
FIGURE 1.
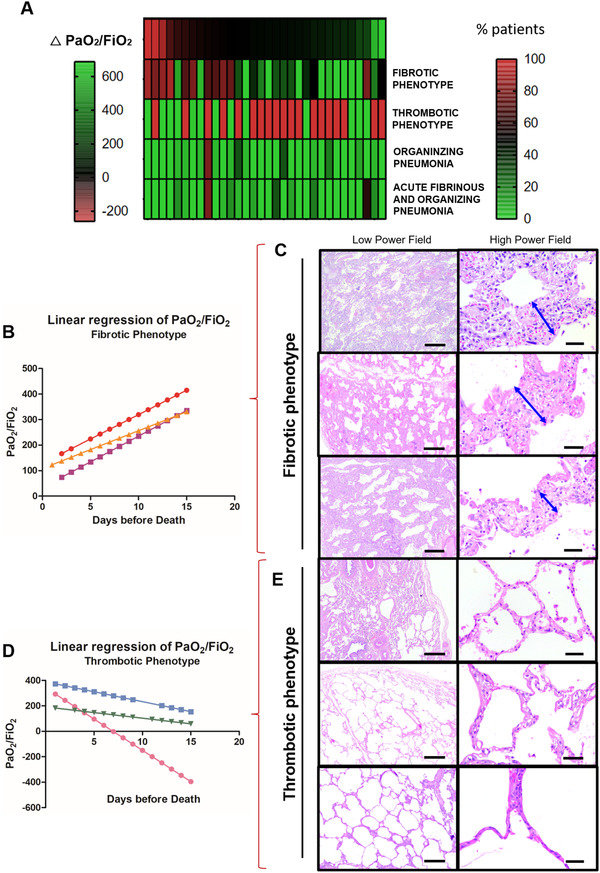
COVID‐19 bimodal clinical and pathological phenotypes. After a multidisciplinary discussion and data integration and analysis, bimodal clinical and pathological phenotypes of COVID‐19 minimally invasive autopsies were discovered by PaO2/FiO2 linear regression and lung morphology correlation, presented as a gradient (A). The two opposite ends of lung injury were named as (1) Fibrotic phenotype (N = 5) presenting progressive decline in PaO2/FiO2 ratio (B) with significant alveolar septal thickening by fibrosis (C–double blue arrows) without thrombus formation (C); and (2) Thrombotic Phenotype (N = 10) presenting a progressive increase in PaO2/FiO2 ratio (D) with recovery of acute/sub‐acute lung injury to or near to normal parenchyma architecture and thrombus formation on vessels (E). Between both phenotypes, a population (N = 32) of non‐bimodal phenotype with different stages of acute, organizing and fibrotic lung injury (A). Scale bar indicates 500 μm in the low power field and 50 μm in high power field (C and E)