

Abstract
We herein report a novel technique for managing large forehead skin defects that include the eyebrows and upper eyelid. Case 1 was of a 55-year-old woman with an eccrine carcinoma (T2N0M0) at the right forehead, resulting in a skin defect 15 cm in diameter. Case 2 was of an 81-year-old man with a malignant peripheral nerve sheath tumor (T1a N0M0) at the left forehead, resulting in a skin defect 18 cm in diameter. A pedicled temporal hairline flap and free forearm flap were combined and placed on the defect, and good eyebrows and forehead morphology was ultimately achieved.
INTRODUCTION
Free flap surgery or the tissue-expander method is generally used for reconstruction of large forehead skin defects associated with resection of malignant tumors. However, when the eyebrow and upper eyelid are further dissected, reconstructive procedures become more complicated and the treatment period is extended. The middle hair at the temporal hairline is similar to that of the eyebrows in terms of hair flow, angle and density. Combining a temporal hairline flap, which includes the temporal hairline hair, with a free forearm flap can result in aesthetic and functional reconstruction outcomes in cases with complex, large forehead defects involving the eyebrows and upper eyelids. This method is a novel and useful reconstruction procedure that may shorten the rehabilitation period and hospital stay duration.
CASE PRESENTATION
Case 1
A 55-year-old woman suffered from eccrine carcinoma (T2N0M0 Stage II [UICC 7th]). Enlarged resection of the forehead and medial right eyebrow was performed at the subperiosteal level with a 25-mm margin around the tumor. The pathological findings (HE-staining) are also attached (Fig. 1).
Figure 1.

Enlarged resection of case1 and the pathological findings.
The bare forehead was covered with a forearm flap and the medial part of the right eyebrow was covered with a temporal hairline flap on the parietal hairline. Because the temporal hairline flap was raised as an island flap for eyebrow reconstruction, the same-side superficial temporal vessels were used as recipient vessels for eyebrow reconstruction. As a result, the recipient vessel for the free forearm flap had to be the opposite superficial temporal vessels (Fig. 2).
Figure 2.
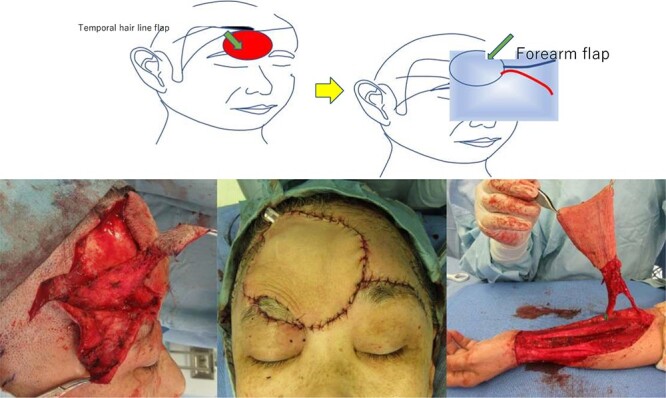
Intraoperative findings of case1 using a temporal hairline flap combined with a free forearm flap.
Two weeks after surgery, the patient returned to work. The condition at 8 weeks after surgery with no touch-up procedures is shown. No obvious metastasis was detected by whole-body computed tomography (CT), and there were no issues with opening or closing the eyelids (Fig. 3).
Figure 3.
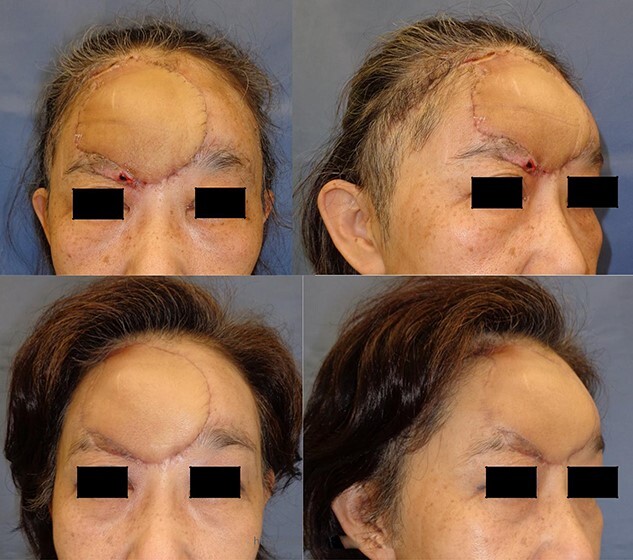
The condition at 8 weeks after surgery of case1 with no touch-up procedures is shown.
Case 2
An 81-year-old man suffered from malignant peripheral nerve sheath tumor (MPNST) G3 T1aN0M0 Stage II (UICC 6th). Enlarged resection of the forehead, left eyebrow and eyelid was performed at the subperiosteal level with a 30-mm margin around the tumor. The pathological findings (HE-staining) are also attached (Fig. 4).
Figure 4.
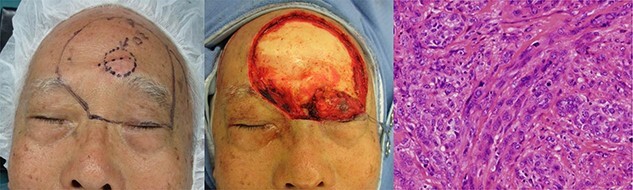
Enlarged resection of case 2 and the pathological findings.
The bare forehead was covered with a temporary artificial dermis and the left eyebrow and eyelid were covered with a temporal hairline flap at the parietal hairline. Since complete removal was confirmed on the permanent pathological specimen, reconstruction of the forehead with a free forearm flap was performed 4 weeks after the surgery. Because a temporal hairline flap pedicled with frontal branch of superficial temporal vessels was raised as a transposition flap for eyebrow reconstruction, the same-side parietal branch of the superficial temporal vessels was used as the recipient vessel for the free forearm flap (Fig. 5).
Figure 5.
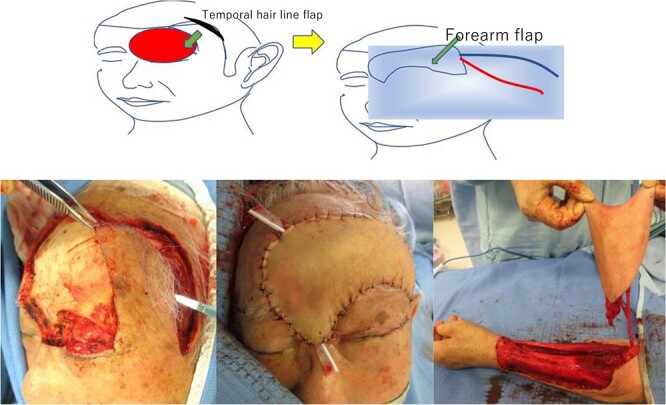
Intraoperative findings of case 2 using a temporal hairline flap combined with a free forearm flap.
The condition at 1 year after surgery with no touch-up procedures is shown. No obvious metastasis was detected by whole-body CT. Mild left eyelid dysfunction remains, but there is no corneal dysfunction (Fig. 6).
Figure 6.

The condition at 1 year after surgery of case 2 with no touch-up procedures is shown.
DISCUSSION
Free flap surgery or the tissue-expander method is generally used for reconstruction of large forehead skin defects associated with resection of malignant tumors. However, when the eyebrow and upper eyelid are further dissected, reconstructive procedures become more complicated and the treatment period is extended. Procedures such as single-hair transplantation or coarse-containing/vellus hair free skin grafting are commonly reported for reconstruction of eyebrow defects. These techniques can match the eyebrow hair flow and hair angle, but the low engraftment rate of transplanted hair remains a clinical challenge. In addition, these methods are often not applicable when the transplant bed and surrounding tissue have also been lost, such as after extensive resection of a malignant tumor [1]. Although subcutaneous island flap [2] and superficial temporal artery flap [3] have been reported as flap-based eyebrow reconstruction methods, they result in so-called ‘toothbrush’-like reconstructed eyebrows and are inferior in terms of appearance because of the thick hair and large skin angle [4]. The middle hair at the temporal hairline is similar to that of the eyebrows in terms of hair flow, angle and density as well as good compatibility between the thickness of the forehead skin and the thickness of the forearm flap. Thus, combining a temporal hairline flap with a free forearm flap can result in aesthetic and functional reconstruction with complex, large forehead defects involving the eyebrows and upper eyelids [5].
There have been no reports of simultaneous reconstruction of combined defects of the upper eyelid and eyebrows, so this method will likely prove extremely useful, as it can shorten rehabilitation period and hospital stay duration.
CONCLUSIONS
The presently proposed reconstruction procedure using a temporal hairline flap Combined with a free forearm flap is extremely useful for covering large, complex forehead defects including the eyebrows and upper eyelids.
DECLARATION OF COMPETING INTEREST
There is no conflict of interest to disclose.
FUNDING
None declared.
INFORMED CONSENT AND PATIENT DETAILS
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
Contributor Information
Masakatsu Hihara, Department of Plastic and Reconstructive Surgery, Kansai Medical University, Osaka, Japan.
Rina Hikiami, Department of Plastic and Reconstructive Surgery, Kansai Medical University, Osaka, Japan.
Toshihito Mitsui, Department of Plastic and Reconstructive Surgery, Kansai Medical University, Osaka, Japan.
Natsuko Kakudo, Department of Plastic and Reconstructive Surgery, Kansai Medical University, Osaka, Japan.
Maki Okamoto, Department of Plastic and Reconstructive Surgery, Kansai Medical University, Osaka, Japan.
Atsuyuki Kuro, Department of Plastic and Reconstructive Surgery, Kansai Medical University, Osaka, Japan.
Kenji Kusumoto, Department of Plastic and Reconstructive Surgery, Kansai Medical University, Osaka, Japan.
References
- 1. Matsuda K, Shibata M, Kanazawa S, Kubo T, Hosokawa K. Eyebrow reconstruction using a composite skin graft from sideburns. Plast Reconstr Surg Glob Open 2015;3:e290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Omranifard M, Doosti MI. A trial on subcutaneous pedicle island flap for eyebrow reconstruction. Burns 2010;36:692–7. [DOI] [PubMed] [Google Scholar]
- 3. Kajikawa A, Ueda K. Bilateral eyebrow reconstruction using a unilateral extended superficial temporal artery flap. Ann Plast Surg 2003;50:416–9. [DOI] [PubMed] [Google Scholar]
- 4. Juri J. Eyebrow reconstruction. Plast Reconstr Surg 2001;107:1225–8. [DOI] [PubMed] [Google Scholar]
- 5. Motomura H, Muraoka M, Nose K. Eyebrow reconstruction with intermediate hair from the hairline of the forehead on the pedicled temporoparietal fascial flap. Ann Plast Surg 2003;51:314–8 discussion 19-20. [DOI] [PubMed] [Google Scholar]