

Abstract
In comparison with the single-bundle technique, double-bundle anterior cruciate ligament (ACL) reconstruction has proven its superiority regarding biomechanical studies and clinical outcomes in both rotational knee stability and anterior translation function. However, the complexity and risk of complications remain a great concern for the orthopaedic surgeon performing double-bundle ACL reconstruction. We present a simplified double-bundle ACL reconstruction by the 3-inside technique with 2 suspension buttons and 1 interference screw. The semitendinosus tendon is tripled to be the anteromedial (AM) bundle, whereas the gracilis is doubled for the posterolateral (PL) bundle. We perform a 3-socket approach with an inside-out femoral tunnel for the AM bundle, an outside-in femoral tunnel for the PL bundle, and a retrograde tibial socket for the tibial bundle. Thus, this technique is, simply, a combination of 2 procedures: one single all-inside method (for the AM bundle) and one outside-in method (for the PL bundle), with which most arthroscopic surgeons are familiar. The AM and PL bundles are fixed at 30° and 45°, respectively, using 2 suspension buttons and 1 interference screw. Our simplified technique could reduce surgical costs and minimize complications while maintaining isometric position and appropriate graft size for each patient.
Technique Video
The full detailed technique showing all steps of the operation.
Anterior cruciate ligament (ACL) reconstruction failure remains a challenge for orthopaedic surgeons, even though this procedure is commonly performed, approaching the number of 100,000 and 200,000 cases per year in United States in the last decade.1 One of the factors that affects the outcome of anterior cruciate ligament reconstruction (ACLR) is that the reconstructed ACL cannot maintain biomechanics and anatomic features. This is a hindrance for patients to fully recover to perform their daily activities effectively. ACLR without normal biomechanical restoration leads to exceedingly loose or overconstrained grafts, resulting in a malfunctioning knee and later the development of osteoarthritis.2 In comparison with the single-bundle technique, double-bundle reconstruction has proven its superiority regarding biomechanical studies and clinical outcomes, in both rotational knee stability and anterior translation function.3, 4, 5, 6, 7, 8 The double-bundle ACLR (DBACLR) can reconstruct “a more native ACL,” which is originally composed of 2 functional bundles with 4 anatomical insertion sites, providing 2 tension patterns for each bundle. However, the traditional DBACLR technique requires 4 isolated tunnels and 4 methods of fixation, which increases operational time, cost, and possible complications.9
Among DBACLR techniques, the modified DBACLR method performs only 3 tunnels (2 femoral tunnels and 1 tibial tunnel), demonstrating equivalent kinematic stability, in both cadaveric models and clinical research, with the traditional techniques.10,11 Drilling only one tunnel at the tibial plateau instead of 2 helps to decrease the risk of tunnel communication, socket wall damage, and operative complications.10,11 With this technique, some authors chose an all-inside technique for 2 bundles with 3 adjustable suspensions called “the simplified fixation method”; however, this technique is still a challenge for surgeons. In addition, in this technique, surgeons have to use 3 suspension buttons, which increases the total cost, leaving a financial burden on patients in developing countries.12 Fortunately, while inside-out fixation remains the standard of the DBACLR techniques, recent improvements in all-inside reconstruction devices have led to a growth in their popularity.13
In this article, we perform a simple DBACLR technique using only 2 suspension buttons and 1 interference screw. We still use a 3-socket approach with 2 anatomic femoral tunnels and 1 traditional tibial tunnel. Semitendinosus tendon is used for the anteromedial (AM) bundle and is fixated in an all-inside manner, whereas the gracilis is prepared for the posterolateral (PL) bundle and is secured with a screw.
Technically, this operation is simply a combination of 2 procedures: one single all-inside method (for the AM bundle) and one outside-in method (for the PL bundle), which is familiar to most arthroscopic surgeons. Furthermore, this modified technique solves the problem of the small size of hamstring autografts in the Asian population when processing DBACLR by GraftLink.10,14 Furthermore, it lowers the cost of used implants. For all these reasons, full steps along with pearls and pitfalls for this updated technique will be introduced in detail as follow.
Surgical Technique (With Video Illustration)
The whole technique is detailed visually in Video 1.
Patient Preparation
Under spinal anesthesia, the patient is positioned supine with the knee flexed to 90°. A thigh tourniquet is inflated to a pressure of 300 mm Hg. The knee is marked with a surgical pen to identify the patellofemoral joint, femorotibial joint, patellar tendon, iliotibial (IT) band, AM portal, and anterolateral (AL) portal. Standard AM and AL portals are established for arthroscope and hand device working, as demonstrated in Fig 1. A routine arthroscopic knee assessment is done for joint assessment, confirmation of the injury, debridement, and dealing with any chondral or meniscal pathologies found.
Fig 1.

Anteromedial and anterolateral portal for arthroscopy.
Graft Harvesting and Sizing
Semitendinosus and gracilis tendons are harvested by a tendon stripper via a 3-cm incision over the pes anserinus on the medial tibial plateau in the ordinary manner, as presented in Fig 2. Then, the semitendinosus tendon is tripled and temporarily secured with one circle of suture to make a temporary AM bundle. The gracilis tendon is doubled and prepared for the PL bundle graft. AM and PL bundles along with a group of both bundles (tibial bundle) are measured for diameters by the Arthrex Graft Sizing Block (Arthrex, Naples, FL), as shown in Fig 3.
Fig 2.

Semitendinosus and gracilis tendons are harvested to prepare for graft.
Fig 3.

Graft sizing: anteromedial bundle (A) and tibial bundle (B) using an Arthrex Graft Sizing Block.
Tunnel Preparation
After sizing the diameters of the AM, PL, and tibial bundle, we drill 3 tunnels based on each bundle’s diameter, beginning with the femoral tunnel for the AM bundle, passing by the femoral tunnel for the PL bundle, and finishing by the tibial tunnel. The instruments required for this procedure are shown in Fig 4.
Fig 4.

Instruments to prepare for tunnels. (A) Instruments to prepare for femoral anteromedial bundle tunnel: 7- to 9-mm drill, 5.0-mm drill, 2.0-mm guide pin, Bullseye Femoral Off-set Guide. (B) Instruments to prepare for femoral posterolateral bundle tunnel: Pinn-ACL guide ConMed, 2.0-mm guide pin, 5.0-mm reamer, and 6.0-mm reamer (C) Instruments to prepare for the tibial socket: Pinn ACL guide ConMed, 2.0-mm guide pin, 5.0-mm Drill, and FlipCutter II Drill (Arthrex).
Femoral Tunnel for AM Bundle: Inside-Out
The shaver and radiofrequency instruments are used to debride the lateral wall of the intercondylar notch. Radiofrequency is also used to mark for AM and PL bundle anatomic placements as described by Fu et al.15 (Fig 5). The anatomic footprints of the AM and PL bundles are in the lower 30% to 35% of the notch wall. The femoral AM socket is reamed for traditional ENDOBUTTON fixation. After placing the knee in 110 to 120° of flexion and under visualizing from the AL portal, we insert a femoral ACL Drill Guide through the AM portal to mark the AM bundle placement (Fig 6). The femoral tunnel is drilled through the femoral condyle from inside to the lateral thigh outside, using the guide pin, and drilling continues using the 5.0-mm drill bit. Then, the femoral socket for the AM bundle is reamed to the measured diameter of the AM graft, leaving at least 1 cm of cortical bone for hanging the ENDOBUTTON later (Fig 7). Usually, the length of the femoral socket is from 30 to 35 mm.
Fig 5.
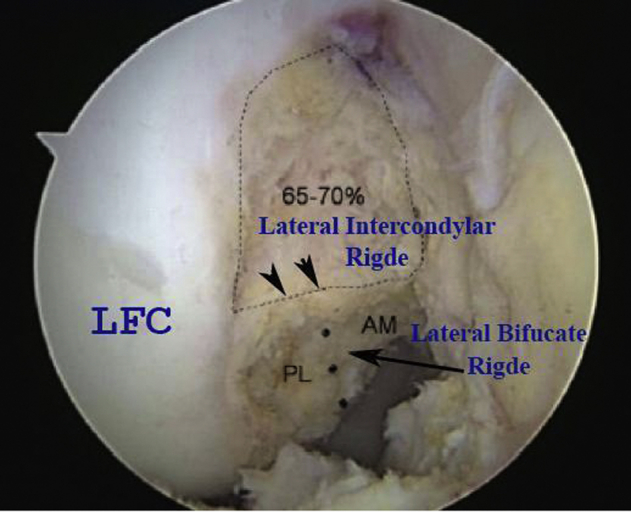
Arthroscopic anteromedial (AM) portal view of the right knee in 90° of flexion. AM and posterolateral (PL) bundles’ anatomic footprints are in the lower 30% to 35% of the notch wall, below the lateral intercondylar ridge. The PL bundle footprint is just lateral to AM footprint, separated by the lateral bifurcate ridge. (LFC, lateral femoral condyle.)
Fig 6.

Drilling femoral tunnel for anteromedial (AM) bundle. The knee was placed in 110 to 120° of flexion, under visualizing from the anterior lateral portal, and then a femoral ACL Drill Guide is inserted through the AM portal to mark the AM bundle placement.
Fig 7.

The femoral tunnel is drilled using the guide pin, then a 5.0-mm drill bit, and finished with an appropriate drill bit based on measured anterior medial graft diameter.
Femoral Tunnel for PL Bundle: Outside-In
A posterolateral (PL) socket is conveniently made for interference screw fixation. Before drilling the socket, a 2- to 3-cm incision is made to expose the IT band, visualizing the socket place at the lateral condylar to avoid damaging the neurovascular structures. The skin incision is just anterior and superior to the lateral femoral epicondyle and above the anterior part of the IT band (Fig 8). The Pinn-ACL guide (ConMed, Largo, FL) is placed in a position, inside the knee joint, where it points to the femoral premarked footprint of the PL inside and outside. It is away from the patellofemoral joint and lateral tibiofemoral joint by at least 2 cm (Fig 9). Through the Pinn-ACL guide, we drill the outside-in tunnel, beginning with the 2.0-mm guide pin, and finishing with the 6.0-mm drill bit, preparing for the 7-mm interference screw for later fixation. Now, the 2 femoral tunnels can be seen under the arthroscopic view (Fig 10).
Fig 8.
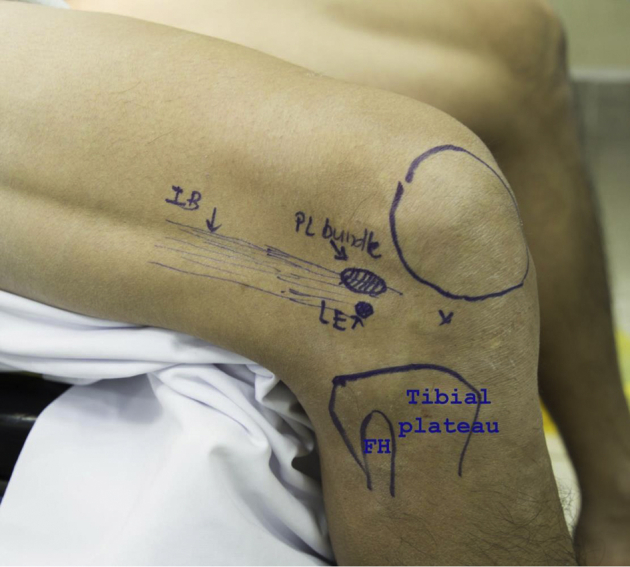
The skin incision to visualize the socket place for the PL tunnel. The skin incision is just anterior and superior to the lateral femoral epicondyle, above the anterior part of the IB. (FH, fibular head; IB, iliotibial band; LE, lateral epicondyle; PL, posterolateral.)
Fig 9.

View from the knee joint, the Pinn-ACL guide is placed at the femoral premarked footprint of the posterolateral bundle. View from the outside, its position is away from the patellofemoral joint and lateral tibiofemoral joint at least 2 cm.
Fig 10.
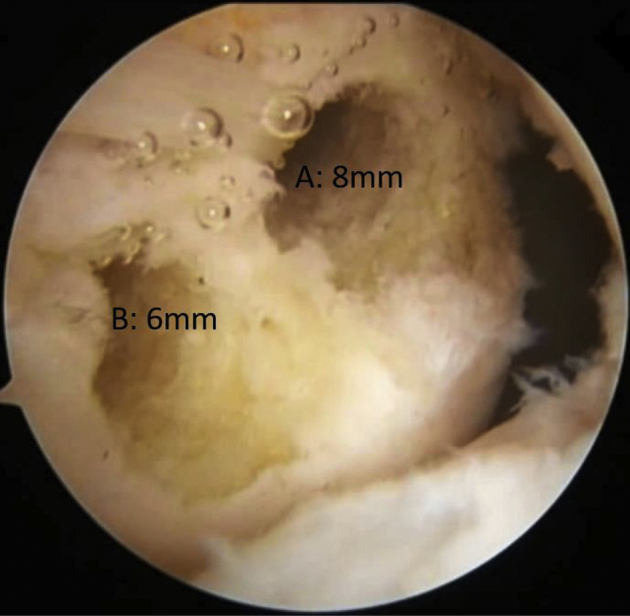
The 2 femoral tunnels under arthroscopic. (A) The 8-mm diameter anteromedial tunnel. (B) The 6-mm diameter posterolateral tunnel.
Tibial Socket for Tibial Bundle: Retrograde
After the Pinn-ACL guide is placed at the center footprint of the ACL at the tibial plateau, the 25- to 30-mm length socket, with a diameter equal to the measured tibial bundle size, is created by using the 2.0-mm needle guide, followed by the 5.0-mm drill bit outside-in, and ending with the FlipCutter II drill bit (Arthrex) inside-out (Fig 11). It is essential to reserve at least 1 cm of cortical bone outside. Usually, the length of this tibial tunnel ranges from 35 to 45 mm. Three conducting sutures passing from the AM portal, through the 3 made tunnels, are used for pulling the grafts to the joint to be stabilized inside the sockets.
Fig 11.

The Pinn-ACL guide is placed at the center footprint of the anterior cruciate ligament at the tibial plateau.
Graft Preparation
After completing the socket preparation, the appropriate lengths of AM and PL bundles are estimated for graft preparation. The AM bundle is prepared according to the GraftLink technique (Arthrex) with 2 stitches on each end using number 2 ParcusBraid (Parcus Medical, LLC, Sarasota, FL) (Fig 12). The semitendinosus is tripled with an ENDOBUTTON loop (nonadjustable loop) (FixLoop + Noraker, Lyon, France) and an adjustable loop (FixLoop + Noraker) attached to the femoral and tibial ends, respectively (Fig 5). Then, the 3-strain AM bundle is adjusted to the given length (typically 6.0-7.0 cm) before being secured with a nonabsorbable FiberWire. The gracilis tendon is doubled for the PL bundle and secured to the adjustable loop at the distal end of the AM bundle (Fig 13). The tibial AM and PL bundles are finally sized for diameter again before inserting into the knee joint.
Fig 12.
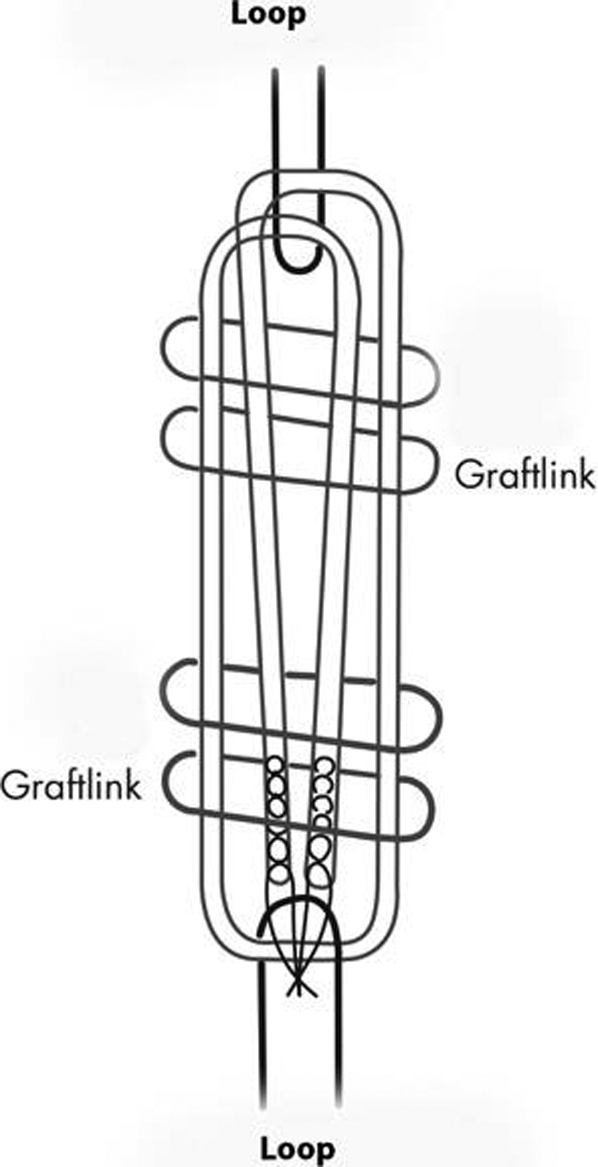
The anterior medial graft is braided based on GraftLink technique, with 2 stitches of number 2 ParcusBraid (Parcus Medical) on each end (typically 6 cm to 7.0 cm in length).
Fig 13.

The tibial ends of anteromedial (AM) and posterolateral bundle are attached to an adjustable loop (FixLoop + Noraker). The femoral end of AM bundle is attached to a nonadjustable loop (FixLoop Noraker).
Graft Insertion
First, the AM bundle is inserted into the joint through the AM portal. The proximal end is fixated at the femoral condyle by the ENDOBUTTON loop in the traditional manner (Fig 14). Then, the PL bundle is also introduced through the AM portal. Finally, the distal end of the 2 bundles (tibial bundle), which are connected by an adjustable loop, is pulled back into the joint via the AM portal, and then passed through the tibial tunnel to outside.
Fig 14.

The anteromedial (AM) bundle is inserted through the AM portal.
Graft Fixation
The 2 bundles of the reconstructed ligament are fixed at 2 different knee flexion angles following 3 steps:
Step 1: Fixing the proximal end of the AM bundle with the fixed ENDOBUTTON loop (described previously).
Step 2: Fixing the tibial end of AM bundle while tensioning the bundle with the knee at 30°flexion and then fastening the adjustable loop in an all-inside fashion (Fig 15).
Fig 15.

Fixation of the tibial end of the graft at 30° knee flexion.
Step 3: At the condyle, fixing the proximal end of the PL bundle with 1 interference screw (EUROSCREW; Teknimed, L’Union, France) outside-in while the knee is flexed at 45°. Anatomic ACL tension is confirmed under the arthroscopic view (Fig 16).
Fig 16.

Confirmation of anterior cruciate ligament graft tension under the arthroscopic view.
Follow-Up and Postoperative Training
Like the single-bundle method, the scar of the PL bundle’s incision on the outer thigh surface is often more prominent and early attached to the IT band. This scar usually turns to normal in the third month, when the knee movement improves.
The patient is trained with an intensive exercise rehabilitation program. It includes crutches-protected weight-bearing exercises in the first week, long-knee bracing for another 3 weeks, and regular walking and running starting from the fourth month. The patient may return to their normal exercise routine from the fifth month if all criteria are achieved.
Discussion
We hereby present a double-bundle ACL reconstruction technique using 2 suspension buttons and one interference screw. While ACL naturally consists of 2 bundles, the AM and the PL, the classic single-bundle reconstruction could not obtain the correct physiological function of the real bundles as well as their anatomical fixed position.16,17 The double-bundle reconstruction technique was first described by Mott in 1983,18 proving the advantages in both aspects of biomechanics and clinical studies.19, 20, 21, 22
The double-bundle technique was quite technically sophisticated and more invasive. Thus, it appeared to have many complications. This creates controversy in choosing between different approaches. Compared with the 4-tunnel double-bundle ACL reconstruction technique, the technique of 3 tunnels is believed to gain the same level of stability, with easier technical steps and less complication.23
The described ACL reconstruction technique is based on 3 tunnels, including 1 tibial tunnel and 2 femoral tunnels. This separation was believed to be better, as it has more advantages and a wide range of applications than the split of 1 femoral tunnel and 2 tibial tunnels. Those advantages could be listed as follows: (1) It can be done on all sizes of the knee because surgeons need only one tunnel in the tibial plateau, such as the case with the single-bundle technique. This point is especially important to those who have short statures like female patients and Southeast Asian patients. (2) The condyle can always provide enough space to drill 2 separate tunnels, and there have been no reports of complications in the condylar wall. (3) The postoperative exercise program will not change; however, the patient can return to the training earlier due to better firmness when making this technique. (4) Regarding the ligament strength, hanging the grafts by the loop device on the tibial plateau is superior to the screw.
Compared with other techniques, we believe that our 3-inside technique of ACLR attains significant advantages in some points summarized in Table 1. First, the AM bundle is made via tripling the semitendinosus tendon, and the PL bundle is made via doubling the gracilis tendon. This method is based on the significance of the AM bundle, which needs to be larger and stronger (usually requires larger than 7 mm in diameter) compared with the PL bundle.24 In addition, the AM bundle is created via the GraftLink Technique with 2 stitches on each end to ensure its strength.
Table 1.
Advantages and Limitations of the DBACLR Technique Using Only Two Suspension Buttons and One Interference Screw
| Advantages | Limitations |
|---|---|
| Reconstructed ACL 2 bundles in the correct anatomical isometric position. | PL bundle: small size with an average of 5 mm in diameter. |
| Each bundle is fixed at a specific angle to get the optimal biomechanical recovery. | Risk of rupture of the osseous septum between the 2 AM and PL bundle tunnels at the femoral condyle due to malposition of ACL guide placement or wrong direction of femoral drilling. |
| Cost-saving and low risk of complications. | In the White or Black populations, whose PL bundle may be oversized, there is a greater risk of femoral tunnel confluence on the medial–lateral condylar surface. |
| Simple technique and easy to perform. | Whether a 45° flexion is optimal when fixating the PL bundle. |
ACL, anterior cruciate ligament; AM, anteromedial; DBACLR, double-bundle anterior cruciate ligament reconstruction; PL, posterolateral.
Second, we modify the process of drilling the tunnels and braiding the grafts by measuring the diameter of the bundles when creating 5-strand ligaments (before fixing them), drilling the tunnels corresponding to these diameters, and estimating the length of the graft (based on the length of the tunnel) so that its length in the tunnel is at least 1.5 to 2.0 cm. After determining the appropriate size, we proceed to braid and fix the bundles to the loop. This method helps to create the most suitable graft size for each patient.
Third, the proximal end of the AM bundle is fixed by an ENDOBUTTON, which is simpler, cheaper, and safer than the adjustable loop. Furthermore, the proximal end of the PL bundle is fixed by one interference screw, which is manageable, feasible, and secure. Based on these characteristics, preparation for ACL reconstruction surgery using 2 bundles and 3 tunnels is not different from that of a single-bundle all-inside technique, with only the exception of using one screw for the upper PL bundle at the condyle. Along with a recent study, there is no difference in the range of motion, Lysholm, International Knee Documentation Committee category, and Tegner scores between graft fixation devices. Thus, this approach not only helps simplify the technique but also saves the surgery expenses.25
Fourth, we determine the position for hanging the PL bundle to reduce the complications. An incision is made on the lateral side of the thigh, which is upon the IT band. This area does not contain any vital structures. Therefore, it would be an appropriate site for anchoring the PL bundle with no significant complications. However, locating the outer surface of the lateral femoral condyle could sometimes be difficult in obese patients.
Lastly, 45° of knee flexion is chosen to fix the PL bundle. To establish the maximal tensile strength, several studies have reported that the ideal AM fixing position is when the knee is in 30° flexion. However, there are considerable controversies over the PL fixing site. Some authors flexed the knee to 90°, whereas others supported the usage of a 45° for fixing the PL bundle. In simulated motion, regarding the PL bundle, it will be at the maximal relaxation at 90°and maximal tensile strength at 0 degrees of knee flexion. Therefore, we chose 45° of knee bend when fixing the PL bundle so that these bundles are not too tight when extending the knee to the maximum and not too loose when the knee is bent 90°. During the surgery, all knees are bent over 90° and extend to the maximum without any struggling. Thus, the 2 bundles of AM and PL are fixed at 30° and 45°, respectively, while both are in the isometric position.
However, certain limitations to this technique can be listed. There is a risk of rupture of the osseous septum between the 2 AM and PL bundle tunnels at the femoral condyle. Although we have not encountered such a case, it might occur if the ACL guide is placed in the incorrect position, or if the direction of drilling is inaccurate. Second, we have not performed this method in White or Black populations, whose PL bundle may be oversized compared with individuals of Asian descent. This is because of the concern about the availability of enough space to drill the PL bundle without causing femoral tunnel confluence on the lateral condylar surface if the PL bundle is larger than 6.5 mm. Moreover, we have not been able to prove whether a 45° flexion is optimal when fixating the PL bundle, although after fixing the PL bundle at 45 flexion degrees, there was no restriction in the knee range of movement. Under endoscopic examination, the PL bundle was also not overstretched or slack in that range. In addition, sometimes the PL bundle cannot be placed on the posterolateral side of the AM bundle. In these cases, the PL bundle must be removed and reattached. To place the PL bundle in the correct position, it should be placed at the lateral side of the adjustable loop; then, a separate pulling rope is tied around the distal end of the PL bundle to adjust the PL bundle direction before pulling the 2 bundles into the tibial tunnel. All limitations and pitfalls of this technique are summarized in Table 1 and Table 2, respectively.
Table 2.
Pearls and Pitfalls of the DBACLR Technique Using Only Two Suspension Buttons and One Interference Screw
| Pearls | Pitfalls | |
|---|---|---|
| Preparing the graft by GraftLink technique with 2 stitches on each end. | Enhance the security and strength of grafts. | |
| ACL reconstruction process following grafts sizing, tunnels drilling, and graft insertion | Reconstruct the appropriate graft sizes for each tunnel. | Takes time, sometimes a re-drill of the tunnels is necessary. |
| Using an ENDOBUTTON for the proximal end of the AM bundle | Feasible, cost-saving, and low rate of complications. | AM bundle may be too long or too short in the tibial socket. |
| Femoral tunnel for PL bundle: outside- in | Reproducible | |
| Fixing the PL bundle at 45° of knee flexion. | Reach the isometric position. | |
| One tibial socket for AM & PL bundles | PL bundle placement at the posterolateral side to the AM bundle in the tibial socket is not always feasible. |
ACL, anterior cruciate ligament; AM, anteromedial; DBACLR, double-bundle anterior cruciate ligament reconstruction; PL, posterolateral.
In summary, by creating 3 tunnels using the all-inside technique for AM bundle accompanied by the standard technique for PL bundle, 2 suspension buttons, and 1 interference screw, we simplified the DBACLR technique, saved costs, and minimized complications.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
The full detailed technique showing all steps of the operation.
References
- 1.Mall N.A., Chalmers P.N., Moric M., et al. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2014;42:2363–2370. doi: 10.1177/0363546514542796. [DOI] [PubMed] [Google Scholar]
- 2.Tashman S., Kolowich P., Collon D., Anderson K., Anderst W. Dynamic function of the ACL-reconstructed knee during running. Clin Orthop Relat Res. 2007;454:66–73. doi: 10.1097/BLO.0b013e31802bab3e. [DOI] [PubMed] [Google Scholar]
- 3.Tsai A.G., Wijdicks C.A., Walsh M.P., Laprade R.F. Comparative kinematic evaluation of all-inside single-bundle and double-bundle anterior cruciate ligament reconstruction: A biomechanical study. Am J Sports Med. 2010;38:263–272. doi: 10.1177/0363546509348053. [DOI] [PubMed] [Google Scholar]
- 4.Kondo E., Merican A.M., Yasuda K., Amis A.A. Biomechanical comparisons of knee stability after anterior cruciate ligament reconstruction between 2 clinically available transtibial procedures: Anatomic double bundle versus single bundle. Am J Sports Med. 2010;38:1349–1358. doi: 10.1177/0363546510361234. [DOI] [PubMed] [Google Scholar]
- 5.Plaweski S., Petek D., Saragaglia D. Morphometric analysis and functional correlation of tibial and femoral footprints in anatomical and single bundle reconstructions of the anterior cruciate ligament of the knee. Orthop Traumatol Surg Res. 2011;97(6 suppl):S75–S79. doi: 10.1016/j.otsr.2011.07.004. [DOI] [PubMed] [Google Scholar]
- 6.Chowdhury A.Z., Ali M.H., Faisal M.A., et al. Anterior cruciate ligament reconstruction using autologous hamstring double bundle graft compared with single bundle graft procedures. Mymensingh Med J. 2019;28:126–136. [PubMed] [Google Scholar]
- 7.Oh J.Y., Kim K.T., Park Y.J., et al. Biomechanical comparison of single-bundle versus double-bundle anterior cruciate ligament reconstruction: A meta-analysis. Knee Surg Relat Res. 2020;32:14. doi: 10.1186/s43019-020-00033-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sinha S., Naik A.K., Kumar A., Jacob T., Kar S. Analysis of modified double-bundle anterior cruciate ligament reconstruction with implantless fixation on tibial side. Chin J Traumatol. 2020;23:341–345. doi: 10.1016/j.cjtee.2020.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brophy R.H., Wright R.W., Matava M.J. Cost analysis of converting from single-bundle to double-bundle anterior cruciate ligament reconstruction. Am J Sports Med. 2009;37:683–687. doi: 10.1177/0363546508328121. [DOI] [PubMed] [Google Scholar]
- 10.Yasen S.K., Logan J.S., Smith J.O., Nancoo T., Risebury M.J., Wilson A.J. TriLink: Anatomic double-bundle anterior cruciate ligament reconstruction. Arthrosc Tech. 2014;3:e13–e20. doi: 10.1016/j.eats.2013.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ahn J.H., Choi S.-H., Wang J.H., Yoo J.C., Yim H.S., Chang M.J. Outcomes and second-look arthroscopic evaluation after double-bundle anterior cruciate ligament reconstruction with use of a single tibial tunnel. JBJS. 2011;93:1865–1872. doi: 10.2106/JBJS.K.00136. [DOI] [PubMed] [Google Scholar]
- 12.Connaughton A.J., Geeslin A.G., Uggen C.W. All-inside ACL reconstruction: How does it compare to standard ACL reconstruction techniques? J Orthop. 2017;14:241–246. doi: 10.1016/j.jor.2017.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lubowitz J.H., Ahmad C.S., Anderson K. All-inside anterior cruciate ligament graft-link technique: Second-generation, no-incision anterior cruciate ligament reconstruction. Arthroscopy. 2011;27:717–727. doi: 10.1016/j.arthro.2011.02.008. [DOI] [PubMed] [Google Scholar]
- 14.Conte E.J., Hyatt A.E., Gatt C.J., Jr., Dhawan A. Hamstring autograft size can be predicted and is a potential risk factor for anterior cruciate ligament reconstruction failure. Arthroscopy. 2014;30:882–890. doi: 10.1016/j.arthro.2014.03.028. [DOI] [PubMed] [Google Scholar]
- 15.Fu F.H., van Eck C.F., Tashman S., Irrgang J.J., Moreland M.S. Anatomic anterior cruciate ligament reconstruction: A changing paradigm. Knee Surg Sports Traumatol Arthrosc. 2015;23:640–648. doi: 10.1007/s00167-014-3209-9. [DOI] [PubMed] [Google Scholar]
- 16.Karlsson J., Irrgang J.J., van Eck C.F., Samuelsson K., Mejia H.A., Fu F.H. Anatomic single- and double-bundle anterior cruciate ligament reconstruction, part 2: Clinical application of surgical technique. Am J Sports Med. 2011;39:2016–2026. doi: 10.1177/0363546511402660. [DOI] [PubMed] [Google Scholar]
- 17.Tashman S., Collon D., Anderson K., Kolowich P., Anderst W. Abnormal rotational knee motion during running after anterior cruciate ligament reconstruction. Am J Sports Med. 2004;32:975–983. doi: 10.1177/0363546503261709. [DOI] [PubMed] [Google Scholar]
- 18.Mott H.W. Semitendinosus anatomic reconstruction for cruciate ligament insufficiency. Clin Orthop Relat Res. 1983;(172):90–92. [PubMed] [Google Scholar]
- 19.van Eck C.F., Kopf S., Irrgang J.J., et al. Single-bundle versus double-bundle reconstruction for anterior cruciate ligament rupture: A meta-analysis—does anatomy matter? Arthroscopy. 2012;28:405–424. doi: 10.1016/j.arthro.2011.11.021. [DOI] [PubMed] [Google Scholar]
- 20.Buoncristiani A.M., Tjoumakaris F.P., Starman J.S., Ferretti M., Fu F.H. Anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2006;22:1000–1006. doi: 10.1016/j.arthro.2006.06.005. [DOI] [PubMed] [Google Scholar]
- 21.Yagi M., Wong E.K., Kanamori A., Debski R.E., Fu F.H., Woo S.L. Biomechanical analysis of an anatomic anterior cruciate ligament reconstruction. Am J Sports Med. 2002;30:660–666. doi: 10.1177/03635465020300050501. [DOI] [PubMed] [Google Scholar]
- 22.Cho S., Muneta T., Ito S., Yagishita K., Ichinose S. Electron microscopic evaluation of two-bundle anatomically reconstructed anterior cruciate ligament graft. J Orthop Sci. 2004;9:296–301. doi: 10.1007/s00776-004-0779-2. [DOI] [PubMed] [Google Scholar]
- 23.Drews B.H., Seitz A.M., Huth J., Bauer G., Ignatius A., Durselen L. ACL double-bundle reconstruction with one tibial tunnel provides equal stability compared to two tibial tunnels. Knee Surg Sports Traumatol Arthrosc. 2017;25:1646–1652. doi: 10.1007/s00167-016-4199-6. [DOI] [PubMed] [Google Scholar]
- 24.Katouda M., Soejima T., Kanazawa T., Tabuchi K., Yamaki K., Nagata K. Relationship between thickness of the anteromedial bundle and thickness of the posterolateral bundle in the normal ACL. Knee Surg Sports Traumatol Arthrosc. 2011;19:1293–1298. doi: 10.1007/s00167-011-1417-0. [DOI] [PubMed] [Google Scholar]
- 25.Wang Y., Lei G., Zeng C., et al. Comparative risk-benefit profiles of individual devices for graft fixation in anterior cruciate ligament reconstruction: A systematic review and network meta-analysis. Arthroscopy. 2020;36:1953–1972. doi: 10.1016/j.arthro.2020.04.023. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The full detailed technique showing all steps of the operation.
The full detailed technique showing all steps of the operation.