
FIGURE 3.
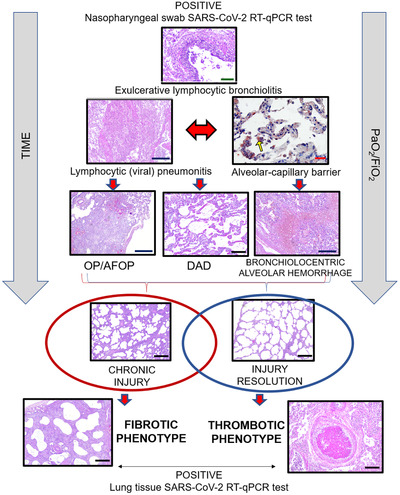
COVID‐19 lung pathophysiology. The viral infection starts in the lungs first by reaching the airways and infecting bronchial epithelial cells. Then, the pathophysiological processes in response to the viral attack cause an exulcerating lymphocytic bronchiolitis, followed by lymphocytic (viral) pneumonitis. Consequently, the second wave of infection overspreads through the lung parenchyma, inducing cellular pneumonitis, which injures the alveolo‐capillar barriers near distal airways, highlighted by immunohistochemistry with anti‐SARS‐CoV‐2 (yellow arrow). Then, fibroplastic balls (organizing pneumonia–OP) and fibrin balls (acute fibrinous and organizing pneumonia–AFOP), diffuse alveolar damaged (DAD) and bronchiolocentric alveolar hemorrhage may occur in the injured lung tissue. Over the time of viral infection and mechanical ventilation, two different repair processes can occur depending on the resolution or progression of the injury, coinciding with the bimodal clinic‐pathological phenotype: (1) Chronic injury with fibrotic phenotype; or (2) Gradual injury resolution with thrombotic phenotype. Scale bars indicate: 500 μm (blue), 200 μm (black), 100 μm (green) and 50 μm (red)