

Abstract
Takotsubo syndrome – also known as broken-heart syndrome, Takotsubo cardiomyopathy, and stress-induced cardiomyopathy – is a recently discovered acute cardiac disease first described in Japan in 1991. This review aims to update understanding on the epidemiology, pathophysiology, clinical presentation, diagnosis, and treatment of Takotsubo syndrome, highlighting aspects of interest to cardiologists and general practitioners.
Key words: broken-heart syndrome, stress cardiomyopathy, Takotsubo cardiomyopathy, Takotsubo syndrome
Background
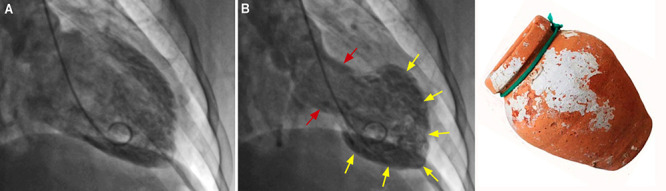
Takotsubo syndrome (TTS) – also known as broken-heart syndrome, Takotsubo cardiomyopathy, and stress-induced cardiomyopathy – is a recently discovered acute cardiac disease first described in Japan in 1991.1 TTS has a clinical presentation with chest pain, ischaemic electrocardiographic (ECG) changes, and elevation of biomarkers, such as cardiac troponin and brain natriuretic peptide (BNP), triggered by significant emotional or physical stress, and accompanied by distinct patterns of transient left ventricular dysfunction.2,3This contractile dysfunction classically adopts an apical ballooning shape of the left cardiac chamber resembling a Japanese octopus trap named a Takotsubo (figure 1).4,5 TTS mimics acute coronary syndrome (ACS) and can be indistinguishable from that disease if the coronary arteries are demonstrated to be normal.6,7 In this scenario, a differential diagnosis – although challenging – is essential for ensuring correct treatment.
Figure 1. Left ventriculography from a right anterior oblique view in a patient with typical Takotsubo syndrome. A. End-diastolic image. B. End-systolic image showing hyperkinesis of the base of the left ventricle (red arrows) but akinesis of the mid and apical segments (yellow arrows), resembling a traditional Japanese octopus trap (takotsubo) (right).
Epidemiology
TTS is more frequent in women than men; thus, about 90% of patients are postmenopausal women.4,8 Approximately 2% of all patients presenting with suspected ACS also have TTS.9-11
Aetiology, predisposition, risk factors, and triggers
The aetiology of TTS is not fully understood, despite intensive research into its possible causes.
Endocrine factors
The higher incidence of TTS in postmenopausal women suggests hormonal influences. Reduced oestrogen levels during menopause increase endothelial dysfunction (imbalance between vasoconstricting and vasodilating factors) leading to microvascular coronary artery spasm, one of the pathogenetic mechanisms proposed for TTS.12
Genetics
A few studies have reported an association between TTS and the expression of some genes, such as
BAG3 and GRK-5.13,14 However, there are conflicting results.15 Currently, there is a large genetic study ongoing among patients with TTS to identify potential genetic predisposition to the disease.16
Psychogenic factors
There is a higher prevalence of TTS in patients with neurological and psychiatric pathologies.3 This association could represent an extracardiac association that should be considered. Depression and anxiety are more common in patients with TTS than in those with ACS or in healthy controls.17,18 Depressed patients have an exaggerated norepinephrine response to emotional stress,19 and patients with anxiety have decreased re-absorption of norepinephrine because of failure in re-uptake transporters.20 TTS can also occur in patients with central nervous system diseases involving brain-heart interactions,21 such as ischaemic stroke,22 subarachnoid haemorrhage,23 and seizures.24
Triggers
Emotional and physical stressors include one or more of the following: divorce, illness or death of a loved one, job loss, bad financial news, earthquakes and aftershocks, car accidents, strokes, seizures, asthma attacks, phaeochromocytoma, giving birth, cancers, infectious diseases, surgery, and anaesthesia.4
It has even been triggered by SARS-CoV-2 infection.25
Pathophysiology
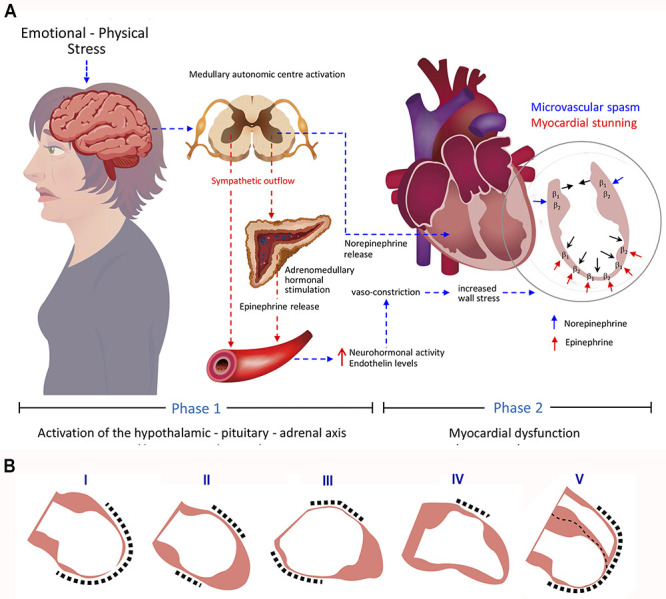
The exact pathophysiology of TTS remains incompletely understood. Nevertheless, the hypothesis of the involvement of a catecholamine surge is the most accepted, currently. This involves an adrenergic cascade through the hypothalamic–pituitary–adrenal axis.26,27 This pathogenic mechanism involves two phases, shown in figure 2A. Phase 1 involves activation of the hypothalamic–pituitary-adrenal axis, and phase 2 involves myocardial dysfunction induced by sympathetic hyperactivity. The first phase begins after an acute psychological and/ or physical stress resulting in increased circulating and myocardial catecholamine levels.28,29 During the second phase, different mechanisms have been considered to explain the cardiotoxicity of catecholamines producing myocardial dysfunction. Among these, the most prominent are direct catecholamine-mediated myocardial stunning and microvascular spasm.27
Figure 2. A. Diagram representing the phases involved in the most accepted pathophysiological mechanism of Takotsubo syndrome. Beta1-adrenergic receptor (norepinephrine binds preferentially to these receptors and has a positive inotropic effect); beta2-adrenergic receptor (when epinephrine binds to these receptors at supraphysiological levels has a negative inotropic effect). B. Diagram representing the five types of Takotsubo syndrome based on left ventricular angiograms: I, apical type, the typical and most common variant; II, midventricular atypical variant; III, basal atypical variant; IV, focal atypical variant; and V, isolated right ventricular or biventricular variant.
Myocardial stunning
In this, rising catecholamine levels act on beta-adrenergic receptors, triggering the onset of myocardial dysfunction and affecting inotropic cardiac function.28 During severe stress, circulating epinephrine peaks, making the beta-adrenergic receptors most sensitive to its negative inotropic effects.26
Beta-adrenergic receptors have their highest concentration in the apical myocardium, with a gradient decrease from apex to base, which could explain the left ventricular dysfunction pattern most typically seen in patients with TTS (figure 2A).30 The causes of the atypical and different anatomical variants in TTS are unknown. The affected myocardium observed in cases of TTS is accompanied by severe histological abnormalities resulting from the direct toxicity of catecholamines, as well as catecholamine-mediated microcirculatory disturbances followed by ischaemia, however, with potential for rapid functional recovery.31
As will be discussed later in this review, the lack of persistent myocardial damage in patients with TTS is demonstrated in the findings observed on cardiac magnetic resonance imaging, showing only significant myocardial oedema with no evidence of late gadolinium enhancement. This excludes the possibility of significant fibrosis, suggesting that the damage to the dysfunctional myocardium is transient.32
Microvascular spasm
Since TTS was first described, in addition to spasm of the epicardial coronary arteries, diffuse coronary vasoconstriction was documented and can have a pathogenic role.1 Some authors consider that severe and prolonged microvascular constriction causes acute transient myocardial ischaemia in patients with TTS, leading to a severe impairment of left ventricle (LV) contractility involving areas of increased wall stress, such as the mid-left ventricular wall and the apex.32,34 Therefore, TTS may be considered a novel form of ACS.35
Clinical presentation
TTS usually presents clinically as an ACS, mostly in postmenopausal women, triggered by an episode of acute emotional or unusual physical stress. The most common symptoms are chest pain and dyspnoea.4Physical examinations can be normal or with nonspecific findings.
According to left ventriculography studies, four anatomical variants of TTS have been described: the apical type (approximately 80%), represents the most commonly described or typical variety characterised by apical ballooning, hypo-, a-, or dyskinesia of mid-apical myocardial segments. This is followed, in terms of frequency, by the atypical variants: the midventricular type (15–18%), featuring hypo-, a-, or dyskinesia of midventricular segments; the basal type (2%) where only basal segments are involved; and the focal type (1.5%) mainly affecting an anterolateral segment.3,36 Other variants include isolated right ventricular dysfunction or biventricular dysfunction (figure 2B).37
TTS is clinically indistinguishable from acute myocardial infarction (AMI), so its diagnosis is frequently a challenge. A critical score to differentiate TTS from ACS was proposed by the International Takotsubo Registry. This score includes seven criteria, which are given different points according to their diagnostic importance, as shown in table 1.38 Thus, a patient with a score of 30 points has a predictive probability of <1% of having TTS, and one with >70 points has a probability of approximately 90% of being diagnosed with TTS.38 The diagnosis of TTS is mainly based on proposed guidelines, such as those of the Mayo Clinic,10 the European Society of Cardiology,39 and the international diagnostic criteria (InterTAK Diagnostic Score).4 The latter recommends the use of cardiac magnetic resonance (CMR) imaging to exclude infectious myocarditis and for diagnostic confirmation in patients with wall motion abnormalities extending beyond the myocardial territory of a single coronary artery. Approximately, one-third of patients with suspected TTS can have an apical acute myocardial infarction (AMI), as defined using CMR for the final diagnosis.40 The same recommendation should apply in patients with an old myocardial infarction.41 In this scenario, CMR is essential to differentiate TTS from AMI and myocarditis accurately, demonstrating myocardial oedema and the absence of late gadolinium enhancement, ensuring optimal treatment.42-44
Table 1. Clinical predictors for the diagnosis of Takotsubo syndrome.
|
Criteria |
Points |
|---|---|
|
Female sex |
25 |
|
Emotional trigger |
24 |
|
Physical trigger |
13 |
|
Absence of ST-segment depression* |
12 |
|
Psychiatric disorders |
11 |
|
Neurological disorders |
9 |
|
QTc prolongation |
6 |
|
Total |
100 |
*Except in lead aVR
Differentiation from ACS
The diagnosis of ACS relies on the presence of chest pain associated with ECG changes with ischaemic pattern and elevation of circulating levels of biomarkers of myocardial damage (troponin and BNP). On the other hand, TTS usually mimics an ACS and can be indistinguishable from it in patients with suspected ACS and normal coronary arteries on coronary angiography; therefore, an expert committee for TTS has proposed a diagnostic algorithm to help distinguish them.44
Tests used in patients with suspected TTS
ECG
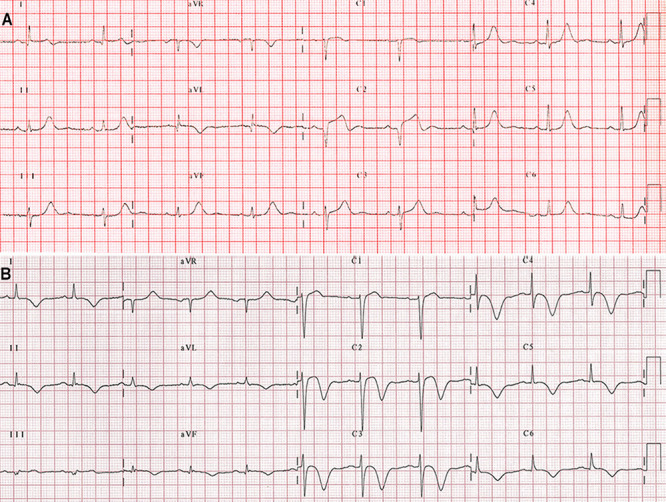
Most patients with TTS have abnormalities on ECG resembling ACS; mainly, ST-segment elevation, T-wave inversion, or both (figure 3).45,46 These abnormalities evolve over time with resolution of ST-segment elevation, when present, and are followed by T-wave inversion and QT-interval prolongation, and a subsequent gradual resolution of T-wave inversion, although it can persist for several months.47
Figure 3. A. A 12-lead electrocardiogram (ECG) in an 80-year-old woman with a focal atypical variant of Takotsubo syndrome showing sinus rhythm with ST-segment elevation of &1.0 mm in leads V1 and V3; 2.0 mm in lead V2 with a QS wave; T-wave inversions in leads D1 and AVL; and corrected QT-interval of 446 ms. B. ECG in a 68-year-old woman with a typical variant of Takotsubo syndrome showing a sinus rhythm with ST-segment elevation &2.0 mm in leads V1 and V2; T-wave inversions in leads D1, D2, AVL, V2-V6; positive T-wave in lead aVR, and prolongation of the corrected QT-interval of 491 ms.
Cardiac biomarkers
On admission to hospital, patients with TTS have elevation of myocardial injury biomarkers, such as creatine kinase-myocardial band isoenzyme (CK–MB), troponin and BNP.44 BNP concentration is higher in patients with TTS compared with those with AMI,3 and early BNP/troponin T, and BNP/CK-MB ratios help to differentiate TTS from AMI with greater accuracy than BNP alone.48 However, CK-MB is only mildly elevated in most patients with TTS.49
Echocardiography
Transthoracic echocardiography (TTE) is a quick, usually available, and very useful non-invasive diagnostic method in the diagnosis of TTS, allowing the visualisation of the regional wall motion abnormalities (RWMA) observed in the typical (figure 4B) and atypical variants of TTS, as well as the global function of the LV. Likewise, it is the diagnostic tool commonly used in following up the resolution of the RWMA of the LV; half of the patients have an early recovery with absence of RWMA within 10 days after the onset of TTS (figure 4F); the other half have a delayed recovery over about two months, and have a higher prevalence of in-hospital complications and higher mortality and should be monitored closely.50 TTE also allows cardiologists to diagnose involvement of the right ventricle (RV) in patients with TTS by detecting RWMA affecting the free wall and/ or apex and the dilation of the RV,51-53 and the detection of complications, such as dynamic LV outflow obstruction (LVOTO) and mitral regurgitation (figures 4C and 4D) caused by systolic anterior motion of the mitral leaflet (figure 4B),54-56 as well as thrombus formation in a dysfunctional LV apex.57,58
Figure 4. Two-dimensional transthoracic echocardiography (TTE) and cardiac magnetic resonance (CMR) imaging in a 57-year-old woman with a typical variant of Takotsubo syndrome with left ventricular outflow tract obstruction and mitral regurgitation (MR). Upper row: A. TTE, end-diastolic four-chamber view. B. TTE end-systolic image four-chamber view showing akinesis of the mid-apical segments of the left ventricle (LV) (yellow arrowheads) and systolic anterior motion (SAM) of the mitral valve (pink arrow). C. Colour Doppler imaging showing severe eccentric mitral regurgitation with a Coanda effect. D. Continuous-wave Doppler velocity showing a pattern of dynamic obstruction of the LV with a peak pressure gradient measured in the LV outflow tract at 20 mmHg. Middle row: Follow-up TTE. E. End-diastolic four-chamber view. F. End-systolic image four-chamber view showing normalisation of the LV contraction and the absence of the mitral valve SAM. G. Colour Doppler imaging showing trivial mitral regurgitation. Bottom row: CMR in a four-chamber view. H. End-diastolic image showing a small LV thrombus (red arrow). I. End-systolic image showing akinesis of the mid-apical segments of the LV (between yellow arrows), and the LV thrombus (red arrow). J. T2-weighted image showing a hyperintense signal representing oedema in the LV mid-apical and latero-apical segments (blue arrows) compared with the basal segment (green arrow). K. Late gadolinium-enhancement image showing absence of myocardial delayed contrast enhancement representing necrosis/fibrosis.
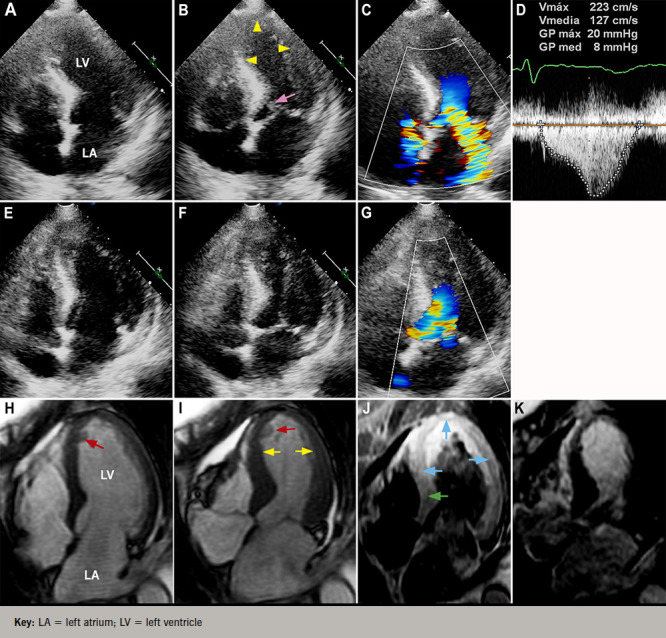
Key: LA = left atrium; LV = left ventricle
Coronary angiography and ventriculography
While electrocardiographic findings, cardiac biomarkers, and TTE are useful in the study of patients with TTS, coronary angiography is essential for the differential diagnosis of TTS from ACS. Most patients with TTS have completely normal coronary arteries, but some might have coronary artery disease that should not be considered as an exclusion criterion for TTS.4,10 Left ventriculography illustrates the characteristic wall motion abnormalities seen in the typical (figure 1B) and atypical forms of TTS.
CMR imaging
CMR is increasingly being used as a diagnostic tool in the evaluation of patients with suspected TTS to establish the diagnosis accurately, because it allows the cardiologist to visualise RWMA precisely (figure 4I), quantify global LV and RV functions, and indicate, not just the presence of myocardial oedema representing reversible myocardial injury (figure 4J), but, most importantly, the absence of delayed gadolinium hyperenhancement (figure 4K), allowing the differentiation of TTS from myocardial infarction and myocarditis diseases in which it is present.59,60 CMR is also vital to confirm the diagnosis of TTS in patients presenting with an ACS and with a history of an old myocardial infarction to ensure optimal treatment, as indicated previously.41 The international diagnostic criteria guidelines have recently recommended the use of CMR to exclude infectious myocarditis and confirm diagnosis of TTS.4
Prognosis
Even though TTS has a benign course, with full recovery within a matter of days to a few weeks, around 22% of patients will experience serious cardiac complications such as an ACS.4 According to their prevalence, they are classified as follows:
Frequent: acute heart failure (12-45%), LVOTO (10–25%) (figure 4D), mitral regurgitation (14–25%) (figure 4C), or cardiogenic shock (6–20%).
Moderate: atrial fibrillation (5–15%), LV-thrombus (2–8%) (figures 4H and 4I), cardiac arrest (4–6%), and atrioventricular block (5%).
Rare: tachya rrhythmia, bradyarrhythmia and torsade de pointes (2–5%), death (1–4.5%), ventricular tachycardia/fibrillation (˜3%), and acute ventricular septal defect (<1%).41
Regarding the recurrence of TTS, approximately 4–5% of patients who survive the initial event can have a recurrence from three weeks to as long as 4.7 years.61,62 The annual recurrence rate has been reported to vary between 1 and 3.5%.63,64
Treatment
Because most patients with TTS are hospitalised with a suspicion of ACS, they are initially treated according to the clinical guidelines for this disease,65 until the correct diagnosis of TTS is made.
To date, there are no specific or standardised treatments for patients with TTS based on randomised clinical trials,6 and because this is a temporary heart condition, the aim of treatment is to give supportive therapy and minimise complications. Most patients have an uneventful course requiring limited pharmacological therapies, such as the use of angiotensin-converting enzyme (ACE) inhibitors and angiotensin-receptor blockers (ARBs),3,63 beta blockers,44 and antiplatelet therapies,66 having a full recovery within a couple of weeks. Oral anticoagulation therapy for three months seems reasonable in patients with LV thrombi.58 Patients also need continuous ECG monitoring for at least 48 hours, because of the risk of serious cardiac arrhythmias, such as torsades de pointes, triggered by prolonged corrected QT-intervals.67,68 Patients complicated with acute pulmonary oedema, cardiogenic shock, and those recovering from cardiac arrest require intensive care.44
Patients with pulmonary oedema should be given diuretics and nitroglycerine intravenously, after excluding LVOTO in approximately 20% of patients, avoiding worsening of the pressure gradient. LVOTO can be diagnosed during ventriculography or by continuous-wave Doppler ultrasonography (figure 4D). In patients with hypotension without heart failure, clinicians should consider the administration of intravenous fluids, short-acting beta blockers, and, eventually, an LV assist device, e.g. an Impella pump. On the other hand, patients in cardiogenic shock must receive treatment for primary heart failure with catecholamines if LVOTO is not present, or levosimendan could be an alternative inotrope to catecholamines. Furthermore, because of the risk of intraventricular thrombus formation with risk of embolisation, anticoagulation with subcutaneous or intravenous heparin seems reasonable.44 As a long-term treatment, patients should receive ACE inhibitors or ARBs for at least one year to improve survival, but beta blockers are not beneficial.3 in approximately 20% of patients, avoiding worsening of the pressure gradient. LVOTO can be diagnosed during ventriculography or by continuous-wave Doppler ultrasonography (figure 4D). In patients with hypotension without heart failure, clinicians should consider the administration of intravenous fluids, short-acting beta blockers, and, eventually, an LV assist device, e.g. an Impella pump. On the other hand, patients in cardiogenic shock must receive treatment for primary heart failure with catecholamines if LVOTO is not present, or levosimendan could be an alternative inotrope to catecholamines. Furthermore, because of the risk of intraventricular thrombus formation with risk of embolisation, anticoagulation with subcutaneous or intravenous heparin seems reasonable.44 As a long-term treatment, patients should receive ACE inhibitors or ARBs for at least one year to improve survival, but beta blockers are not beneficial.3
Conclusion
TTS is an acute heart condition typically induced by emotional or physical stress, affecting mainly postmenopausal women. The exact pathophysiology of TTS remains incompletely understood; nonetheless, the hypothesis of involvement of a catecholamine surge is the most accepted, currently, specifically, involving an adrenergic cascade through the hypothalamic-pituitary-adrenal axis. It is characterised by transient RWMA of the LV and is clinically indistinguishable from AMI. In this scenario, CMR is essential to differentiate TTS from ACS and acute myocarditis accurately to ensure optimal management. Pharmacological therapies that have proven to be beneficial include the use of ACE inhibitors, ARBs, and antiplatelet therapies. The annual recurrence rate has been reported as 1–3.5%.
Key message
Takotsubo syndrome (TTS) is an acute heart condition typically induced by emotional or physical stress affecting mainly postmenopausal women and is clinically indistinguishable from acute myocardial infarction (AMI)
The exact pathophysiology of TTS remains incompletely understood; nonetheless, the hypothesis of involvement of a catecholamine surge is the most accepted one, currently
Cardiac magnetic resonance imaging is essential to accurately differentiate TTS from AMI and acute myocarditis, in order to ensure optimal management
Pharmacological therapies that have proven to be beneficial include the use of angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers, and antiplatelet therapies
Conflicts of Interest
None declared.
Editors’ note
See also the case reports on pages 35–6 and 37–8 of this issue.
Funding Statement
Funding None.
References
- 1.Sato TH, Uchida T, Dote K, Ishihara M. In: Clinical Aspect of Myocardial Injury: From Ischemia to Heart Failure. Kodama K, Haze K, Hori M, editors. Tokyo: Kagakuhyoronsha Publishing Co; 1990. Tako-tsubo-like left ventricular dysfunction due to multivessel coronary spasm; pp. 56–64. [Google Scholar]
- 2.Kurowski V, Kaiser A, von Hof K, et al. Apical and midventricular transient left ventricular dysfunction syndrome (tako-tsubo cardiomyopathy): frequency, mechanisms, and prognosis. Chest. 2007;132:809–816. doi: 10.1378/chest.07-0608. [DOI] [PubMed] [Google Scholar]
- 3.Templin C, Ghadri JR, Diekmann J, et al. Clinical features and outcomes of Takotsubo (stress) cardiomyopathy. N Engl J Med. 2015;373:929–938. doi: 10.1056/NEJMoa1406761. [DOI] [PubMed] [Google Scholar]
- 4.Ghadri JR, Wittstein IS, Prasad A, et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): clinical characteristics, diagnostic criteria, and pathophysiology. Eur Heart J. 2018;39:2032–2046. doi: 10.1093/eurheartj/ehy076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dias A, Nuñez Gil I J, Santoro F, et al. Takotsubo syndrome: state-of-the-art review by an expert panel – Part 1. Cardiovasc Revasc Med. 2019;20:70–79. doi: 10.1016/j.carrev.2018.11.015. [DOI] [PubMed] [Google Scholar]
- 6.Kato K, Lyon AR, Ghadri JR, Templin C. Takotsubo syndrome: aetiology, presentation and treatment. Heart. 2017;103:1461–1469. doi: 10.1136/heartjnl-2016-309783. [DOI] [PubMed] [Google Scholar]
- 7.Dawson DK. Acute stress-induced (takotsubo) cardiomyopathy. Heart. 2018;104:96–102. doi: 10.1136/heartjnl-2017-311579. [DOI] [PubMed] [Google Scholar]
- 8.Schneider B, Athanasiadis A, Stöllberger C, et al. Gender differences in the manifestation of tako-tsubo cardiomyopathy. Int J Cardiol. 2013;166:584–588. doi: 10.1016/j.ijcard.2011.11.027. [DOI] [PubMed] [Google Scholar]
- 9.Ito K, Sugihara H, Katoh S, Azuma A, Nakagawa M. Assessment of Takotsubo (ampulla) cardiomyopathy using 99mTc-tetrofosmin myocardial SPECT -comparison with acute coronary syndrome. Ann Nucl Med. 2003;17:115–122. doi: 10.1007/BF02988449. [DOI] [PubMed] [Google Scholar]
- 10.Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. 2008;155:408–417. doi: 10.1016/j.ahj.2007.11.008. [DOI] [PubMed] [Google Scholar]
- 11.Prasad A, Dangas G, Srinivasan M, et al. Incidence and angiographic characteristics of patients with apical ballooning syndrome (takotsubo/stress cardiomyopathy) in the HORIZONS-AMI trial: an analysis from a multicenter, international study of ST-elevation myocardial infarction. Catheter Cardiovasc Interv. 2014;83:343–348. doi: 10.1002/ccd.23441. [DOI] [PubMed] [Google Scholar]
- 12.Naegele M, Flammer AJ, Enseleit F, et al. Endothelial function and sympathetic nervous system activity in patients with Takotsubo syndrome. Int J Cardiol. 2016;224:226–230. doi: 10.1016/j.ijcard.2016.09.008. [DOI] [PubMed] [Google Scholar]
- 13.Citro R, d’Avenia M, De Marco M, et al. Polymorphisms of the antiapoptotic protein bag3 may play a role in the pathogenesis of tako-tsubo cardiomyopathy. Int J Cardiol. 2013;168:1663–1665. doi: 10.1016/j.ijcard.2013.03.050. [DOI] [PubMed] [Google Scholar]
- 14.Spinelli L, Trimarco V, Di Marino S, Marino M, Iaccarino G, Trimarco B. L41Q polymorphism of the G protein coupled receptor kinase 5 is associated with left ventricular apical ballooning syndrome. Eur J Heart Fail. 2010;12:13–16. doi: 10.1093/eurjhf/hfp173. [DOI] [PubMed] [Google Scholar]
- 15.Mattsson E, Saliba-Gustafsson P, Ehrenborg E, Tornvall P. Lack of genetic susceptibility in takotsubo cardiomyopathy: a case-control study. BMC Med Genet. 2018;19:39. doi: 10.1186/s12881-018-0544-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Eitel I, Moeller C, Munz M, et al. Genome-wide association study in takotsubo syndrome: preliminary results and future directions. Int J Cardiol. 2017;236:335–339. doi: 10.1016/j.ijcard.2017.01.093. [DOI] [PubMed] [Google Scholar]
- 17.Summers MR, Lennon RJ, Prasad A, et al. Pre-morbid psychiatric and cardiovascular diseases in apical ballooning syndrome (tako-tsubo/stress-induced cardiomyopathy): potential pre-disposing factors. J Am Coll Cardiol. 2010;55:700–701. doi: 10.1016/j.jacc.2009.10.031. https://doi.org/1016/j.jacc.2009.10.031 [DOI] [PubMed] [Google Scholar]
- 18.Delmas C, Lairez O, Mulin E, et al. Anxiodepressive disorders and chronic psychological stress are associated with Tako-Tsubo cardiomyopathy – new physiopathological hypothesis. Circ J. 2013;77:175–180. doi: 10.1253/circj.CJ-12-0759. [DOI] [PubMed] [Google Scholar]
- 19.Mausbach BT, Dimsdale JE, Ziegler MG, et al. Depressive symptoms predict norepinephrine response to a psychological stressor task in Alzheimer’s caregivers. Psychosom Med. 2005;67:638–642. doi: 10.1097/01.psy.0000173312.90148.97. [DOI] [PubMed] [Google Scholar]
- 20.Alvarenga ME, Richards JC, Lambert G, Esler MD. Psychophysiological mechanisms in panic disorder: a correlative analysis of noradrenaline spillover, neuronal noradrenaline reuptake, power spectral analysis of heart rate variability, and psychological variables. Psychosom Med. 2006;68:8–16. doi: 10.1097/01.psy.0000195872.00987.db. [DOI] [PubMed] [Google Scholar]
- 21.Finsterer J, Wahhbi K. CNS disease triggering Takotsubo stress cardiomyopathy. Int J Cardiol. 2014;177:322–329. doi: 10.1016/j.ijcard.2014.08.101. [DOI] [PubMed] [Google Scholar]
- 22.Scheitz JF, Mochmann HC, Witzenbichler B, Fiebach JB, Audebert HJ, Nolte CH. Takotsubo cardiomyopathy following ischemic stroke: a cause of troponin elevation. J Neurol. 2012;259:188–190. doi: 10.1007/s00415-011-6139-1. [DOI] [PubMed] [Google Scholar]
- 23.Inamasu J, Ganaha T, Nakae S, et al. Therapeutic outcomes for patients with aneurysmal subarachnoid hemorrhage complicated by Takotsubo cardiomyopathy. Acta Neurochir (Wien) 2016;158:885–893. doi: 10.1007/s00701-016-2768-6. [DOI] [PubMed] [Google Scholar]
- 24.Ghadri JR, Ruschitzka F, Luscher TF, Templin C. Takotsubo cardiomyopathy: still much more to learn. Heart. 2014;100:1804–1812. doi: 10.1136/heartjnl-2013-304691. [DOI] [PubMed] [Google Scholar]
- 25.Meyer P, Degrauwe S, Delden CV, Ghadri JR, Templin C. Typical takotsubo syndrome triggered by SARS-CoV-2 infection. Eur Heart J. 2020;41:1860. doi: 10.1093/eurheartj/ehaa306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Akashi Y, Nef H, Lyon A. Epidemiology and pathophysiology of Takotsubo syndrome. Nat Rev Cardiol. 2015;12:387–397. doi: 10.1038/nrcardio.2015.39. [DOI] [PubMed] [Google Scholar]
- 27.Pellicia F, Kaski JC, Crea F, Camici PG. Pathophysiology of Takotsubo syndrome. Circulation. 2017;135:2426–2441. doi: 10.1161/CIRCULATIONAHA.116.027121. [DOI] [PubMed] [Google Scholar]
- 28.Wittstein IS, Thiemann DR, Lima JAC, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005;353:539–548. doi: 10.1056/NEJMoa043046. [DOI] [PubMed] [Google Scholar]
- 29.Kume T, Akasaka T, Kawamoto T, et al. Assessment of coronary microcirculation in patients with Takotsubo-like left ventricular dysfunction. Circ J. 2005;69:934–939. doi: 10.1253/circj.69.934. [DOI] [PubMed] [Google Scholar]
- 30.Lyon AR, Rees PS, Prasad S, Poole-Wilson PA, Harding SE. Stress (Takotsubo) cardiomyopathy – a novel pathophysiological hypothesis to explain catecholamine-induced acute myocardial stunning. Nat Clin Pract Cardiovasc Med. 2008;5:22–29. doi: 10.1038/ncpcardio1066. [DOI] [PubMed] [Google Scholar]
- 31.Nef HM, Möllmann H, Kostin S, et al. Tako-Tsubo cardiomyopathy: intraindividual structural analysis in the acute phase and after functional recovery. Eur Heart J. 2007;28:2456–2464. doi: 10.1093/eurheartj/ehl570. [DOI] [PubMed] [Google Scholar]
- 32.Testa M, Feola M. Usefulness of myocardial positron emission tomography/nuclear imaging in Takotsubo cardiomyopathy. World J Radiol. 2014;6:502–506. doi: 10.4329/wjr.v6.i7.502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Vitale C, Rosano GM, Kaski JC. Role of coronary microvascular dysfunction in Takotsubo cardiomyopathy. Circ J. 2016;80:299–305. doi: 10.1253/circj.CJ-15-1364. [DOI] [PubMed] [Google Scholar]
- 34.Crea F, Camici PG, Bairey Merz CN. Coronary microvascular dysfunction: an update. Eur Heart J. 2014;35:1101–1111. doi: 10.1093/eurheartj/eht513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Luscher TF, Templin C. Is takotsubo syndrome a microvascular acute coronary syndrome? Towards a new definition. Eur Heart J. 2016;37:2816–2820. doi: 10.1093/eurheartj/ehw057. [DOI] [PubMed] [Google Scholar]
- 36.Ghadri JR, Cammann VL, Napp LC, et al. International Takotsubo Registry Differences in the clinical profile and outcomes of typical and atypical Takotsubo syndrome: data from the International Takotsubo Registry. JAMA Cardiol. 2016;1:335–340. doi: 10.1001/jamacardio.2016.0225. [DOI] [PubMed] [Google Scholar]
- 37.Medina de Chazal H, Del Buono MG, Keyser-Marcus L, et al. Stress cardiomyopathy diagnosis and treatment: JACC state-of-the-art review. J Am Coll Cardiol. 2018;72:1955–1971. doi: 10.1016/j.jacc.2018.07.072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ghadri JR, Camman VL, Jurisic S, et al. A novel clinical score (InterTAK Diagnostic Score) to differentiate takotsubo syndrome from acute coronary syndrome: results from the International Takotsubo Registry. Eur J Heart Fail. 2017;19:1036–1042. doi: 10.1002/ejhf.683. [DOI] [PubMed] [Google Scholar]
- 39.Lyon AR, Bossone E, Schneider B, et al. Current state of knowledge on Takotsubo syndrome: a position statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2016;18:8–27. doi: 10.1002/ejhf.424. [DOI] [PubMed] [Google Scholar]
- 40.Gandhi H, Rodriguez JE, Reynolds H. Takotsubo cardiomyopathy versus apical infarction in patients with myocardial infarction and non-obstructive coronary artery disease (MINOCA) J Am Coll Cardiol. 2017;69:270. doi: 10.1016/S0735-1097(17)33659-8. [DOI] [Google Scholar]
- 41.Díaz-Navarro, Villagran F. Takotsubo cardiomyopathy and coronary artery disease: value of cardiac magnetic resonance imaging for diagnostic confirmation: a case report. Eur Heart J Case Rep. 2018;3:yty151. doi: 10.1093/ehjcr/yty151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Eitel I, Behrendt F, Schindler K, et al. Differential diagnosis of suspected apical ballooning syndrome using contrast-enhanced magnetic resonance imaging. Eur Heart J. 2008;29:2651–2659. doi: 10.1093/eurheartj/ehn433. [DOI] [PubMed] [Google Scholar]
- 43.Bratis K. Cardiac magnetic resonance in Takotsubo syndrome. Eur Cardiol. 2017;1:58–62. doi: 10.15420/ecr.2017:7:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Ghadri JR, Wittstein IS, Sharkey S, et al. International Expert Consensus Document on Takotsubo syndrome (Part II): diagnostic workup, outcome, and management. Eur Heart J. 2018;39:2047–2062. doi: 10.1093/eurheartj/ehy077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or Takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006;27:1523–1529. doi: 10.1093/eurheartj/ehl032. [DOI] [PubMed] [Google Scholar]
- 46.Frangieh AH, Obeid S, Ghadri JR, et al. ECG criteria to differentiate between Takotsubo (stress) cardiomyopathy and myocardial infarction. J Am Heart Assoc. 2016;5:e003418. doi: 10.1161/JAHA.116.003418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kosuge M, Kimura K. Electrocardiographic findings of Takotsubo cardiomyopathy as compared with those of anterior acute myocardial infarction. J Electrocardiol. 2014;47:684–689. doi: 10.1016/j.jelectrocard.2014.03.004. [DOI] [PubMed] [Google Scholar]
- 48.Randhawa MS, Dhillon AS, Taylor HC, Sun Z, Desai MY. Diagnostic utility of cardiac biomarkers in discriminating takotsubo cardiomyopathy from acute myocardial infarction. J Card Fail. 2014;20:2–8. doi: 10.1016/j.cardfail.2013.12.004. [DOI] [PubMed] [Google Scholar]
- 49.Kurisu S, Kihara Y. Tako-tsubo cardiomyopathy: clinical presentation and underlying mechanism. J Cardiol. 2012;60:429–437. doi: 10.1016/j.jjcc.2012.06.015. [DOI] [PubMed] [Google Scholar]
- 50.Jurisic S, Camman VL, Kato K, et al. Clinical predictors and prognostic impact of recovery of wall motion abnormalities in Takotsubo syndrome: results from the International Takotsubo Registry. J Am Heart Assoc. 2019;8:e011194. doi: 10.1161/JAHA.118.011194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Haghi D, Athanasiadis A, Papavassiliu T, et al. Right ventricular involvement in Takotsubo cardiomyopathy. Eur Heart J. 2006;27:2433–2439. doi: 10.1093/eurheartj/ehl274. [DOI] [PubMed] [Google Scholar]
- 52.Heggemann F, Hamm K, Brade J, et al. Right ventricular function quantification in Takotsubo cardiomyopathy using two-dimensional strain echocardiography. PLoS One. 2014;9:e103717. doi: 10.1371/journal.pone.0103717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Kagiyama N, Okura H, Kume T, Hayashida A, Yoshida K. Isolated right ventricular takotsubo cardiomyopathy. Eur Heart J Cardiovasc Imaging. 2015;16:285. doi: 10.1093/ehjci/jeu207. [DOI] [PubMed] [Google Scholar]
- 54.Liang J, Janish C, Bishu K, Reeder G. Dynamic left ventricular outflow tract obstruction in apical ballooning syndrome (Takotsubo cardiomyopathy) Perfusion. 2014;30:82–84. doi: 10.1177/0267659114536584. [DOI] [PubMed] [Google Scholar]
- 55.Bouabdallaoui N, Wang Z, Lecomte M, Ennezat PV, Blanchard D. Acute mitral regurgitation in Takotsubo cardiomyopathy. Eur Heart J Acute Cardiovasc Care. 2015;4:197–199. doi: 10.1177/2048872614521764. [DOI] [PubMed] [Google Scholar]
- 56.Izumo M, Akashi YJ. Role of echocardiography for takotsubo cardiomyopathy: clinical and prognostic implications. Cardiovasc Diagn Ther. 2018;8:90–100. doi: 10.21037/cdt.2017.07.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Haghi D, Papavassiliu T, Heggemann F, Kaden JJ, Borggrefe M, Suselbeck T. Incidence and clinical significance of left ventricular thrombus in Tako-Tsubo cardiomyopathy assessed with echocardiography. QJM. 2008;101:381–386. doi: 10.1093/qjmed/hcn017. [DOI] [PubMed] [Google Scholar]
- 58.Santoro F, Stiermaier T, Tarantino N, et al. Left centricular thrombi in Takotsubo syndrome: incidence, predictors, and management. Results from the GEIST (German Italian Stress Cardiomyopathy) registry. J Am Heart Assoc. 2017;6:e006990. doi: 10.1161/JAHA.117.006990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Kohan AA, Levy Yeyati E, De Stefano L, et al. Usefulness of MRI in takotsubo cardiomyopathy: a review of the literature. Cardiovasc Diagn Ther. 2014;4:138–146. doi: 10.3978/j.issn.2223-3652.2013.10.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Abbas A, Sonnex E, Pereira RS, Coulden RA. Cardiac magnetic resonance assessment of takotsubo cardiomyopathy. Clin Radiol. 2016;71:e110–e119. doi: 10.1016/j.crad.2015.10.020. [DOI] [PubMed] [Google Scholar]
- 61.Sharkey SW, Windenburg DC, Lesser JR, et al. Natural history and expansive clinical profile of stress (Tako-Tsubo) cardiomyopathy. J Am Coll Cardiol. 2010;55:333–341. doi: 10.1016/j.jacc.2009.08.057. [DOI] [PubMed] [Google Scholar]
- 62.El-Battrawy I, Santoro F, Stiermaier T, et al. Incidence and clinical impact of recurrent Takotsubo syndrome: results from the GEIST registry. J Am Heart Assoc. 2019;8:e010753. doi: 10.1161/JAHA.118.010753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Singh K, Carson K, Usmani Z, Sawhney G, Shah R, Horowitz J. Systematic review and meta-analysis of incidence and correlates of recurrence of Takotsubo cardiomyopathy. Int J Cardiol. 2014;174:696–701. doi: 10.1016/j.ijcard.2014.04.221. [DOI] [PubMed] [Google Scholar]
- 64.Campos FAD, Ritt LEF, Costa JPS, et al. Factors associated with recurrence in Takotsubo syndrome: a systematic review. Arq Bras Cardiol. 2020;14:477–483. doi: 10.36660/abc.20180377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2018;39:119–177. doi: 10.1093/eurheartj/ehx393. [DOI] [PubMed] [Google Scholar]
- 66.Dias A, Franco E, Koshkelashvili N, et al. Antiplatelet therapy in Takotsubo cardiomyopathy: does it improve cardiovascular outcomes during index event. Heart Vessels. 2016;31:1285–1290. doi: 10.1007/s00380-015-0729-2. [DOI] [PubMed] [Google Scholar]
- 67.Syed FF, Asirvatham SJ, Francis J. Arrhythmia occurrence with takotsubo cardiomyopathy: a literature review. Europace. 2010;13:780–788. doi: 10.1093/europace/euq435. [DOI] [PubMed] [Google Scholar]
- 68.Brown KH, Trohman RG, Madias C. Arrhythmias in Takotsubo cardiomyopathy. Card Electrophysiol Clin. 2015;7:331–340. doi: 10.1016/j.ccep.2015.03.015. [DOI] [PubMed] [Google Scholar]