
Figure 3 |. Histological characteristics of the transition from acute kidney injury (AKI) to chronic kidney disease (CKD).
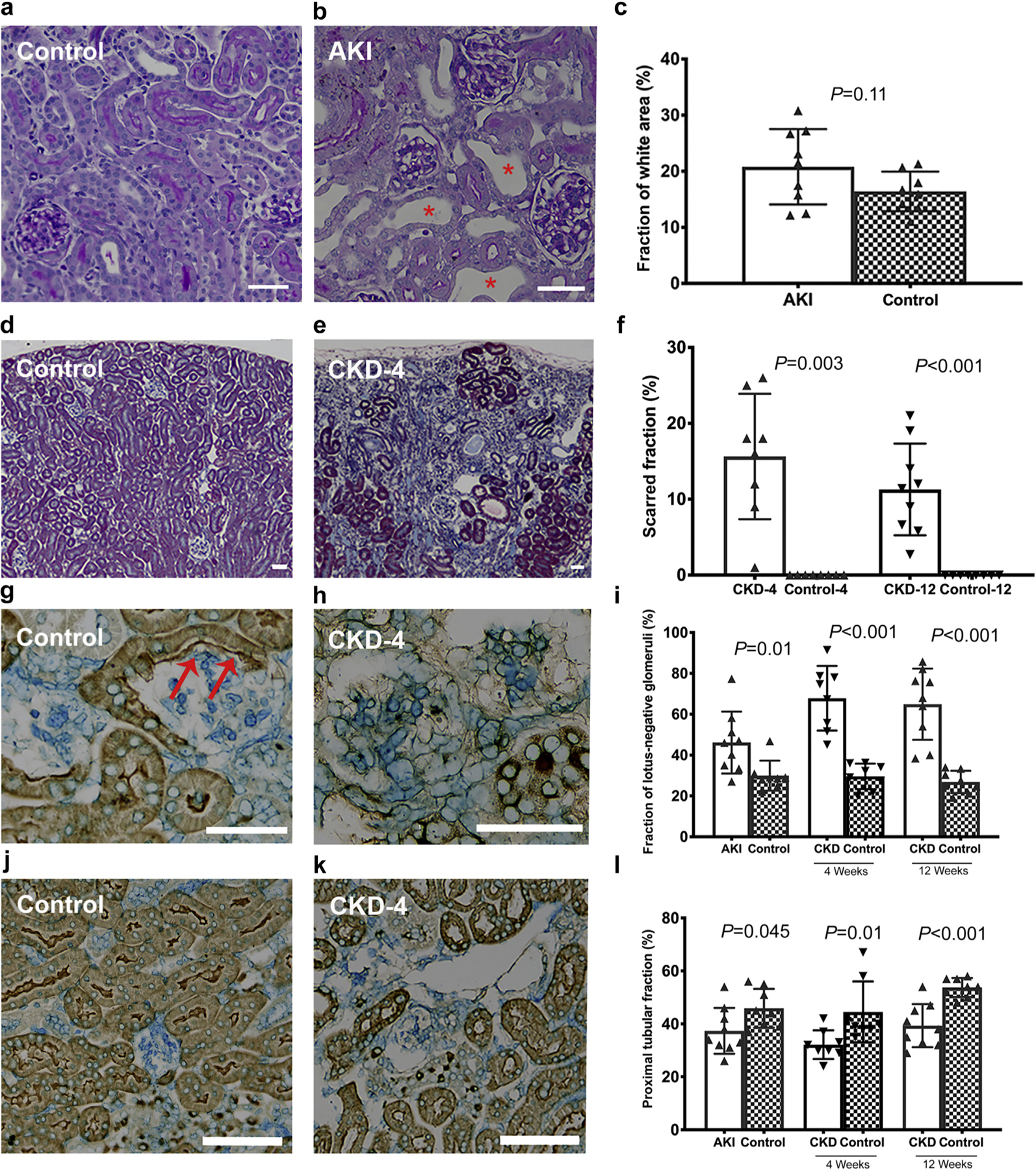
(a,b) Representative tubular dilation in AKI group compared with the controls, where areas of tubular dilation were frequent in the AKI group (b; red *). (c) The quantification of the percentage of white space. Scarred area (d–f) was assessed by trichrome stain in the CKD-4 and CKD-12 groups. (e) The kidneys in the CKD-4 and CKD-12 groups were smaller and had cortical wedge-shaped lesions. These scarred areas contained many atrophic tubules and lotus-negative glomeruli (h). (g–i) Lotus-negative glomeruli and (j–l) proximal tubular fraction were assessed on lotus lectin stained kidneys. (g) A healthy glomerulus in a control animal where the glomerulus is connected to the tubule. The red arrows highlight the parietal cells marked as lotus-positive signifying an intact glomerulotubular junction. (j–l) Proximal tubular content was reduced in the CKD-12 group. Bars in the histologic sections = 50 μm. P values < 0.002 are considered significant. CKD-4, CKD 4 weeks after injury; CKD-12, CKD 12 weeks after injury. To optimize viewing of this image, please see the online version of this article at www.kidney-international.org.