
Figure 1. BAL fluid obtained from patients with CLAD demonstrate elevated levels of IL-6 and sIL-6R when compared to CLAD free controls.
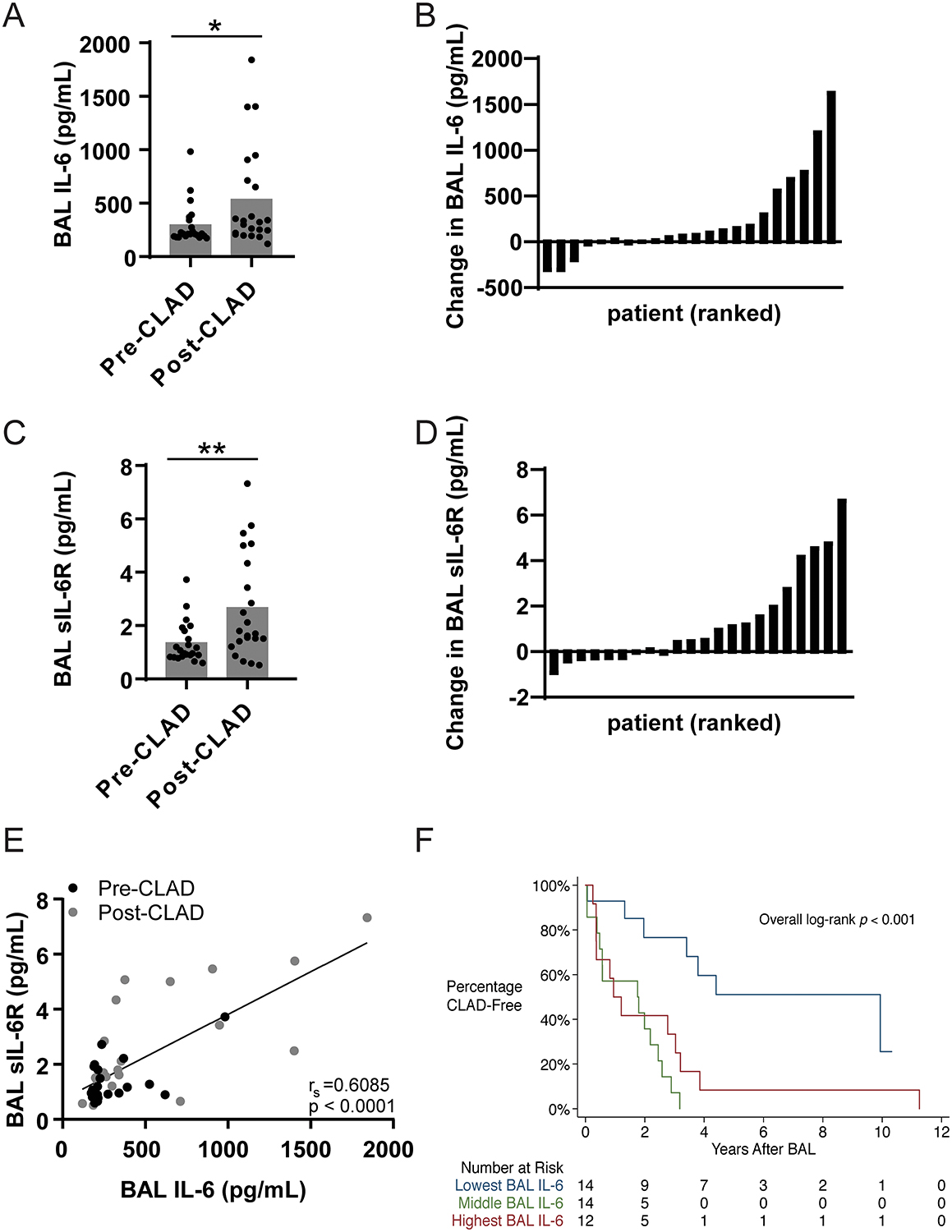
(A) BAL concentrations of IL-6 were measured by ELISA for 22 matched pre-CLAD and post-CLAD samples and were compared using a matched pair Wilcoxon test. Post-CLAD samples had significantly higher IL-6 levels (535.2±476.7pg/mL) compared to CLAD free controls (296.0±193.2pg/mL, Wilcoxon test p=0.0251). (B) Absolute change in BAL IL-6 concentration per patient ranked in ascending order. (C) Post-CLAD BAL samples also had higher levels of sIL-6R (2.670±1.96pg/mL), measured by ELISA, compared to CLAD free controls (1.385±0.77pg/mL; Wilcoxon test p=0.0074). (D) Absolute change in BAL sIL-6R concentration per patient ranked in ascending order. (E) There is a significant linear correlation between IL-6 and sIL-6R levels in both pre-CLAD (Spearman’s correlation=0.3056, p=0.0076), post-CLAD (Spearman’s correlation=0.5011, p=0.0002), and combined groups (shown). (F) The parent cohort of 40 one-year surveillance bronchoscopies was subdivided into tertiles based on BAL IL-6 levels (<180 pg/mL, 180–212 pg/mL, >212 pg/mL) and compared using standard Kaplan-Meyer analysis. Patients in the lowest tertile had significantly longer time to CLAD onset compared to patients in the middle or upper tertiles (media survival 4.402 vs. 1.777 vs. 1.077 years respectively, p=0.001).