattern is ‘binge and crash’; such patients tend to take approximately 1.5 times more drugs/month than chronic users.81 A recent study showed that ‘binge and crash’ methamphetamine administration in mice resulted in cardiac hypertrophy, fibrotic remodeling, and mitochondrial dysfunction leading to contractile dysfunction.78 Pre-clinical studies to determine molecular signaling mediating methamphetamine toxicity point to Sigmar1 as a target. Cardiomyopathy associated with methamphetamine in mice resulted from Sigmar1 inhibition by methamphetamine, resulting in alteration of mitochondrial dynamics and function78. In addition, methamphetamine causes increased oxidative stress, altered intracellular calcium dynamics, enhanced inflammatory markers, and reduced cardiac contractility10,82.
Substituted amphetamines and EKG changes:
In a retrospective cohort study, only 28.3% of methamphetamine users had a normal EKG. Tachyarrhythmias, right axis deviation, left ventricular hypertrophy, P-pulmonale pattern, inferior Q waves, lateral T-wave inversion, and prolonged QTc interval were common findings in the methamphetamine group. QTc >440 ms (Table 3) was observed in 27.2% of patients, 83,84. Emergency department data showed sinus tachycardia to be the predominant tachyarrhythmia in methamphetamine admissions.85 Methamphetamine-induced myocardial ischemia evident by EKG changes have been reported; in a retrospective analysis of 627 EKGs of patients using methamphetamine, 6.5% showed evidence of MI.86 MDMA caused sinus tachycardia, hypertension, hyperthermia, and vasospasm.87 Further, MDMA can cause MI and associated EKG changes. MDMA use has been associated with ST-elevation and non-ST elevation MI in case reports.88
Substituted Amphetamines and Bradyarrhythmias:
Bradyarrhythmias have not been associated with methamphetamine.83,84 Decreased heart-rate variability (HRV) in chronic methamphetamine users suggests autonomic nervous system dysfunction.89 HRV and parasympathetic cardiovascular tone were decreased in repeat MDMA users versus non-users.90
Substituted Amphetamines and Atrial Arrhythmias:
Active methamphetamine users have increased left atrial size vs non-users or those who have discontinued methamphetamine74,91 increasing the risk of atrial arrhythmias, specifically, atrial fibrillation.92 Similarly, a small, prospective, study using ambulatory monitors found atrial ectopy and atrial tachycardia during cocaine use in 6/7 hypertensive cocaine users.46 A retrospective study with >11,000 heart failure patients (5% methamphetamine users, 0.6% cocaine users) found an increased incidence of atrial fibrillation and flutter in substance users vs non-users.93
Methamphetamine-associated cardiomyopathy may increase the risk of atrial arrhythmias in methamphetamine users. In a retrospective study of 296 patients with methamphetamine-induced cardiomyopathy and 356 with methamphetamine use but no cardiomyopathy, atrial fibrillation was much more prevalent in cardiomyopathy patients with methamphetamine use.75 Another study with >20,000 patients confirmed these findings, showing that the odds of atrial fibrillation associated with heart failure in methamphetamine users was significantly higher (OR: 27.4, 95% CI: 15.8–47.5).
However, patients with methamphetamine-associated cardiomyopathy were less likely to have atrial fibrillation vs those with cardiomyopathy due to other causes (adjusting for comorbidities)94. This inverse association between atrial fibrillation and methamphetamine use in cardiomyopathy patients was corroborated by a large Veterans Administration study. Patients with methamphetamine-associated cardiomyopathy, however, were approximately 10-years younger.95 Although MDMA has been reported to cause atrial fibrillation in isolated case reports, systematic reporting of any association is lacking.96
Substituted Amphetamines and Ventricular Arrhythmias
Although studies have documented a higher incidence of SCD in people using methamphetamine, evidence for ventricular arrhythmias in the clinical setting is lacking. Case reports have documented monomorphic VT,97 polymorphic VT,98 and VF99 with methamphetamine use. A study of 230 patients presenting to the emergency department with methamphetamine use showed that ~6% had cardiac arrhythmias, including ventricular tachycardia and frequent PVCs.100
A longitudinal study of 1,315 inpatient methamphetamine users and >5,000 control patients, followed for 10 years, found twice the incidence of “cardiac arrhythmias” in methamphetamine users vs controls. However, any arrhythmia diagnosis was not made clear.101 Recently an analysis of the United States National Inpatient Sample database showed that patients admitted with acute heart failure and stimulant use (cocaine and/or amphetamines) had a significantly higher risk of ventricular tachycardia vs. acute heart failure patients without co-existent stimulant use.102
Although methamphetamine use patients admitted with heart failure had almost twice the rate of in-hospital mortality as cocaine use (1.4% vs 0.7%), ventricular arrhythmias were just slightly higher in the cocaine use patients compared to methamphetamine use patients (7.8% versus 7.2%). A comparison of methamphetamine and cocaine related arrhythmias based on real life reporting to Federal Adverse Event Reporting System (FAERS) database was performed and reported under the section on stimulant use with cocaine and methamphetamine: a pharmacovigilance analysis in the supplementary material.
Substituted Amphetamines and Sudden Arrhythmic Deaths:
Methamphetamine and MDMA use increase risk of SCD in patients with pre-excitation syndromes103 and in patients with various cardiovascular diseases based on case reports.104 MDMA has been reported to provoke SCD in patients with channelopathies98 and electrical storm as a result of serotonin syndrome.105 Prescription amphetamine use has not been associated with SCD in children,106 and adults.107
In a study involving 100 autopsies108 of individuals testing positive for methamphetamine, moderate-to-severe atherosclerosis was found in only 17%. Direct methamphetamine toxicity, with no other identifiable cause of death, was the attributed cause of death in 68%, suggesting arrhythmias as a factor. Myocardial fiber hypertrophy and focal myocardial necrosis were observed in many of these individuals.108 A retrospective study of 1,649 Australian patients who died with known toxicology positive for methamphetamine showed that 3.7% of patients died most likely from arrhythmic causes.109 Like cocaine, a large majority of methamphetamine users in autopsy series of SCD had well below toxic levels of the drug.110
Treatment of Arrhythmias in Patients with Substituted amphetamines use:
Treatment options for methamphetamine-induced cardiac arrhythmias have to be weighed against negative inotropic effects of the drug as many patients with methamphetamine use have co-existent methamphetamine-induced cardiomyopathy. Unlike cocaine, there is no specific contraindication, or controversy, surrounding use of beta-blockers in methamphetamine patients with cardiac arrhythmias. Selective and non-selective beta-blockers can be used with slow titration, especially in patients with methamphetamine-induced cardiomyopathy, to treat methamphetamine-related cardiac arrhythmias.111 One of the few randomized studies testing beta-blockers in MDMA users found no adverse effects and effective antihypertensive and anti-tachycardic effect when using the combined alpha and beta antagonist carvedilol in patients taking MDMA.112
Benzodiazepines may be useful to treat methamphetamine-induced cardiac arrhythmias by mitigating agitation and sympathetic tone.113 If supplementary antipsychotic agents are needed in the care of patients with methamphetamine-induced arrhythmias, shorter acting drugs like droperidol may be preferred over haloperidol and should always be coupled with close monitoring of QTC interval. Electrical storms due to MDMA-induced serotonin syndrome can be treated by treating hyperthermia, managing autonomic instability, and serotonin antagonism.105 Extra-corporeal life support has been previously used for recurrent and refractory electrical storms caused by substituted amphetamines.105
The Ethics of Defibrillator Use in Patients with Stimulant Use Disorder and Risk of Sudden Cardiac Death:
Patients with stimulant substance use and non-ischemic cardiomyopathy have high likelihood of having substance-induced cardiomyopathy. As abstinence could lead to recovery of cardiac function, efforts and resources should be dedicated to promoting abstinence and recovery (please refer to section on multidisciplinary team approach to stimulant use in the supplementary material). This is particularly true in patients with stimulant substance use as they may be using multiple substances, that each individually increase the risk of cardiomyopathy.
Cardiac MRI can be used as an adjunctive tool to predict recovery from stimulant drug-induced cardiomyopathy and therefore in the decision of implantable cardioverter defibrillator (ICD) implant for primary prevention.114 While a majority of patients with stimulant-related cardiomyopathy are prescribed goal-directed medical therapy, only 14%−33% underwent an ICD implant.74,75
Reasons for this are multifold: 1) Patients with methamphetamine-related cardiomyopathy often abuse other substances and lack insight into their illness and treatment options, 2) Patients with methamphetamine use often have co-occurring psychiatric illnesses115 making them unreliable for follow-up after ICD implantation, 3) Methamphetamine users may be homeless and lack social support, making it difficult to attend device clinics.
A large proportion of heart failure patients with comorbid stimulant use leave care against medical advice (7.8% vs. 1.1% in acute heart failure admissions without stimulant use),102 raising questions about their ability to follow through with the plan of care and follow-up appointments. Unfortunately, issues with compliance can set them up for increased complications or risk that the complications will go undetected, such as pocket infection, lead malfunction, or battery depletion.
Another factor that adds to reservations of ICD implantation in active substance abusers is risk of lead endocarditis in case of intravenous drug abuse. In the spirit of “primum non nocere,” first, do no harm, a most pressing concern is the risk of inappropriate shocks due to sinus tachycardia or supraventricular tachycardia triggered by active substance use. In a retrospective study of 326 patients with ICDs, with and without HIV, cocaine use was positively associated with risk of ICD therapies, approximately half of which were inappropriate. Not surprisingly, a retrospective study evaluating characteristic features of patients with phantom shocks found an association between phantom shocks, previous electrical storms and cocaine use.116
Increased defibrillation thresholds in active stimulant substance users is a concern that makes ICD therapy potentially futile or increases the risk of repeated shocks, making the decision to implant an ICD more complicated. Compared to age and sex-matched controls, methamphetamine-associated cardiomyopathy patients receiving ICDs had a defibrillation threshold almost 10 Joules higher.117 Similarly, studies comparing chronic cocaine users to control patients showed up to 13 joules higher defibrillation threshold in cocaine users receiving ICDs.118,119
We observed a direct time-dependent correlation between cocaine use and failed ICD therapies. A 36-year-old patient with ischemic cardiomyopathy and ICD implantation 6 years ago was admitted with VT/VF storm and multiple ICD shocks, including multiple failed shocks 16 hours after cocaine use with no evidence of ischemia. Defibrillation threshold testing 4 days later showed successful defibrillation at approximately half the energy of the therapies that failed during active cocaine use. Importantly, no studies show that ICDs reduce risk of sudden death or total mortality in stimulant users with or without cardiomyopathy and for primary or secondary prevention with or without other established cardiovascular disease.
Unanswered questions and future research
While there is a large body of literature related to mechanisms, prevalence, and treatment of cardiac arrhythmias in stimulant drug users, there are significant deficits in the current knowledge. Table 4 summarizes the gaps in understanding and possible avenues for new research.
Table 4:
Current knowledge, gaps in understanding and avenues of new research in stimulant use related cardiac arrhythmias
| Current Knowledge | Unanswered Questions | New areas of Research |
|---|---|---|
| Stimulant drugs alter expression and gating properties of multiple ion channels and calcium handling proteins affecting the ventricular myocyte action potential | Is there a cause-and-effect relationship between stimulant drugs and cardiac arrhythmias? Does electrical remodeling caused by stimulant drugs translate or lead to ventricular arrhythmias at the level of the organ or the organism? |
In-vivo and ex-vivo animal models of stimulant use and cardiac arrhythmias |
| Stimulant drugs cause multiple EKG changes including QT prolongation, QRS prolongation, early repolarization and ST changes | Are the EKG changes induced by stimulant drugs dose dependent and/or affected by presence of other stimulant and non-stimulant drugs of abuse and/or affected by other comorbidities? | Cohort or retrospective human studies and animal studies focusing on EKG changes with stimulant drug use with emphasis on dose response, co-existent drugs of abuse and comorbidities |
| Stimulant drugs are associated with increased atrial and ventricular arrhythmias based on retrospective studies | The exact incidence and prevalence of atrial and ventricular arrhythmias in subjects using stimulant drugs is currently unknown | Systematic prospective continuous cardiac monitoring of stimulant drug users to evaluate incidence and prevalence of atrial and ventricular arrhythmias |
| Current treatment of stimulant drug induced arrhythmias is based on anecdotal evidence, retrospective studies and small randomized control studies | What is the safety and efficacy of drugs including beta-blockers, calcium channel blockers and antiarrhythmic drugs in stimulant drug induced cardiac arrhythmias? | Randomized controlled trials of selective and non-selective beta-blockers, alpha-blockers, calcium channel blockers and antiarrhythmic drugs in the treatment of stimulant drug induced cardiac arrhythmias |
| Active stimulant drug use alters defibrillation thresholds. Stimulant drug users have poor compliance and follow up after ICD placement for primary/secondary prevention of SCD | What is the safety and efficacy of ICDs in patients with a history of stimulant drug use for primary or secondary prevention of SCD? | Randomized controlled trials or retrospective review focusing on the benefit of ICD in patients with history of stimulant drug use |
Conclusions:
Cocaine and methamphetamine cause structural and electrical remodeling of the atria and ventricles with subsequent EKG changes and ensuing atrial and ventricular arrhythmias. Mechanisms behind, and the true incidence of, stimulant drug-induced cardiac arrhythmias need further investigation. Treatment of stimulant drug-induced cardiac arrhythmias based on general principles of cardiac rhythm management, experience from stimulant drug toxicities and case reports, requires further refinement by larger clinical studies and/or observations. A multidisciplinary approach to the treatment of patients with stimulant use disorder will heighten success rates. ICD use in patients with stimulant drug use remains controversial.
Supplementary Material
Funding:
This publication was supported by an Institutional Development Award from the National Institutes of General Medical Sciences of the National Institutes of Health (NIH) under grant number P20GM121307 to C.G. Kevil, and by R01HL145753, R01HL145753–01S1, R01HL145753–03S1, LSUHSC-S CCDS Finish Line Award, and LSUHSC-S LARC Research Awards to M. S. B
Abbreviations:
- ADHD
Attention deficit hyperactivity disorder
- MDMA
3,4-methylenedioxy-methamphetamine
- CNS
Central nervous system
- DAT
Dopamine transporter
- KATP
ATP-sensitive potassium channel
- IKr
inward rectifying potassium channel
- APD
action potential duration
- CaMKII
Calcium calmodulin kinase II
- Kto
Transient outward potassium channel
- HIV
Human immunodeficiency virus
- MI
Myocardial Infarction
- BNP
Brain natriuretic peptide
- cAMP
Cyclic adenosine monophosphate
- VF
Ventricular fibrillation
- VT
Ventricular tachycardia
- SCD
Sudden cardiac death
- HRV
Heart rate variability
- PVC
Premature ventricular contraction
- CP
Chest pain
- FAERS
FDA’s adverse event reporting system
- PRR
Proportional reporting ratio
- HTN
Hypertension
- ICD
Implantable cardioverter-defibrillator
Footnotes
Disclosures: All authors in this study declare no conflicts of interest.
Supplemental Materials:
I. Stimulant Misuse and Co-occurring Risk Factors for Arrhythmias
II. Stimulant Use with Cocaine and Methamphetamine: A Pharmacovigilance Analysis
III. Multidisciplinary Team Approach to Stimulant Use
References:
- 1.World Drug Report 2020 [Internet]. United Nations : World Drug Report 2020. [cited 2021 Feb 19];Available from: //wdr.unodc.org/wdr2020/en/index.html [Google Scholar]
- 2.Howell LL, Kimmel HL. Monoamine transporters and psychostimulant addiction. Biochem Pharmacol. 2008;75:196–217. [DOI] [PubMed] [Google Scholar]
- 3.Reith ME, Meisler BE, Sershen H, Lajtha A. Structural requirements for cocaine congeners to interact with dopamine and serotonin uptake sites in mouse brain and to induce stereotyped behavior. Biochem Pharmacol. 1986;35:1123–1129. [DOI] [PubMed] [Google Scholar]
- 4.Ritz MC, Lamb RJ, Goldberg SR, Kuhar MJ. Cocaine receptors on dopamine transporters are related to self-administration of cocaine. Science. 1987;237:1219–1223. [DOI] [PubMed] [Google Scholar]
- 5.Volkow ND, Wang GJ, Fischman MW, Foltin RW, Fowler JS, Abumrad NN, Vitkun S, Logan J, Gatley SJ, Pappas N, et al. Relationship between subjective effects of cocaine and dopamine transporter occupancy. Nature. 1997;386:827–830. [DOI] [PubMed] [Google Scholar]
- 6.Volkow ND, Wang GJ, Fowler JS, Gatley SJ, Logan J, Ding YS, Dewey SL, Hitzemann R, Gifford AN, Pappas NR. Blockade of striatal dopamine transporters by intravenous methylphenidate is not sufficient to induce self-reports of “high.” J Pharmacol Exp Ther. 1999;288:14–20. [PubMed] [Google Scholar]
- 7.Wu S-N, Chang H-D, Sung RJ. Cocaine-induced inhibition of ATP-sensitive K+ channels in rat ventricular myocytes and in heart-derived H9c2 cells. Basic Clin Pharmacol Toxicol. 2006;98:510–517. [DOI] [PubMed] [Google Scholar]
- 8.Reyes S, Kane GC, Zingman LV, Yamada S, Terzic A. Targeted disruption of K(ATP) channels aggravates cardiac toxicity in cocaine abuse. Clin Transl Sci. 2009;2:361–365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.O’Leary ME. Inhibition of HERG potassium channels by cocaethylene: a metabolite of cocaine and ethanol. Cardiovasc Res. 2002;53:59–67. [DOI] [PubMed] [Google Scholar]
- 10.Xiao Y-F, Ke Q, Wang S-Y, Yang Y, Chen Y, Wang GK, Morgan JP, Cox B, Leaf A. Electrophysiologic properties of lidocaine, cocaine, and n-3 fatty-acids block of cardiac Na+ channels. Eur J Pharmacol. 2004;485:31–41. [DOI] [PubMed] [Google Scholar]
- 11.Crumb WJ, Clarkson CW. Characterization of cocaine-induced block of cardiac sodium channels. Biophys J. 1990;57:589–599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.O’Leary ME, Chahine M. Cocaine binds to a common site on open and inactivated human heart (Na(v)1.5) sodium channels. J Physiol. 2002;541:701–716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.O’Leary ME, Digregorio M, Chahine M. Closing and inactivation potentiate the cocaethylene inhibition of cardiac sodium channels by distinct mechanisms. Mol Pharmacol. 2003;64:1575–1585. [DOI] [PubMed] [Google Scholar]
- 14.Tsushima RG, Kelly JE, Wasserstrom JA. Characteristics of cocaine block of purified cardiac sarcoplasmic reticulum calcium release channels. Biophys J. 1996;70:1263–1274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Renard DC, Delaville FJ, Thomas AP. Inhibitory effects of cocaine on Ca2+ transients and contraction in single cardiomyocytes. Am J Physiol. 1994;266:H555–567. [DOI] [PubMed] [Google Scholar]
- 16.Nicolás JM, Rubin E, Thomas AP. Ethanol and cocaine cause additive inhibitory effects on the calcium transients and contraction in single cardiomyocytes. Alcohol Clin Exp Res. 1996;20:1077–1082. [DOI] [PubMed] [Google Scholar]
- 17.Sanchez EJ, Hayes RP, Barr JT, Lewis KM, Webb BN, Subramanian AK, Nissen MS, Jones JP, Shelden EA, Sorg BA, et al. Potential role of cardiac calsequestrin in the lethal arrhythmic effects of cocaine. Drug Alcohol Depend. 2013;133:344–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Henning RJ, Cuevas J. Cocaine activates calcium/calmodulin kinase II and causes cardiomyocyte hypertrophy. J Cardiovasc Pharmacol. 2006;48:802–813. [DOI] [PubMed] [Google Scholar]
- 19.Kimura S, Bassett AL, Xi H, Myerburg RJ. Early afterdepolarizations and triggered activity induced by cocaine. A possible mechanism of cocaine arrhythmogenesis. Circulation. 1992;85:2227–2235. [DOI] [PubMed] [Google Scholar]
- 20.Zwartsen A, de Korte T, Nacken P, de Lange DW, Westerink RHS, Hondebrink L. Cardiotoxicity screening of illicit drugs and new psychoactive substances (NPS) in human iPSC-derived cardiomyocytes using microelectrode array (MEA) recordings. J Mol Cell Cardiol. 2019;136:102–112. [DOI] [PubMed] [Google Scholar]
- 21.Brickner ME, Willard JE, Eichhorn EJ, Black J, Grayburn PA. Left ventricular hypertrophy associated with chronic cocaine abuse. Circulation. 1991;84:1130–1135. [DOI] [PubMed] [Google Scholar]
- 22.Mittleman MA, Mintzer D, Maclure M, Tofler GH, Sherwood JB, Muller JE. Triggering of myocardial infarction by cocaine. Circulation. 1999;99:2737–2741. [DOI] [PubMed] [Google Scholar]
- 23.Schwartz BG, Rezkalla S, Kloner RA. Cardiovascular effects of cocaine. Circulation. 2010;122:2558–2569. [DOI] [PubMed] [Google Scholar]
- 24.Lange RA, Hillis LD. Cardiovascular complications of cocaine use. N Engl J Med. 2001;345:351–358. [DOI] [PubMed] [Google Scholar]
- 25.Qureshi AI, Suri MF, Guterman LR, Hopkins LN. Cocaine use and the likelihood of nonfatal myocardial infarction and stroke: data from the Third National Health and Nutrition Examination Survey. Circulation. 2001;103:502–506. [DOI] [PubMed] [Google Scholar]
- 26.Tazelaar HD, Karch SB, Stephens BG, Billingham ME. Cocaine and the heart. Hum Pathol. 1987;18:195–199. [DOI] [PubMed] [Google Scholar]
- 27.Lattanzio FA, Tiangco D, Osgood C, Beebe S, Kerry J, Hargrave BY. Cocaine increases intracellular calcium and reactive oxygen species, depolarizes mitochondria, and activates genes associated with heart failure and remodeling. Cardiovasc Toxicol. 2005;5:377–390. [DOI] [PubMed] [Google Scholar]
- 28.Gardin JM, Wong N, Alker K, Hale SL, Paynter J, Knoll M, Jamison B, Patterson M, Kloner RA. Acute cocaine administration induces ventricular regional wall motion and ultrastructural abnormalities in an anesthetized rabbit model. Am Heart J. 1994;128:1117–1129. [DOI] [PubMed] [Google Scholar]
- 29.Sutliff RL, Haase C, Russ R, Hoit BD, Morris R, Norman AB, Lewis W. Cocaine increases mortality and cardiac mass in a murine transgenic model of acquired immune deficiency syndrome. Lab Invest. 2003;83:983–989. [DOI] [PubMed] [Google Scholar]
- 30.Gamouras GA, Monir G, Plunkitt K, Gursoy S, Dreifus LS. Cocaine abuse: repolarization abnormalities and ventricular arrhythmias. Am J Med Sci. 2000;320:9–12. [DOI] [PubMed] [Google Scholar]
- 31.Hoffman RS. Treatment of patients with cocaine-induced arrhythmias: bringing the bench to the bedside. Br J Clin Pharmacol. 2010;69:448–457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sharma J, Rathnayaka N, Green C, Moeller FG, Schmitz JM, Shoham D, Dougherty AH. Bradycardia as a Marker of Chronic Cocaine Use: A Novel Cardiovascular Finding. Behav Med. 2016;42:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Liaudet L, Calderari B, Pacher P. Pathophysiological mechanisms of catecholamine and cocaine-mediated cardiotoxicity. Heart Fail Rev. 2014;19:815–824. [DOI] [PubMed] [Google Scholar]
- 34.Egred M, Davis GK. Cocaine and the heart. Postgrad Med J. 2005;81:568–571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Gatto L, Frati G, Biondi-Zoccai G, Versaci F. Cocaine and acute coronary syndromes: Novel management insights for this clinical conundrum. Int J Cardiol. 2018;260:16–17. [DOI] [PubMed] [Google Scholar]
- 36.Al-Sadawi M, Alkhawam H, Hartt A, Soleiman A, McFarlane SI. Cocaine-Induced Brugada Pattern. Am J Med Case Rep. 2019;7:59–61.31396550 [Google Scholar]
- 37.Bebarta VS, Summers S. Brugada electrocardiographic pattern induced by cocaine toxicity. Ann Emerg Med. 2007;49:827–829. [DOI] [PubMed] [Google Scholar]
- 38.Om A, Ellenbogen KA, Vetrovec GW. Cocaine-induced bradyarrhythmias. Am Heart J. 1992;124:232–234. [DOI] [PubMed] [Google Scholar]
- 39.Kariyanna PT, Jayarangaiah A, Al-Sadawi M, Ahmed R, Green J, Dubson I, McFarlane SI. A Rare Case of Second Degree Mobitz Type II AV Block Associated with Cocaine Use. Am J Med Case Rep. 2018;6:146–148.30294672 [Google Scholar]
- 40.Clarkson CW, Chang C, Stolfi A, George WJ, Yamasaki S, Pickoff AS. Electrophysiological effects of high cocaine concentrations on intact canine heart. Evidence for modulation by both heart rate and autonomic nervous system. Circulation. 1993;87:950–962. [DOI] [PubMed] [Google Scholar]
- 41.Franklin SM, Thihalolipavan S, Fontaine JM. Sinus Bradycardia in Habitual Cocaine Users. Am J Cardiol. 2017;119:1611–1615. [DOI] [PubMed] [Google Scholar]
- 42.Gad A, Morelli P, Decristofaro J. Perinatal isolated atrial flutter associated with maternal cocaine and opiate use in a late preterm infant. J Matern Fetal Neonatal Med. 2010;23:1062–1065. [DOI] [PubMed] [Google Scholar]
- 43.Ouali S, Guermazi O, Ben Halima M, Boudiche S, Khedher N, Adeljalil F, Meghaeith F, Larbi N, Mourali MS. Ventricular tachycardia revealing drug abuse induced myocarditis: two case reports. Clin Case Rep. 2018;6:1225–1229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Bauman JL, Grawe JJ, Winecoff AP, Hariman RJ. Cocaine-related sudden cardiac death: a hypothesis correlating basic science and clinical observations. J Clin Pharmacol. 1994;34:902–911. [DOI] [PubMed] [Google Scholar]
- 45.Billman GE, Hoskins RS. Cocaine-induced ventricular fibrillation: protection afforded by the calcium antagonist verapamil. FASEB J. 1988;2:2990–2995. [DOI] [PubMed] [Google Scholar]
- 46.Secemsky E, Lange D, Waters DD, Goldschlager NF, Hsue PY. Hemodynamic and arrhythmogenic effects of cocaine in hypertensive individuals. J Clin Hypertens (Greenwich). 2011;13:744–749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hollander JE, Hoffman RS, Burstein JL, Shih RD, Thode HC. Cocaine-associated myocardial infarction. Mortality and complications. Cocaine-Associated Myocardial Infarction Study Group. Arch Intern Med. 1995;155:1081–1086. [PubMed] [Google Scholar]
- 48.Pilgrim JL, Woodford N, Drummer OH. Cocaine in sudden and unexpected death: a review of 49 post-mortem cases. Forensic Sci Int. 2013;227:52–59. [DOI] [PubMed] [Google Scholar]
- 49.Lucena J, Blanco M, Jurado C, Rico A, Salguero M, Vazquez R, Thiene G, Basso C. Cocaine-related sudden death: a prospective investigation in south-west Spain. Eur Heart J. 2010;31:318–329. [DOI] [PubMed] [Google Scholar]
- 50.Morentin B, Ballesteros J, Callado LF, Meana JJ. Recent cocaine use is a significant risk factor for sudden cardiovascular death in 15–49-year-old subjects: a forensic case-control study. Addiction. 2014;109:2071–2078. [DOI] [PubMed] [Google Scholar]
- 51.Alvi RM, Neilan AM, Tariq N, Hassan MO, Awadalla M, Zhang L, Afshar M, Rokicki A, Mulligan CP, Triant VA, et al. The Risk for Sudden Cardiac Death Among Patients Living With Heart Failure and Human Immunodeficiency Virus. JACC Heart Fail. 2019;7:759–767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Sandau KE, Funk M, Auerbach A, Barsness GW, Blum K, Cvach M, Lampert R, May JL, McDaniel GM, Perez MV, et al. , American Heart Association Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; and Council on Cardiovascular Disease in the Young. Update to Practice Standards for Electrocardiographic Monitoring in Hospital Settings: A Scientific Statement From the American Heart Association. Circulation. 2017;136:e273–e344. [DOI] [PubMed] [Google Scholar]
- 53.Lo KB, Virk HUH, Lakhter V, Ram P, Gongora C, Pressman G, Figueredo V. Clinical Outcomes After Treatment of Cocaine-Induced Chest Pain with Beta-Blockers: A Systematic Review and Meta-Analysis. Am J Med. 2019;132:505–509. [DOI] [PubMed] [Google Scholar]
- 54.Richards JR, Hollander JE, Ramoska EA, Fareed FN, Sand IC, Izquierdo Gómez MM, Lange RA. β-Blockers, Cocaine, and the Unopposed α-Stimulation Phenomenon. J Cardiovasc Pharmacol Ther. 2017;22:239–249. [DOI] [PubMed] [Google Scholar]
- 55.Billman GE. The effect of adrenergic receptor antagonists on cocaine-induced ventricular fibrillation: alpha but not beta adrenergic receptor antagonists prevent malignant arrhythmias independent of heart rate. J Pharmacol Exp Ther. 1994;269:409–416. [PubMed] [Google Scholar]
- 56.Richards JR, Garber D, Laurin EG, Albertson TE, Derlet RW, Amsterdam EA, Olson KR, Ramoska EA, Lange RA. Treatment of cocaine cardiovascular toxicity: a systematic review. Clin Toxicol (Phila). 2016;54:345–364. [DOI] [PubMed] [Google Scholar]
- 57.Bailey DN. Amitriptyline and procainamide inhibition of cocaine and cocaethylene degradation in human serum in vitro. J Anal Toxicol. 1999;23:99–102. [DOI] [PubMed] [Google Scholar]
- 58.Beckman KJ, Parker RB, Hariman RJ, Gallastegui JL, Javaid JI, Bauman JL. Hemodynamic and electrophysiological actions of cocaine. Effects of sodium bicarbonate as an antidote in dogs. Circulation. 1991;83:1799–1807. [DOI] [PubMed] [Google Scholar]
- 59.McCord J, Jneid H, Hollander JE, de Lemos JA, Cercek B, Hsue P, Gibler WB, Ohman EM, Drew B, Philippides G, et al. , American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Management of cocaine-associated chest pain and myocardial infarction: a scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Circulation. 2008;117:1897–1907. [DOI] [PubMed] [Google Scholar]
- 60.Grawe JJ, Hariman RJ, Winecoff AP, Fischer JH, Bauman JL. Reversal of the electrocardiographic effects of cocaine by lidocaine. Part 2. Concentration-effect relationships. Pharmacotherapy. 1994;14:704–711. [PubMed] [Google Scholar]
- 61.Liu D, Hariman RJ, Bauman JL. Cocaine concentration-effect relationship in the presence and absence of lidocaine: evidence of competitive binding between cocaine and lidocaine. J Pharmacol Exp Ther. 1996;276:568–577. [PubMed] [Google Scholar]
- 62.Hondeghem LM, Katzung BG. Antiarrhythmic agents: the modulated receptor mechanism of action of sodium and calcium channel-blocking drugs. Annu Rev Pharmacol Toxicol. 1984;24:387–423. [DOI] [PubMed] [Google Scholar]
- 63.Derlet RW, Albertson TE, Tharratt RS. Lidocaine potentiation of cocaine toxicity. Ann Emerg Med. 1991;20:135–138. [DOI] [PubMed] [Google Scholar]
- 64.Shih RD, Hollander JE, Burstein JL, Nelson LS, Hoffman RS, Quick AM. Clinical safety of lidocaine in patients with cocaine-associated myocardial infarction. Ann Emerg Med. 1995;26:702–706. [DOI] [PubMed] [Google Scholar]
- 65.Winecoff AP, Hariman RJ, Grawe JJ, Wang Y, Bauman JL. Reversal of the electrocardiographic effects of cocaine by lidocaine. Part 1. Comparison with sodium bicarbonate and quinidine. Pharmacotherapy. 1994;14:698–703. [PubMed] [Google Scholar]
- 66.Kanani PM, Guse PA, Smith WM, Barnett A, Ellinwood EH. Acute deleterious effects of cocaine on cardiac conduction, hemodynamics, and ventricular fibrillation threshold: effects of interaction with a selective dopamine D1 antagonist SCH 39166. J Cardiovasc Pharmacol. 1998;32:42–48. [DOI] [PubMed] [Google Scholar]
- 67.Ohuoha DC, Schindler CW, Rothman RB. Serotonin-4 receptor antagonists reverse cocaine-induced cardiac arrhythmia. Life Sci. 1998;63:1673–1678. [DOI] [PubMed] [Google Scholar]
- 68.Liang R, Zhou Y, Wu F, Zhou C, Zhao X, Zhang M, Tian X, Zhu B. Effect of methamphetamine on potassium and L-type calcium currents in rat ventricular myocytes. Toxicol Mech Methods. 2010;20:458–465. [DOI] [PubMed] [Google Scholar]
- 69.Sugimoto K, Okamura K, Tanaka H, Takashima S, Ochi H, Yamamoto T, Matoba R. Methamphetamine directly accelerates beating rate in cardiomyocytes by increasing Ca(2+) entry via L-type Ca(2+) channel. Biochem Biophys Res Commun. 2009;390:1214–1220. [DOI] [PubMed] [Google Scholar]
- 70.Qu Y-H, Leung K-P, Qiao D-F, Li D-R, Liu C, Yue X, Wang H-J. Remodeling of ion channel expression may contribute to electrophysiological consequences caused by methamphetamine in vitro and in vivo. Biochem Biophys Res Commun. 2014;443:441–446. [DOI] [PubMed] [Google Scholar]
- 71.Koczor CA, Fields E, Jedrzejczak MJ, Jiao Z, Ludaway T, Russ R, Shang J, Torres RA, Lewis W. Methamphetamine and HIV-Tat alter murine cardiac DNA methylation and gene expression. Toxicol Appl Pharmacol. 2015;288:409–419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Zhuo L, Liu Q, Liu L, Sun T, Wang R, Qu G, Liu Q, Liu Y, Ren L. Roles of 3,4-methylenedioxymethamphetamine (MDMA)-induced alteration of connexin43 and intracellular Ca(2+) oscillation in its cardiotoxicity. Toxicology. 2013;310:61–72. [DOI] [PubMed] [Google Scholar]
- 73.Kevil CG, Goeders NE, Woolard MD, Bhuiyan MS, Dominic P, Kolluru GK, Arnold CL, Traylor JG, Orr AW. Methamphetamine Use and Cardiovascular Disease. Arterioscler Thromb Vasc Biol. 2019;39:1739–1746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Schürer S, Klingel K, Sandri M, Majunke N, Besler C, Kandolf R, Lurz P, Luck M, Hertel P, Schuler G, et al. Clinical Characteristics, Histopathological Features, and Clinical Outcome of Methamphetamine-Associated Cardiomyopathy. JACC Heart Fail. 2017;5:435–445. [DOI] [PubMed] [Google Scholar]
- 75.Zhao SX, Kwong C, Swaminathan A, Gohil A, Crawford MH. Clinical Characteristics and Outcome of Methamphetamine-Associated Pulmonary Arterial Hypertension and Dilated Cardiomyopathy. JACC Heart Fail. 2018;6:209–218. [DOI] [PubMed] [Google Scholar]
- 76.Darke S, Duflou J, Kaye S. Prevalence and nature of cardiovascular disease in methamphetamine-related death: A national study. Drug Alcohol Depend. 2017;179:174–179. [DOI] [PubMed] [Google Scholar]
- 77.Richards JR, Harms BN, Kelly A, Turnipseed SD. Methamphetamine use and heart failure: Prevalence, risk factors, and predictors. Am J Emerg Med. 2018;36:1423–1428. [DOI] [PubMed] [Google Scholar]
- 78.Abdullah CS, Aishwarya R, Alam S, Morshed M, Remex NS, Nitu S, Kolluru GK, Traylor J, Miriyala S, Panchatcharam M, et al. Methamphetamine induces cardiomyopathy by Sigmar1 inhibition-dependent impairment of mitochondrial dynamics and function. Commun Biol. 2020;3:682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.He SY, Matoba R, Fujitani N, Sodesaki K, Onishi S. Cardiac muscle lesions associated with chronic administration of methamphetamine in rats. Am J Forensic Med Pathol. 1996;17:155–162. [DOI] [PubMed] [Google Scholar]
- 80.Turdi S, Schamber RM, Roe ND, Chew HG, Culver B, Ren J. Acute methamphetamine exposure inhibits cardiac contractile function. Toxicol Lett. 2009;189:152–158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Simon SL, Richardson K, Dacey J, Glynn S, Domier CP, Rawson RA, Ling W. A comparison of patterns of methamphetamine and cocaine use. J Addict Dis. 2002;21:35–44. [DOI] [PubMed] [Google Scholar]
- 82.Westover AN, Nakonezny PA, Haley RW. Acute myocardial infarction in young adults who abuse amphetamines. Drug Alcohol Depend. 2008;96:49–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Haning W, Goebert D. Electrocardiographic abnormalities in methamphetamine abusers. Addiction. 2007;102 Suppl 1:70–75. [DOI] [PubMed] [Google Scholar]
- 84.Paratz ED, Zhao J, Sherwen AK, Scarlato R-M, MacIsaac AI. Is an Abnormal ECG Just the Tip of the ICE-berg? Examining the Utility of Electrocardiography in Detecting Methamphetamine-Induced Cardiac Pathology. Heart Lung Circ. 2017;26:684–689. [DOI] [PubMed] [Google Scholar]
- 85.Mladěnka P, Applová L, Patočka J, Costa VM, Remiao F, Pourová J, Mladěnka A, Karlíčková J, Jahodář L, Vopršalová M, et al. , TOX-OER and CARDIOTOX Hradec Králové Researchers and Collaborators. Comprehensive review of cardiovascular toxicity of drugs and related agents. Med Res Rev. 2018;38:1332–1403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Hawley LA, Auten JD, Matteucci MJ, Decker L, Hurst N, Beer W, Clark RF. Cardiac complications of adult methamphetamine exposures. J Emerg Med. 2013;45:821–827. [DOI] [PubMed] [Google Scholar]
- 87.Greene SL, Kerr F, Braitberg G. Review article: amphetamines and related drugs of abuse. Emerg Med Australas. 2008;20:391–402. [DOI] [PubMed] [Google Scholar]
- 88.Kafle P, Shrestha B, Mandal A, Sharma D, Bhandari M, Amgai B, Khalid M, Sidhu JS, Solaimanzadeh I, Gayam V, et al. Ecstasy induced acute systolic heart failure and Non-Ischemic Cardiomyopathy in a young female: a rare case report and literature review. J Community Hosp Intern Med Perspect. 2019;9:336–339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Henry BL, Minassian A, Perry W. Effect of methamphetamine dependence on heart rate variability. Addict Biol. 2012;17:648–658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Brody S, Krause C, Veit R, Rau H. Cardiovascular autonomic dysregulation in users of MDMA (“Ecstasy”). Psychopharmacology (Berl). 1998;136:390–393. [DOI] [PubMed] [Google Scholar]
- 91.Ito H, Yeo K-K, Wijetunga M, Seto TB, Tay K, Schatz IJ. A comparison of echocardiographic findings in young adults with cardiomyopathy: with and without a history of methamphetamine abuse. Clin Cardiol. 2009;32:E18–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Conen D, Glynn RJ, Sandhu RK, Tedrow UB, Albert CM. Risk factors for incident atrial fibrillation with and without left atrial enlargement in women. Int J Cardiol. 2013;168:1894–1899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Nishimura M, Bhatia H, Ma J, Dickson SD, Alshawabkeh L, Adler E, Maisel A, Criqui MH, Greenberg B, Thomas IC. The Impact of Substance Abuse on Heart Failure Hospitalizations. Am J Med. 2020;133:207–213.e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Thomas IC, Nishimura M, Ma J, Dickson SD, Alshawabkeh L, Adler E, Maisel A, Criqui MH, Greenberg B. Clinical Characteristics and Outcomes of Patients With Heart Failure and Methamphetamine Abuse. J Card Fail. 2020;26:202–209. [DOI] [PubMed] [Google Scholar]
- 95.Nishimura M, Ma J, Fox S, Toomu A, Mojaver S, Juang DK, Maisel AS, Thomas IC. Characteristics and Outcomes of Methamphetamine Abuse Among Veterans With Heart Failure. Am J Cardiol. 2019;124:907–911. [DOI] [PubMed] [Google Scholar]
- 96.Madhok A, Boxer R, Chowdhury D. Atrial fibrillation in an adolescent--the agony of ecstasy. Pediatr Emerg Care. 2003;19:348–349. [DOI] [PubMed] [Google Scholar]
- 97.Yu AJS, Rowe M, Martin P, Dahiya A. Reversible methamphetamine-induced cardiomyopathy mimicking arrhythmogenic right ventricular cardiomyopathy with ventricular tachycardia. HeartRhythm Case Rep. 2020;6:139–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Diffley M, Armenian P, Gerona R, Reinhartz O, Avasarala K. Catecholaminergic polymorphic ventricular tachycardia found in an adolescent after a methylenedioxymethamphetamine and marijuana-induced cardiac arrest. Crit Care Med. 2012;40:2223–2226. [DOI] [PubMed] [Google Scholar]
- 99.Packe GE, Garton MJ, Jennings K. Acute myocardial infarction caused by intravenous amphetamine abuse. Br Heart J. 1990;64:23–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Bazmi E, Mousavi F, Giahchin L, Mokhtari T, Behnoush B. Cardiovascular Complications of Acute Amphetamine Abuse: Cross-sectional study. Sultan Qaboos Univ Med J. 2017;17:e31–e37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Huang M-C, Yang S-Y, Lin S-K, Chen K-Y, Chen Y-Y, Kuo C-J, Hung Y-N. Risk of Cardiovascular Diseases and Stroke Events in Methamphetamine Users: A 10-Year Follow-Up Study. J Clin Psychiatry. 2016;77:1396–1403. [DOI] [PubMed] [Google Scholar]
- 102.Shetty S, Malik AH, Ali A, Yang YC, Briasoulis A, Alvarez P. Characteristics, trends, outcomes, and costs of stimulant-related acute heart failure hospitalizations in the United States. Int J Cardiol. 2021; [DOI] [PubMed] [Google Scholar]
- 103.Aspeslagh B, Calle P, De Pooter J. Wolff Parkinson White and recreational (meth)amphetamine use: a potentially lethal combination. Acta Clin Belg. 2020;1–4. [DOI] [PubMed] [Google Scholar]
- 104.Eigsti R, Firchau DJ, Nashelsky MB. 3,4-Methylenedioxymethamphetamine (MDMA, Ecstasy) Intoxication in a Young Adult with Giant Coronary Aneurysms from Kawasaki Disease. Acad Forensic Pathol. 2018;8:752–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Voizeux P, Lewandowski R, Daily T, Ellouze O, Bouchot O, Bouhemad B, Guinot P-G. Case of Cardiac Arrest Treated with Extra-Corporeal Life Support after MDMA Intoxication. Case Rep Crit Care. 2019;2019:7825915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Cooper WO, Habel LA, Sox CM, Chan KA, Arbogast PG, Cheetham TC, Murray KT, Quinn VP, Stein CM, Callahan ST, et al. ADHD drugs and serious cardiovascular events in children and young adults. N Engl J Med. 2011;365:1896–1904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Habel LA, Cooper WO, Sox CM, Chan KA, Fireman BH, Arbogast PG, Cheetham TC, Quinn VP, Dublin S, Boudreau DM, et al. ADHD medications and risk of serious cardiovascular events in young and middle-aged adults. JAMA. 2011;306:2673–2683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Akhgari M, Mobaraki H, Etemadi-Aleagha A. Histopathological study of cardiac lesions in methamphetamine poisoning-related deaths. Daru. 2017;25:5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Darke S, Kaye S, Duflou J. Rates, characteristics and circumstances of methamphetamine-related death in Australia: a national 7-year study. Addiction. 2017;112:2191–2201. [DOI] [PubMed] [Google Scholar]
- 110.Bjune T, Risgaard B, Kruckow L, Glinge C, Ingemann-Hansen O, Leth PM, Linnet K, Banner J, Winkel BG, Tfelt-Hansen J. Post-mortem toxicology in young sudden cardiac death victims: a nationwide cohort study. Europace. 2018;20:614–621. [DOI] [PubMed] [Google Scholar]
- 111.Richards JR. Beta Blockers and the Cardiac Complications of Methamphetamine. Heart Lung Circ. 2017;26:416–417. [DOI] [PubMed] [Google Scholar]
- 112.Hysek C, Schmid Y, Rickli A, Simmler LD, Donzelli M, Grouzmann E, Liechti ME. Carvedilol inhibits the cardiostimulant and thermogenic effects of MDMA in humans. Br J Pharmacol. 2012;166:2277–2288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, Jaffe AS, Jneid H, Kelly RF, Kontos MC, et al. , ACC/AHA Task Force Members, Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;130:2354–2394. [DOI] [PubMed] [Google Scholar]
- 114.Pujol-López M, Ortega-Paz L, Flores-Umanzor EJ, Perea RJ, Bosch X. Cardiac Magnetic Resonance as an Alternative to Endomyocardial Biopsy to Predict Recoverability of Left Ventricular Function in Methamphetamine- Associated Cardiomyopathy. JACC Heart Fail. 2017;5:853–854. [DOI] [PubMed] [Google Scholar]
- 115.Jones AA, Gicas KM, Seyedin S, Willi TS, Leonova O, Vila-Rodriguez F, Procyshyn RM, Smith GN, Schmitt TA, Vertinsky AT, et al. Associations of substance use, psychosis, and mortality among people living in precarious housing or homelessness: A longitudinal, community-based study in Vancouver, Canada. PLoS Med. 2020;17:e1003172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Jacob S, Panaich SS, Zalawadiya SK, McKelvey G, Abraham G, Aravindhakshan R, Sears SF, Conti JB, Marsh HM. Phantom shocks unmasked: clinical data and proposed mechanism of memory reactivation of past traumatic shocks in patients with implantable cardioverter defibrillators. J Interv Card Electrophysiol. 2012;34:205–213. [DOI] [PubMed] [Google Scholar]
- 117.Malhotra R, Patel S, Ramchand T, Al Nimri O. Higher defibrillation threshold in methamphetamine cardiomyopathy patients with implantable cardioverter-defibrillator. Indian Pacing Electrophysiol J. 2017;17:167–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Perrine SA, Nayak R, Bharadwaj AS, McKelvey G, Mohamad T, Jacob S. Effect of substance abuse on defibrillation threshold in patients with implantable cardioverter-defibrillator. Pacing Clin Electrophysiol. 2011;34:193–199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Chen J, Naseem RH, Obel O, Joglar JA. Habitual cocaine use is associated with high defibrillation threshold during ICD implantation. J Cardiovasc Electrophysiol. 2007;18:722–725. [DOI] [PubMed] [Google Scholar]
- 120.Kozor R, Grieve SM, Buchholz S, Kaye S, Darke S, Bhindi R, Figtree GA. Regular cocaine use is associated with increased systolic blood pressure, aortic stiffness and left ventricular mass in young otherwise healthy individuals. PLoS One. 2014;9:e89710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Darke S, Kaye S, Duflou J. Methamphetamine-related death is an under-addressed public health problem. Addiction. 2017;112:2204–2205. [DOI] [PubMed] [Google Scholar]
- 122.Om A, Warner M, Sabri N, Cecich L, Vetrovec G. Frequency of coronary artery disease and left ventricle dysfunction in cocaine users. Am J Cardiol. 1992;69:1549–1552. [DOI] [PubMed] [Google Scholar]
- 123.Diercks DB, Fonarow GC, Kirk JD, Jois-Bilowich P, Hollander JE, Weber JE, Wynne J, Mills RM, Yancy C, Peacock WF, ADHERE Scientific Advisory Committee and Investigators. Illicit stimulant use in a United States heart failure population presenting to the emergency department (from the Acute Decompensated Heart Failure National Registry Emergency Module). Am J Cardiol. 2008;102:1216–1219. [DOI] [PubMed] [Google Scholar]
- 124.Mahtta D, Ramsey D, Krittanawong C, Rifai MA, Khurram N, Samad Z, Jneid H, Ballantyne C, Petersen LA, Virani SS. Recreational substance use among patients with premature atherosclerotic cardiovascular disease. Heart. 2021;107:650–656. [DOI] [PubMed] [Google Scholar]
- 125.McLellan AT, Lewis DC, O’Brien CP, Kleber HD. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA. 2000;284:1689–1695. [DOI] [PubMed] [Google Scholar]
- 126.Brecht M-L, Herbeck D. Time to relapse following treatment for methamphetamine use: a long-term perspective on patterns and predictors. Drug Alcohol Depend. 2014;139:18–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Hubbard RL, Craddock SG, Anderson J. Overview of 5-year followup outcomes in the drug abuse treatment outcome studies (DATOS). J Subst Abuse Treat. 2003;25:125–134. [DOI] [PubMed] [Google Scholar]
- 128.Fisher DG, Reynolds GL, D’Anna LH, Hosmer DW, Hardan-Khalil K. Failure to get into substance abuse treatment. J Subst Abuse Treat. 2017;73:55–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Abuse NI on D. Characteristics of Drug-Dependent People [Internet]. National Institute on Drug Abuse. -- [cited 2021 Apr 24];Available from: https://www.drugabuse.gov/international/abstracts/characteristics-drug-dependent-people
- 130.Farber BA. Client deception about substance use: Research findings and a case study. J Clin Psychol. 2020;76:277–285. [DOI] [PubMed] [Google Scholar]
- 131.Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. Am J Health Promot. 1997;12:38–48. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.