
FIGURE 2.
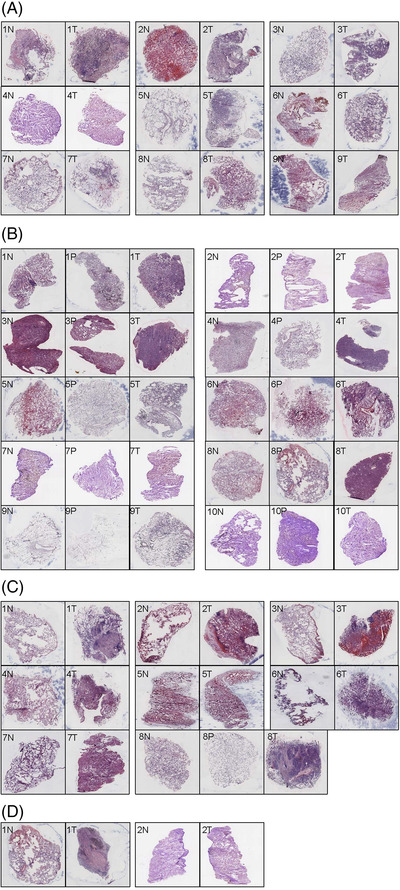
The haematoxylin and eosin (HE) staining images of different lung cancer types in paired samples, including normal tissues (N) and tumour tissues (T) or para‐tumour tissues(P). (A) Lung adenocarcinoma (LUAD: 9 N+T), 1N: the lung tissue structure was present, some alveoli collapsed and a few lymphocytes were infiltrated, 1T: the tumour cells showed invasive growth with less cytoplasm, hyperchromatic nuclei and diffuse infiltration, 2N: lung tissue structure was present and red blood cells were seen in alveolar cavities, 2T: adenocarcinoma cells were seen at the margins of the tissue, growing in an alveolar manner, 3N: normal lung tissue with minimal lymphocytic infiltration, 3T: LUAD with acinar growth, 4N: normal lung tissue with widened alveolar septum and mild fibrous hyperplasia, 4T: not clear enough to be recognised, 5N: the lung structure was basically normal, 5T: LUAD, mainly papillary type, a small amount of wall growth type, 6N: normal lung tissue with red blood cells in alveoli, 6T: LUAD, mainly with wall neoplasia, 7N: the lung structure was normal, 7T: mucinous adenocarcinoma with adherent growth, 8N: the lung tissue was basically normal, 8T: lung cancer mainly with adherent growth, 9N: normal lung tissue, some alveolar structures collapsed, 9T: not clear enough to be recognised. (B) LUAD: 10 N+P+T, 1N: normal lung tissue with minimal lymphocytic infiltration, 1P: the alveolar septum widened with mild fibrous hyperplasia and more dust deposition in lymphatic vessels, 1T: LUAD, adherent growth type, 2N: lung tissue was generally normal with mild fibrosis of the alveolar septum, 2P: alveolar interstitial fibrosis, no tumour tissue, 2T: small amount of acinar type tumour tissue, 3N: the alveolar structure collapsed with lymphocytic infiltration, 3P: alveolar interstitial fibrosis, 3T: LUAD, acinar type, 4N: widened alveolar septum with mild fibrosis, 4P: widened alveolar septum, 4T: LUAD, mainly acinar type, a few papillary type, 5N: lung tissue with some red blood cells, 5P: the lung structure was normal, 5T: a small number of tumour cells grew adherent to the wall, 6N: small amount of lung tissue with red blood cells, 6P: small amount of lung tissue with alveolar septum fibrous hyperplasia, 6T: LUAD, acinar type with marginal adherent growth, 7N: lung septum widened with fibrous tissue mildly hyperplasia, 7P: similar to 7N, 7T: a small number of heterotypic cells, adherant growth, 8N: normal, 8P: the alveolar septum widened with mild fibrous hyperplasia, 8T: LUAD, mainly acinar, some solid, 9N: normal, 9P: the organisational structure was incomplete, 9T: LUAD with adherent growth, 10N: normal, 10P: LUAD, mainly adherent growth, 10T: a small number of tumour cells grew adherent to the wall and mucus was visible in the alveolar cavity. (C) Lung squamous cell carcinomas (LUSC: 7 N+T & 1 N+P+T), 1N: normal, 1T: a large amount of mucus in the alveolar cavity and tumour cells grew adherent to the wall, 2N: basically normal, 2T: LUAD, signet ring cell type, 3N: normal lung tissue with red blood cells, 3T: the alveolar cavity was dilated, red blood cells were found in the cavity and a few lymphocytes were infiltrated in the stroma, none obvious tumour cells were found, 4N: normal, 4T: poorly differentiated carcinoma with solid growth, 5N: normal lung tissue with red blood cells in alveolar cavities, 5T: a small number of cancer cells grew in sheets, and red blood cells were seen in alveolar cavities, 6N: structure is incomplete, 6T: atypia cells, 7N: normal, 7T: small nodular lesions were observed without obvious cancer cells; 8N: basically normal, 8P: normal, 8T: poorly differentiated squamous cell carcinoma, nonkeratinised type. (D) Non‐small cell lung cancer (NSCLC: 2 N+T), 1N: normal, 1T: large necrosis was observed in the lesion, with more dust deposition, and no obvious malignant cells were observed, 2N: a small amount of fibrous hyperplasia in the alveolar septum, 2T: small nodular lesions were observed in the tissue with fibrous hyperplasia, none obvious malignant cells were observed