
Figure 1. Pragmatic approach to atherosclerotic cardiovascular disease (ASCVD) risk assessment and prevention in treated HIV infection.
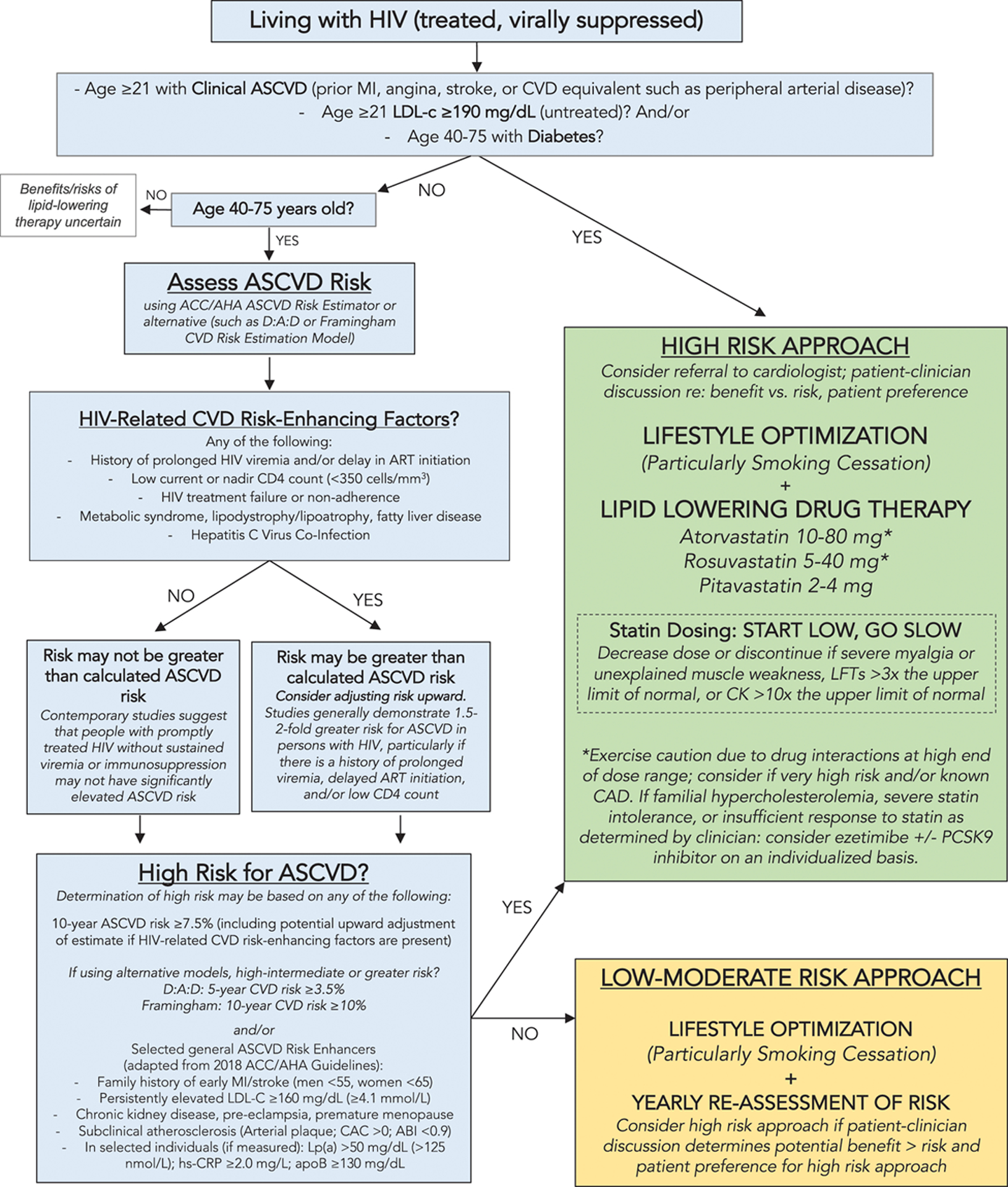
(Reprinted with permission Circulation [2019], 140:e98-e124 © 2019 American Heart Association, Inc.). This figure applies to people with controlled HIV. For people with uncontrolled HIV, the first priority is appropriate HIV therapy to achieve viral suppression. Thresholds based on findings of elevated CVD risk at current or nadir CD4 count <200, <350, and <500 cells/mm3 in Silverberg et al. (2014), Lichtenstein et al., 2010 and Triant et al., 2010. Hazard ratios and incidence rate ratios of 1.4 to 2.1 for myocardial infarction (MI) for people living with HIV (PLWH) vs uninfected people demonstrated in Freiberg et al., (2013) Triant et al., 2007 and Silverberg et al. (2014). Hazard ratio of stroke for PLWH vs. uninfected people was 1.40 in Chow et al. (2012).
Note. ABI indicates ankle-brachial index; ACC/AHA, American College of Cardiology/American Heart Association; apoB, apolipoprotein B; ART, antiretroviral therapy; CAC, coronary artery calcium; CAD, coronary artery disease; CK, creatine kinase; CVD, cardiovascular disease; D:A:D, Data Collection on Adverse Events of Anti-HIV Drugs; hs-CRP, high sensitivity C-reactive protein; LFT, liver function test; LDL-C, low-density lipoprotein cholesterol; Lp(a), lipoprotein A; and PCSK9, proprotein convertase subtilisin-kexin type 9.