
Figure 2: Schematic representations of tAIH-Induced motor plasticity.
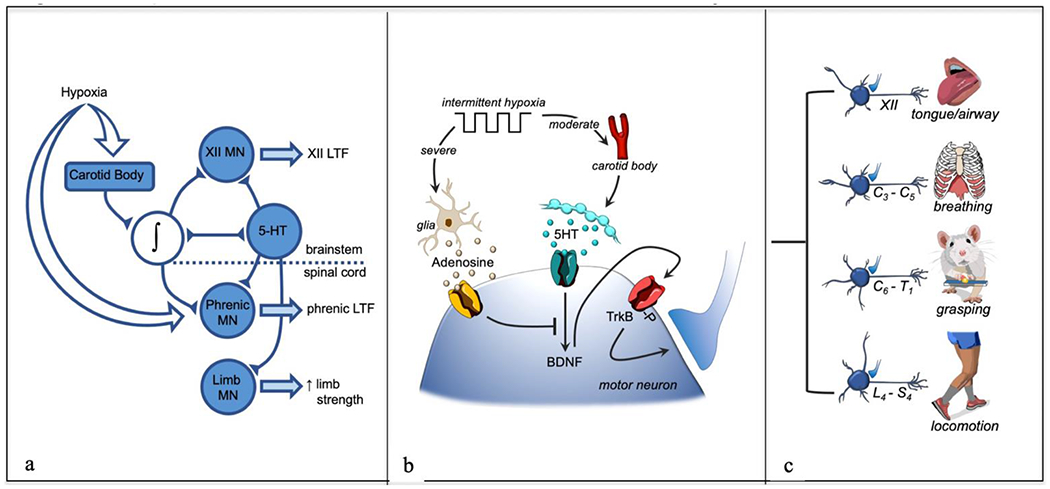
In panel a: Neural network model of tAIH-induced plasticity, including hypoglossal (XII), phrenic and limb motor neurons (MN). In panel b: Working model of cellular mechanisms giving rise to tAIH-induced motor plasticity. Moderate acute intermittent hypoxia (Po2 >40 mmHg) activates carotid body chemo-afferent neurons that then activate raphe serotonergic neurons and trigger serotonin release in widespread motor nuclei. Serotonin activates Gq coupled 5-HT receptors, initiating phrenic motor facilitation via the Q pathway (serotonin-induced, BDNF protein synthesis). Spinal tissue hypoxia also stimulates glia to release of ATP/adenosine into the extracellular space; subsequent binding to Gs coupled adenosine 2A receptors on motor neurons elicits a distinct intracellular signaling cascade that either: 1) elicits a distinct form of phrenic motor plasticity (but only at severe levels of tissue hypoxia), and/or 2) inhibits the Q pathway via cross-talk inhibition. In panel c: tAIH effects are widespread among motor neuron pools, leading to plasticity of many motor systems, including: tongue/upper airway (XII), breathing (C3-C5), grasping (C6-T1) and locomotion (L4-S4). Thus, tAIH elicits global effects on motor neurons that elicit outcomes depending on the target muscle. The impact of AIH is enhanced by combination with task specific training, amplifying BDNF/TrkB effects within the targeted (task specific) motor system.