
Figure 2.
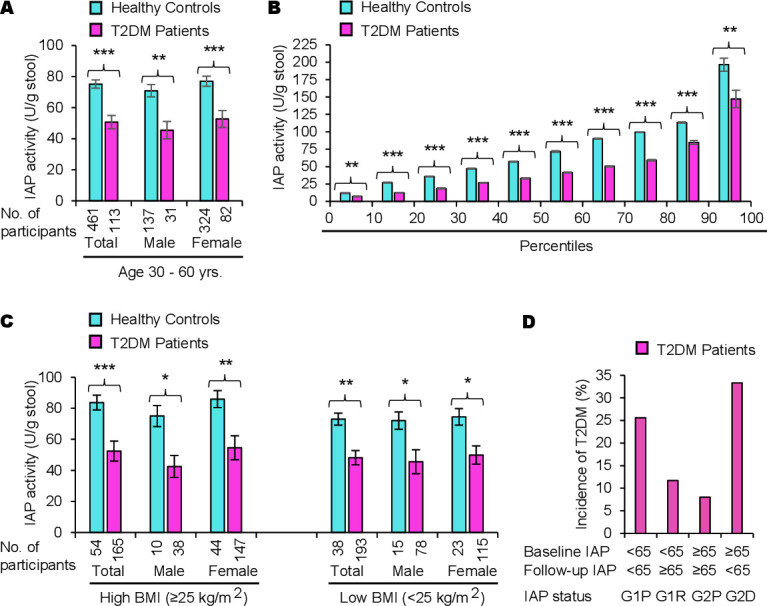
A high level of intestinal alkaline phosphatase (IAP) plays a protective role against type 2 diabetes mellitus (T2DM) irrespective of obesity. (A) Intestinal alkaline phosphatase deficiency (IAPD) is associated with T2DM. Participants, aged 30–60 years old, were screened for T2DM (see figure 1) and diagnosed as having T2DM or no T2DM (healthy controls). Data are summarized as mean (average)±SEM. Statistical significance of the difference between two groups was tested using unpaired two-tailed Student’s t-test. *p<0.05, **p<0.01, ***p<0.001. The post-hoc statistical power analyses revealed the powers for respective total, male, and female groups to be 100%, 100%, and 100%, respectively, which validated the adequacy of power (conventionally, >80% power at α=0.05) for respective sample sizes. Percentage loss of IAP in patients with T2DM compared with healthy controls: total, 32.6%; male, 35.8%; female, 31.6%. The average IAP level is 8.2% less in healthy control men compared with healthy control women; however, the difference is not significant (p=0.27561). (B) Percentile distributions showing IAP levels are low in patients with diabetes at all percentile points compared with healthy controls. Individual IAP values from each group (healthy controls or patients with T2DM) were organized from the lowest to the highest and then the average IAP value within each 10th percentile was calculated (n=11 within each 10th percentile for patients with T2DM and n=46 within each 10th percentile for healthy controls). The average values (mean±SEM) for corresponding percentiles are plotted. Note: Only the values in the first and last 10th percentile divisions will be greatly affected if an ‘outlier’ (a few extremely low or high values, compared with the most other values, affecting the mean value) is present. The values within the 10th and 90th percentiles are real, not affected by outliers. (C) A high level of IAP protects from T2DM irrespective of obesity. Patients with T2DM as well as healthy control participants were categorized into two groups, one group with high body mass index (BMI ≥25.0 kg/m2, includes obese and overweight persons) and the other group with low BMI (<25.0 kg/m2). Note: Persons with high BMI and high levels of IAP do not develop T2DM. There was no significant difference in IAP levels in healthy controls of high BMI and low BMI groups as well as in patients with T2DM of high and low BMI groups. (D) IAPD is associated with a higher incidence of T2DM. The percentage of incidence was calculated for the 5 years (see table 3). Note: Participants with ‘persistent IAPD’ (G1P) and ‘incident IAPD’ (G2D) have much higher incidence of T2DM compared with participants with ‘persistent no IAPD’ (G2P) and ‘remittent IAPD’ (G1R).