
Figure 1. The effects of varied plasma concentration on RB.
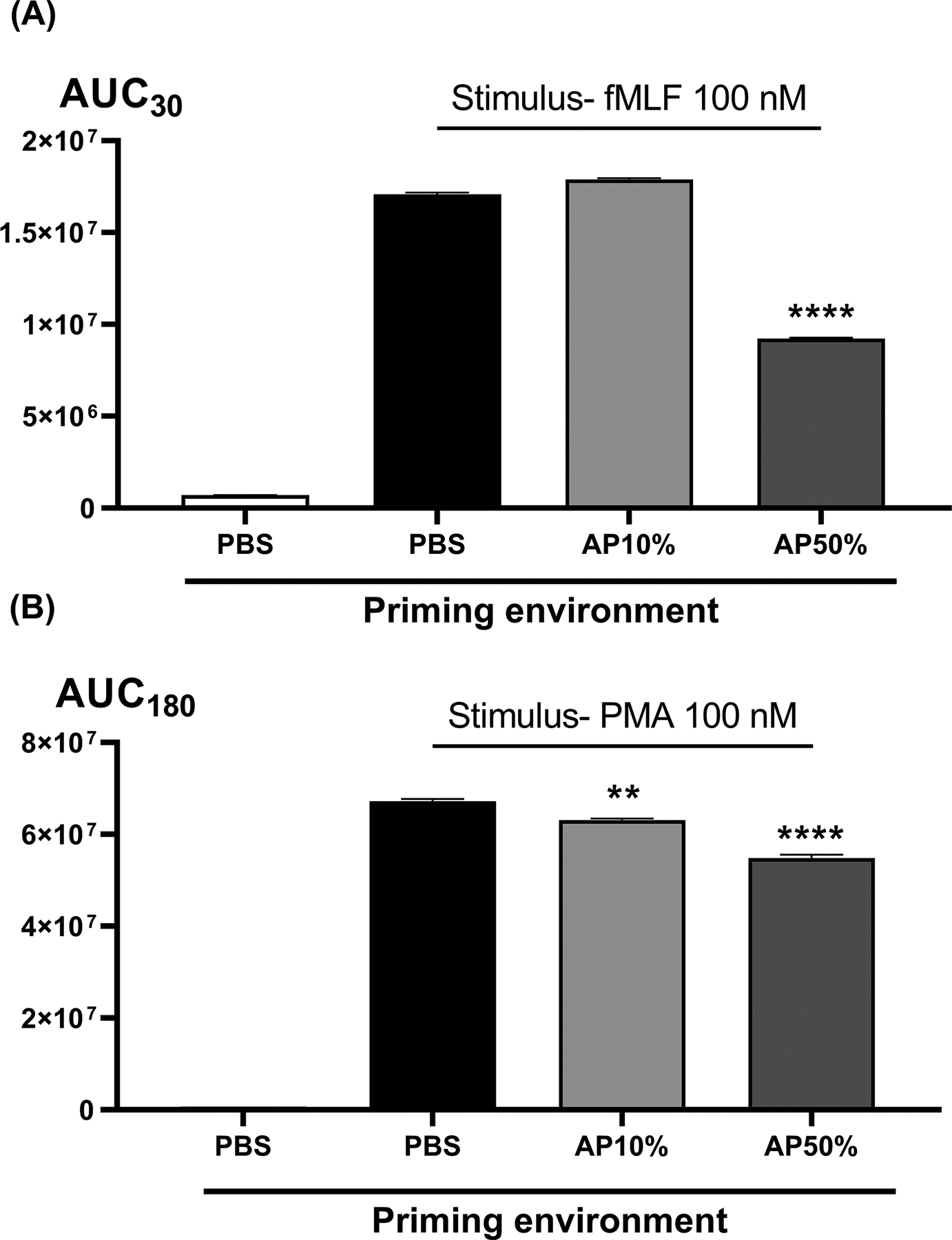
No RB is seen without terminal stimulation by either receptor-mediated fMLF (panel A) or receptor-independent PMA (panel B). Pre-incubation in high concentrations of autologous plasma (AP50%) quench respiratory burst as compared to pre-incubation in PBS media. By using lower concentrations of the autologous plasma to preincubate the cells though, we return RB measurements to the values seen after pre-incubation in PBS (Panel A, PBS vs AP10%). Then by varying the type of biofluid used at the preincubation stage we can see the residual biologic effects of that biofluid environment. For subsequent comparisons with trauma patient plasma we routinely used non-autologous (but healthy) control plasmas since the trauma plasma was always non-autologous. In side-by side comparisons (not shown) no differences in RB were seen after pre-incubation in 10% healthy volunteer (non-autologous) plasma vs 10% autologous plasma. AUCs were compared using one-way ANOVA / Tukey’s test (**p<0.01; ****p<0.001). AP, autologous plasma.