

Abstract
Cervical carcinosarcoma (CCS) is a rare aggressive tumor which was referred to as a sarcoma initially with its morbidity less than 1% of all cervical cancers. Four theories have been proposed for the pathogenesis of CCS. The “metaplastic theory,” also called “monoclonal theory,” has been widely accepted so far. The most common clinical symptom of CCS is abnormal vaginal bleeding. CCS is much less common than the counterparts in uterine corpus and usually confused with uterine carcinosarcoma (UCS) or common cervical cancer. The management for CCS has been mainly extrapolated from studies of UCS or cervical cancers. However, CCS has its special anatomical position and biological behaviors and is usually diagnosed at an early stage than UCS. Currently, there is no consensus on the survival, management and prognosis factors of CCS. We reviewed and summarized the literatures regarding to the epidemiology, clinical presentations, pathogenesis, diagnosis and treatment of CCS for providing clinicians with comprehensive information to diagnose and treat this malignancy.
Keywords: Cervical carcinosarcoma, uterine carcinosarcoma, immunohistochemistry, treatment
Introduction
Gynecological carcinosarcoma (GCS), also known as malignant mixed mesodermal tumor or malignant mixed Müllerian tumor (MMMT), is heterogeneous and extremely aggressive malignancy that predominantly appears in the uterine corpus, then in the ovary, uterine cervix, vagina, fallopian tubes and peritoneum. 1 The morbidity (less than 0.005% of all cervical cancers) of cervical carcinosarcoma (CCS) is much less than that of uterine body 2 and CCS commonly occurs in the postmenopausal women. Compared to cervical squamous cell carcinoma and adenocarcinoma, primary CCS has a worse outcome because it is prone to metastasis and recurrence. 3
CCS, a biphasic neoplasm, which has been regarded as sarcoma previously, is histologically comprises both epithelial and mesenchymal structures. 4 The metaplastic carcinoma theory that the carcinomatous element is the primary force of tumor invasiveness has been widely accepted. 5 CCS is commonly confused with uterine carcinosarcoma, and is easily misdiagnosed as cervical cancers/sarcomas. However, its histological presentations, biologic behavior and outcome is different from these malignancies. 6 Until now, the management for CCS has been mainly extrapolated from studies of uterine carcinosarcoma or cervical sarcomas, but they should not be treated in the similar way.
Most related reports published previously were case reports or case series, and no consensus has been reached on the optimal management, prognostic factors, and survival of CCS. 3 Therefore, we reviewed published literatures to summarize epidemiology, pathogenesis, clinical presentations, diagnosis, treatments, and prognostic factors of CCS with the aim to provide clinicians with accurately diagnosis and therapy.
Method
We reviewed the literature for studies on CCS by using PubMed/EMBASE/Web of Science. We used the keywords included “cervical carcinosarcoma,” “carcinosarcoma of the uterine cervix,” “cervical malignant mixed Müllerian tumor,” “malignant mixed Müllerian tumor of uterine cervix,” and “cervical malignant mesodermal mixed tumor” respectively. Previous review articles, papers and case reports were included. Language restrictions were not used. We also searched for clinical trials, and abstracts of scientific meetings. Publications from January 1, 1966 to October 1, 2020 were qualified for inclusion.
Epidemiology
CCS accounts for nearly half of cervical sarcoma, with the recurrence rate less than 1% of all cervical malignancies. 7 In Europe, the incidence of CCS is 0.2 cases per 100,000 population. 8 The age of initial diagnosis of CCS ranges from 12 to 94 and the vast majority of patients occurred in postmenopausal.3,9-11 Black patients seem to be more likely to suffer from CCS.3,9
Pelvic radiotherapy, chemotherapy history and HPV infection in particular 16 type are at high risk of developing CCS.10,12-14 One patient who received pelvic radiation therapy 12 years ago with the purpose of treating cervical squamous cell carcinoma was eventually diagnosed with CCS. 12 Another patient was reported to confirm with CCS after the cessation of cyclophosphamide therapy. 13 CCS also occurred in the lower remaining uterine segment and cervix after subtotal hysterectomy. 15 In addition, some studies have documented the integration of high-risk HPV in both epithelial and mesenchymal components of CCS, although the role of HPV in the evolution of CCS needs further exploration. 10
Pathogenesis
The pathogenesis of CCS remains unclear and may be associated with the following four theories. The collision theory postulates that tumors stem from two different but synchronous neoplastic cell populations, respectively.16,17 The combination theory supports both neoplastic cell populations originate from a common stem cell. The composition theory infers that paracrine factors generated from the carcinomatous structure induce proliferative response of mesenchymal components and it has been denied in daily practice as the sarcomatous component shows the histological features of malignancy. 18 However, some recent molecular and immunological findings sustain the metaplastic carcinoma theory that CCS may stem from the carcinomatous elements and then differentiate into sarcoma components.19-24 The coexistence of CCS and cervical squamous cell carcinoma also support the metaplastic carcinoma theory.10,14,25
Clinical Presentations
The initial symptoms of CCS are similar to cervical cancer, mainly including abnormal vaginal spotting/bleeding and watery vaginal discharge. These presentations are easily to be detected by patients in the early stage. Some cases also complain of non-specific symptoms like lower abdominal pain, abdominal swelling, increased abdominal girth, loss of weight and gradual weakness. 3 A polyploid mass in the cervix or even a large necrotic or/and hemorrhagic lump replacing the cervix could be discovered after vaginal exploration. Early metastasis in CCS commonly occurs in vagina, rectum, bladder and bones. 15
Diagnosis
Clinical manifestations, physical examination especially vaginal exploration, laboratory tests, ultrasound, imaging features and pathology are conducted to diagnose CCS. As no explicit staging system is available for CCS, most cases reported are staged based on the International Federation of Gynecology and Obstetrics (FIGO) surgical staging of cancer of the cervix uteri.26-28
The complete blood count, serum biochemical data and tumor biomarkers such as carbohydrate antigen 19-9 (CA19-9), carbohydrate antigen 15-3 (CA15-3), carbohydrate antigen 72-4 (CA72-4), are usually unremarkable.1,29 Notably, the elevated serum level of carbohydrate antigen 125 (CA125) and carcinoembryonic antigen (CEA) could be observed in some cases.24,29-31 CCS usually presents as a polypoid or bulky mass in cervix on ultrasound. 1 Computed tomography (CT) or magnetic resonance imaging (MRI) is used to detect a heterogeneous abdominopelvic mass and to check whether the mass is confined to the cervix and/or invaded to the vaginal wall.26,29,31 PET-CT is sometimes available to assure extrauterine metastasis in patients with CCS.11,32,33
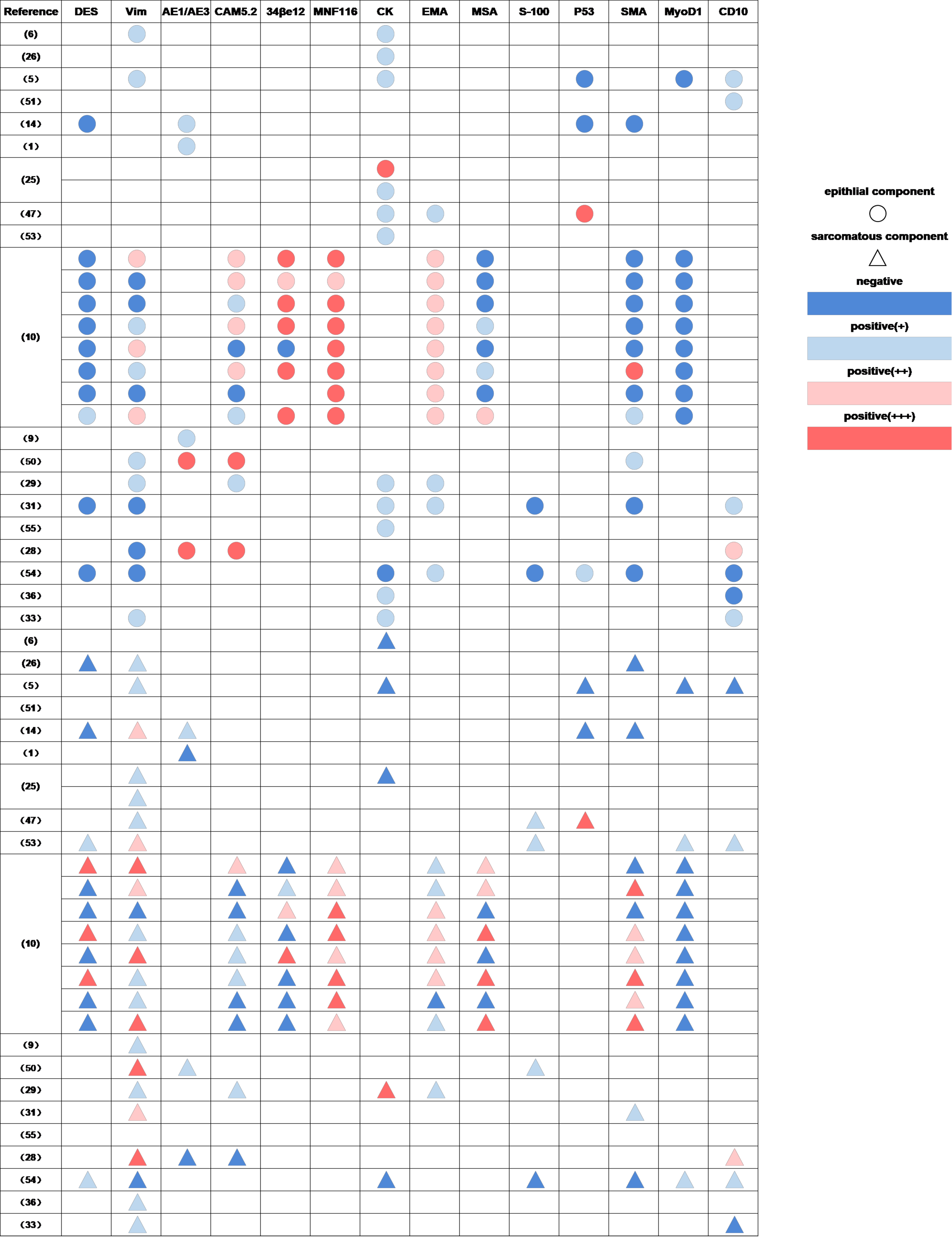
The gold standard of diagnosing CCS is pathological examination. As the accessibility of the uterine cervix, cervical biopsy examination is easy performed and can bring a definite diagnosis of CCS.4,34 Grossly, most CCS cases invade mucosal and even full-thickness, in some rare cases, the uterine cervical mucosal were intact. Histologically, CCS is characterized as a biphasic admixture of intimately juxtaposed carcinomatous and sarcomatous components. The malignant epithelial components usually presents with squamous cell carcinoma (SCC), adenocarcinoma, adeno-squamous carcinoma, basaloid carcinoma, of which SCC and adenocarcinoma account for the most.10,29 The mesenchymal components, either homologous (gynecologic tissue) or heterologous (represented by osteosarcomatous components), predominantly presents as long, spindle cell element. 29 Immunohistochemistry (IHC) displays that the epithelial elements mainly express cytokeratin (CK), broad-spectrum cytokeratin marker (MNF-116), low-molecular-weight cytokeratin marker (CAM 5.2), high-molecular-weight cytokeratin marker (34βE12) and epithelial membrane antigen (EMA), whereas the sarcoma components always express vimentin, desmin, smooth muscle-specific actin (SMA) and muscle-specific actin (MSA). Notably, sarcomatous components can express MNF-116, EMA and epithelial components are immunoreactive for vimentin likewise (Supplementary Figure 1). Meanwhile, IHC is irreplaceable in the classification of heterologous elements. 24 The previous reports showed that the cellular proliferation index (based on Ki-67 immunostaining) was significantly higher in carcinomatous components in contrast with sarcomatous components (mean of 70% and 28% of cells positive, respectively). 35 However, the pathological features of CCS have not been well characterized. Misdiagnosis of CCS sometimes happens in cervical samples because the sarcomatous components are hard to be identified.9,31 A meta-analysis showed that the accurate diagnosis rate of CCS by preoperative pathology was only around 56%, and CCS was easy to be misdiagnosed as purely epithelial carcinoma. 11 Previous studies identified four molecular subtypes as microsatellite instability, POLE-mutated, copy number low, and copy number high subtypes in gynecologic carcinosarcoma (CS) and linked these genomic instability types with the clinicopathological features of gynecologic CS such as tumor histology, stage, therapy and patient prognosis. 36
Treatment
There is no evidence-based guideline on optimal treatment approaches for CCS patients given its rarity. 33 Treatment has given priority to surgery. For early-stage CCS patients, surgery combined with adjuvant radiotherapy with or without chemotherapy, is associated with an improved disease-free survival (DFS) and overall survival(OS). 11 Radiotherapy is commonly recommended to locally advanced-stage CCS patients11,31,37 while chemotherapy is usually conducted in metastatic CCS patients. 31 Recently, one advanced CCS patient with high TMB, negative for programmed cell death protein 1 expression, microsatellite instability stable, and mutations in POLE received cryoablation followed by pembrolizumab and achieved a complete response and a progression-free survival over 11 months. No treatment-related adverse reactions were reported to this patient. Therefore, cryoablation subsequent with immunotherapy may be an optional choice for TMB-high patients with CCS. 38 It is frustrating that target therapy has not been reported in CCS patients until now and prospective trial regarding to the therapy of CCS has not been found.
Surgery
Surgery including total abdominal hysterectomy, bilateral salpingo-oophorectomy with pelvic lymph node dissection (radical surgery) and excision of cervical mass (cytoreduction), is primarily performed in patients with local CCS.4,11 Radical surgery is the strongest recommendation for IB stage (Based on the FIGO surgical staging) patients, who account for nearly half of all CCS patients. 11 While cytoreduction is commonly conducted in advanced patients for relieving symptoms or in early-stage patients who is unable to receive radical surgery. 34 Notably, the absence of cervical mucosal involvement lead to tumor-progression in a silent fashion without vaginal bleeding and eventually the increasing volume of the tumor cause unpredictable tumor rupture. Under such emergency circumstance, surgery is immediately needed. 30 Fifty-four patients with CCS were reviewed from published case reports/series and 48 of them have been reported to suffer from surgery. Among these 48 patients, over half of cases who were diagnosed with FIGO stage I mainly received radical surgery (Table 1).
Table 1.
Published case reports and case series regarding to CCS.
| Reference | Age | CCS type | clinical presentation | FIGO stage | Surgery | RT and CT | Survival (mos.) | |
|---|---|---|---|---|---|---|---|---|
| Dead alive | ||||||||
| Rodriguez-Escudero et al 41 | 12 | Heterologous | Vaginal bleeding | I | H; BSO; LND | RT | NR | NR |
| Maheshwari et al 31 | 60 | Homologous | Lower abdominal pain | I | H; BSO | RT 60 Gy | NR | 22 |
| Abidi et al 42 | 68 | NR | NR | I | RH; BSO; PLNDLND | RT | NR | 18 |
| Wang et al. 43 | 36 | Homologous | Vaginal bleeding | I | H; BSO; PLNDLND | CT | NR | NR |
| Waxman et al 51 | 76 | NR | Vaginal bleeding; cervical mass | IB | ECM; USO | VS + ADM + CTX | NR | 9 |
| Clement et al 34 | 45 | Heterologous | Vaginal bleeding; cervical mass | IB | H; BSO;PLND | CT; RT | 156 | NR |
| 23 | Heterologous | Vaginal bleeding | IB | ECM | RT | NR | NR | |
| 66 | Homologous | Vaginal bleeding; abnormal pap smear | IB | H; BSO | NR | NR | NR | |
| 61 | Homologous | Vaginal bleeding; abnormal pap smear; cervical mass | IB | H; BSO;PLND | NR | NR | 54 | |
| 70 | Homologous | Abnormal pap smear; cervical mass | IB | H; BSO;PLND | NR | NR | NR | |
| 78 | Homologous | Cervical mass | IB | H; BSO; PALND | RT | NR | NR | |
| 84 | Homologous | Vaginal bleeding; cervical mass | IB | H; BSO;PLND | NR | NR | NR | |
| Gan et al 44 | 56 | Homologous | Vaginal bleeding | IB | RH; BSO; PLNDLND/PALND | NR | NR | 24 |
| Miyazawa and Hernandez 45 | 46 | Heterologous | Vaginal bleeding | IB1 | RH; BSO;PLND | RT | NR | 30 |
| Iida et al 29 | 61 | Heterologous | Vaginal bleeding | IB1 | SRH; BSO;PLND | PRT 45Gy | 17 | NR |
| Sharma et al 4 | 29 | Homologous | Abnormal pap smear | IB1 | RH; PLNDND | NR | NR | 65 |
| 66 | Homologous | Vaginal bleeding | IB1 | RH; BSO;PLND/PALND | RT 45 Gy | NR | 35 | |
| Piura et al 52 | 76 | NR | Vaginal bleeding | IB1 | H; BSO;PLND | RT 50.4 Gy | NR | 15 |
| Kadota et al 46 | 61 | Heterologous | NR | IB1 | H; BSO;PLND | TAX + CBP RT 50.4Gy |
NR | 70 |
| Lopez-Chardi et al 47 | 80 | Homologous | Vaginal bleeding | IB1 | H; BSO | RT | NR | 31 |
| Munakata et al 53 | 43 | Heterologous | Cervical mass | IB1 | RH; ND | DDP;RT 40 Gy | NR | 38 |
| Lin et al 1 | 65 | Homologous | Vaginal bleeding | IB1 | RH; BSO;PLND | None | NR | 26 |
| Kimyon Comert et al 11 | 67 | Homologous | Lower abdominal pain | IB1 | RH; BSO;PLND/PALND | DDP; RT | NR | 60 |
| Young et al 6 | 53 | Homologous | Vaginal bleeding; lower abdominal pain | IB2 | RH; BSO;omentectomy | RT 45 Gy | NR | NR |
| Sharma et al 4 | 64 | Homologous | Vaginal bleeding | IB2 | NR | RT 45 Gy | 28 | NR |
| 25 | Homologous | Vaginal bleeding; vaginal discharge | IB2 | RH; PLNDND | None | NR | 42 | |
| Laterza et al 25 | 42 | Homologous | Vaginal bleeding | IB2 | H; BSO;PLND | IFO + DDP | NR | 48 |
| Lee et al 48 | 47 | Heterologous | Vaginal bleeding | IB2 | RH; BSO;PLND | CT; T | NR | 20 |
| Luo et al 14 | 45 | Homologous | Vaginal bleeding | IB2 | TH; BSO;PLND/PALND | CT; RT | NR | NR |
| Kim et al 37 | 53 | NR | Cervical mass | IB2 | RH; BSO;PLND | IFO + DDP TAX + CBP |
12 | NR |
| Connor 54 | 64 | NR | Vaginal bleeding; vaginal discharge | II | NR | PRT + BRT 65.5 Gy | 2.5 | NR |
| Wang et al 43 | 42 | Homologous | Vaginal bleeding | II | H; BSO;PLND | RT | NR | 82 |
| Meguro et al 28 | 63 | Homologous | Vaginal bleeding | IIA | RH; BSO;PLND | CT | NR | NR |
| Kimyon Comert et al 11 | 68 | Homologous | Abnormal pap smear | IIA1 | RH; BSO;PLND/PALND | DDP; RT | NR | NR |
| Clement et al 34 | 87 | Homologous | Abnormal pap smear; cervical mass | IIB | ECM | RT | NR | NR |
| Laterza et al 25 | 74 | Homologous | Vaginal bleeding | IIB | RH; BSO;PLND/PALND | RT 65Gy | 11 | NR |
| Gan et al 44 | 63 | Homologous | Vaginal bleeding;vaginal discharge | IIB | RH; BSO; PLNDLND/PALND | RT | NR | NR |
| 58 | Homologous | Vaginal bleeding | IIB | RH; BSO; PLNDLND/PALND | RT | NR | NR | |
| Semczuk et al 5 | 57 | Homologous | Vaginal bleeding | IIB | TH; BSO;PLND/PALND omentectomy | CTX + ADM | NR | 7 |
| Gastrell et al 26 | 68 | Homologous | Vaginal bleeding | IIIB | NR | DDP; RT 45Gy | NR | 6 |
| Tseng et al 30 | 59 | NR | Lower abdominal pain | IIIB | H; BSO;PLND omentectomy |
ADM + DDP RT 50.4 Gy |
NR | 4 |
| Bagué et al 27 | 62 | Heterologous | NR | IVB | H; BSO | CT; T | NR | 39 |
| Sharma et al 4 | 64 | Homologous | Vaginal bleeding | IVB | NR | IFO; RT 50 Gy | 5 | NR |
| Abell and Ramirez 12 | 68 | NR | Vaginal bleeding | NR | ECM | RT | 15 | NR |
| 44 | NR | Vaginal discharge | NR | RH; cystectomy; vaginectomy | None | 13 | NR | |
| 72 | NR | Vaginal bleeding | NR | NR | RT | 10 | NR | |
| 65 | NR | Vaginal bleeding | NR | ECM | RT | 10 | NR | |
| 70 | NR | Vaginal discharge | NR | NR | RT | 3 | NR | |
| 47 | NR | Vaginal discharge | NR | ECM | RT | 13 | NR | |
| Clement et al 34 | 71 | Homologous | Cervical mass | NR | ECM; PLND | CT; RT | NR | NR |
| Takeshima et al 49 | 84 | NR | Cervical mass | NR | H; BSO | CT; RT | NR | NR |
| Ribeiro-Silva et al 9 | 71 | Homologous | Vaginal bleeding | NR | H; BSO | CT | NR | 12 |
| Wu et al 32 | 25 | NR | NR | NR | RH | CT; RT | NR | NR |
| Roma 50 | 65 | NR | Vaginal bleeding | NR | H; BSO | CT | NR | NR |
| Ribeiro et al 33 | 64 | NR | Vaginal bleeding | NR | RH; BSO;LND; omentectomy | TAX + CBP; RT | 5 | NR |
Abbreviations: ADM, adriamycin; CBP, carboplatin; CCS, cervical carcinosarcoma; CT, chemotherapy; CTX, cyclophosphamide; DDP, cisplatin; ECM, excision of cervical mass; FIGO, Federation of Gynecology and Obstetrics; H, hysterectomy; IFO, Ifosfamide; LND, lymph node dissection; NR, not reported; PLND/PALND, pelvic/para-aortic lymph node dissection; RH, radical hysterectomy; RT, radiotherapy; SRH, semi-radical hysterectomy; TAX, paclitaxel; TH, total hysterectomy; USO/BSO, unilateral/bilateral salpingo-oophorectomy; VS, vincristine sulfate.
Radiotherapy
Although radiotherapy has been provided in patients of CCS, its impact on survival is uncertain. Pelvic radiation and brachytherapy are carried out for patients with CCS and the former was preferable according to the reported cases.25,26,31 Of all collected cases (n = 54), 38 patients received radiotherapy at the variable dose ranging from 40 Gy to 65.5 Gy. Significantly, 32 of them accepted both surgery and radiation, which indicated that radiotherapy was adjuvant treatment option (Table 1). In a review conducted by Kimyon Comert G et al, surgery combined with adjuvant radiotherapy was expressively associated with an improved DFS and OS compared with radiotherapy alone in CCS patients. 11
Chemotherapy
Data on chemotherapy of CCS is finite, mainly from studies of cervical cancer and standard chemotherapy regimens of CCS is still unclear. 25 Cisplatin, doxorubicin, ifosphamide and cyclophosphamide are commonly recommended for metastatic patients with CCS. 31 We collected various chemotherapy regimens conducted on 23 patients of CCS from published reports: Ten patients with FIGO stage I received adjuvant chemotherapy (half of them with platinum-based regimens) following standard surgery and the clinical outcomes of these ten patients were gratifying. Seven patients diagnosed with local advanced stage were treated with the first-line chemotherapy regimens as ifosfamide, cisplatin, adriamycin combined with radiotherapy and their survivals are mixed. One CCS patient with stage IB2 received radical surgery followed by chemotherapy of ifosfamide plus cisplatin. She developed recurrence seven months after surgery and underwent 2 courses of the 2nd line chemotherapy of paclitaxel in combination with carboplatin, then died (Table 1). Obviously, platinum-based chemotherapy regimens were in the majority. However, the effectiveness of chemotherapeutic agents above is hard to evaluate considering lack of prospective or even retrospective study.
Prognostic Factor
The prognosis of CCS is uncertain. Some study showed that the median survival time of CCS patients was only 18 months. 29 One recent research showed two-year DFS and OS of the CCS patients were 49% and 60%, respectively. 11 In early-stage CCS patients, Farley et al also indicated that the 2 year survival rate was around 50%. 15 However, for advanced-stage CCS patients who account for 40-50% in all stages, survival rate cannot be estimated. 29 The prognostic factors of CCS are still indeterminate. There is evidence that the crucial factors revolved prognosis of CCS are the stage, presence of metastasis and extent of invasion. 34 The early tumor stage is an independently positive predictive factor. 11 There were some studies demonstrated homologous carcinosarcoma of the uterus was related to a longer survival compared with the heterologous carcinosarcoma.39,40 However, homologous and heterologous CCS has a comparable survival. 29 In addition, based on the presented report, neither epithelial nor mesenchymal components of the CCS has an exactly influence on DFS or OS. 11 Compared to cervical SCC and adenocarcinoma, primary CCS has the worst outcome. 3
Conclusion
CCS is an extremely rare and aggressive tumor commonly occurs in postmenopausal women. HPV infection in particular 16 type, pelvic radiotherapy and chemotherapy history are at high risk of developing CCS. According to the widely accepted “metaplastic theory,” CCS may stem from the carcinomatous elements and then differentiate into sarcoma components. The common manifestations such as vaginal bleeding is easy to be noticed, therefore CCS can be detected in the early stage. Pathologically, CCS is characterized as a biphasic admixture of intimately juxtaposed carcinomatous and sarcomatous components. Misdiagnosis of CCS sometimes happens in cervical samples due to the less identification of sarcomatous component. Thus, suspicion of CCS should be raised when sarcomatous component appears. Radical surgery and cytoreduction are primarily performed in patients with local CCS. Radiotherapy at the variable dose ranging from 40 Gy to 65.5 Gy as an adjuvant treatment option after surgery offers a better survival for early-stage CCS patients and platinum-based regimens are most commonly conducted in CCS patients in different stage. Patients can benefit from cryoablation followed by immunotherapy especially when patients with POLE mutation, but further evidence is required to confirm the effectiveness of this strategy. Early stage is the crucial factor to predict a positive survival. Further studies are needed to deeply explore the characteristics and pathogenesis of CCS, and to form a guideline of standard therapy in the future.
Supplemental Material
{kind=link}
Supplemental material, sj-jpg-1-onc-10.1177_11795549211056273 for Cervical Carcinosarcoma: Current Understanding on Pathogenesis, Diagnosis, Management and Future Perspectives by Xinyao Shu, Yuwen Zhou, Guixia Wei, Xiaorong Chen and Meng Qiu in Clinical Medicine Insights: Oncology
Footnotes
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions: XShu collected data, reviewed the literature and wrote the manuscript. YZhou collected data, wrote and revised the manuscript. GWei collected data and rechecked the manuscript. XChen assisted in drawing. MQiu design and revised the manuscript. All authors read and approved the final manuscript.
ORCID iD: Meng Qiu  https://orcid.org/0000-0003-3722-6938
https://orcid.org/0000-0003-3722-6938
Supplemental Material: Supplemental material for this article is available online.
References
- 1. Lin Y, Chen H, Ye Z, Ding L, Cao Q, Xue L. Synchronous carcinosarcoma of the uterine cervix with adenoid basal carcinoma and cervical intraepithelial neoplasia III: a case report and literature review. Pathol Res Pract. 2017;213:570-573. doi: 10.1016/j.prp.2017.02.006. [DOI] [PubMed] [Google Scholar]
- 2. Wright JD, Rosenblum K, Huettner PC, et al. Cervical sarcomas: an analysis of incidence and outcome. Gynecol Oncol. 2005;99:348-351. doi: 10.1016/j.ygyno.2005.06.021. [DOI] [PubMed] [Google Scholar]
- 3. Albert A, Lee A, Allbright R, Vijayakumar S. Primary sarcoma of the cervix: an analysis of patient and tumor characteristics, treatment patterns, and outcomes. J Gynecol Oncol. 2020;31:e25. doi: 10.3802/jgo.2020.31.e25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Sharma NK, Sorosky JI, Bender D, Fletcher MS, Sood AK. Malignant mixed Mullerian tumor (MMMT) of the cervix. Gynecol Oncol. 2005;97:442-445. doi: 10.1016/j.ygyno.2005.01.022. [DOI] [PubMed] [Google Scholar]
- 5. Semczuk A, Colas E, Walczyna B, et al. Coexistence of homologous-type cervical carcinosarcoma with endometrioid-type G1 endometrial cancer: a case report with an immunohistochemical study. Int J Clin Exp Pathol. 2014;7:7191-7195. eCollection 2014. [PMC free article] [PubMed] [Google Scholar]
- 6. Young N, Damien M, Schwartz PE, Carter D, Mittal KR. Carcinosarcoma of the uterine cervix initially interpreted as high grade sarcoma. Hum Pathol. 1988;19:605-608. doi: 10.1016/s0046-8177(88)80214-4. [DOI] [PubMed] [Google Scholar]
- 7. Bansal S, Lewin SN, Burke WM, et al. Sarcoma of the cervix: natural history and outcomes. Gynecol Oncol. 2010;118:134-138. doi: 10.1016/j.ygyno.2010.04.021. [DOI] [PubMed] [Google Scholar]
- 8. Barker HE, Scott CL. Genomics of gynaecological carcinosarcomas and future treatment options. Semin Cancer Biol. 2020;61:110-120. doi: 10.1016/j.semcancer.2019.10.006. [DOI] [PubMed] [Google Scholar]
- 9. Ribeiro-Silva A, Novello-Vilar A, Cunha-Mercante AM, De Angelo Andrade LA. Malignant mixed mullerian tumor of the uterine cervix with neuroendocrine differentiation. Int J Gynecol Cancer. 2002;12:223-227. doi: 10.1046/j.1525-1438.2002.01100.x. [DOI] [PubMed] [Google Scholar]
- 10. Grayson W, Taylor LF, Cooper K. Carcinosarcoma of the uterine cervix: a report of eight cases with immunohistochemical analysis and evaluation of human papillomavirus status. Am J Surg Pathol. 2001;25:338-347. doi: 10.1097/00000478-200103000-00008. [DOI] [PubMed] [Google Scholar]
- 11. Kimyon Comert G, Turkmen O, Karalok A, Basaran D, Bulbul D, Turan T. Therapy modalities, prognostic factors, and outcome of the primary cervical carcinosarcoma: meta-analysis of extremely rare tumor of cervix. Int J Gynecol Cancer. 2017;27:1957-1969. doi: 10.1097/igc.0000000000001086. [DOI] [PubMed] [Google Scholar]
- 12. Abell MR, Ramirez JA. Sarcomas and carcinosarcomas of the uterine cervix. Cancer. 1973;31:1176-1192. [DOI] [PubMed] [Google Scholar]
- 13. Bashour BN, Mancer K, Rance CP. Malignant mixed mullerian tumor of the cervix following cyclophosphamide therapy for nephrotic syndrome. J Pediatr. 1973;82:292-293. doi: 10.1016/s0022-3476(73)80173-8. [DOI] [PubMed] [Google Scholar]
- 14. Luo Y, Yao Q, Ren C, Ding X, Hu A, Liu C. HPV infection status in cervical metaplastic carcinomas. J Clin Pathol. 2015;68:170-172. doi: 10.1136/jclinpath-2014-202667. [DOI] [PubMed] [Google Scholar]
- 15. Farley JH, Taylor RR. Cervical carcinosarcoma occurring after subtotal hysterectomy, a case report. Gynecol Oncol. 1997;67:322-324. doi: 10.1006/gyno.1997.4872. [DOI] [PubMed] [Google Scholar]
- 16. Krishnan E, Coleman RE. Malignant mixed mullerian tumours of gynaecological origin: chemosensitive but aggressive tumours. Clin Oncol (R Coll Radiol). 1998;10:246-249. [DOI] [PubMed] [Google Scholar]
- 17. Silverberg SG. Mixed müllerian tumors. Curr Top Pathol. 1992;85:35-56. [DOI] [PubMed] [Google Scholar]
- 18. Kounelis S, Jones MW, Papadaki H, Bakker A, Swalsky P, Finkelstein SD. Carcinosarcomas (malignant mixed mullerian tumors) of the female genital tract: comparative molecular analysis of epithelial and mesenchymal components. Hum Pathol. 1998;29:82-87. [DOI] [PubMed] [Google Scholar]
- 19. Masuda A, Takeda A, Fukami H, Yamada C, Matsuyama M. Characteristics of cell lines established from a mixed mesodermal tumor of the human ovary. Carcinomatous cells are changeable to sarcomatous cells. Cancer. 1987;60:2696-2703. [DOI] [PubMed] [Google Scholar]
- 20. Kernochan LE, Garcia RL. Carcinosarcomas (malignant mixed Müllerian tumor) of the uterus: advances in elucidation of biologic and clinical characteristics. J Natl Compr Canc Netw. 2009;7:550-556; quiz 557. [DOI] [PubMed] [Google Scholar]
- 21. George E, Manivel JC, Dehner LP, Wick MR. Malignant mixed müllerian tumors: an immunohistochemical study of 47 cases, with histogenetic considerations and clinical correlation. Hum Pathol. 1991;22:215-223. [DOI] [PubMed] [Google Scholar]
- 22. Gourley C, Al-Nafussi A, Abdulkader M, Smyth JF, Gabra H. Malignant mixed mesodermal tumours: biology and clinical aspects. Eur J Cancer. 2002;38:1437-1446. [DOI] [PubMed] [Google Scholar]
- 23. McCluggage WG. Malignant biphasic uterine tumours: carcinosarcomas or metaplastic carcinomas? J Clin Pathol. 2002;55:321-325. doi: 10.1136/jcp.55.5.321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. D’Angelo E, Prat J. Pathology of mixed Müllerian tumours. Best Pract Res Clin Obstet Gynaecol. 2011;25:705-718. doi: 10.1016/j.bpobgyn.2011.05.010. [DOI] [PubMed] [Google Scholar]
- 25. Laterza R, Seveso A, Zefiro F, et al. Carcinosarcoma of the uterine cervix: case report and discussion. Gynecol Oncol. 2007;107:S98-S100. doi: 10.1016/j.ygyno.2007.07.038. [DOI] [PubMed] [Google Scholar]
- 26. Gastrell FH, Brasch HD, Johnson CA, Bethwaite PB, McConnell DT. Malignant mixed Müllerian tumour of the cervix treated with concurrent chemoradiation. Aust N Z J Obstet Gynaecol. 2001;41:352-354. [DOI] [PubMed] [Google Scholar]
- 27. Bagué S, Rodríguez IM, Prat J. Malignant mesonephric tumors of the female genital tract: a clinicopathologic study of 9 cases. Am J Surg Pathol. 2004;28:601-607. [DOI] [PubMed] [Google Scholar]
- 28. Meguro S, Yasuda M, Shimizu M, Kurosaki A, Fujiwara K. Mesonephric adenocarcinoma with a sarcomatous component, a notable subtype of cervical carcinosarcoma: a case report and review of the literature. Diagn Pathol. 2013;8:74. doi: 10.1186/1746-1596-8-74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Iida T, Yasuda M, Kajiwara H, et al. Case of uterine cervical carcinosarcoma. J Obstet Gynaecol Res. 2005;31:404-408. doi: 10.1111/j.1447-0756.2005.00310.x. [DOI] [PubMed] [Google Scholar]
- 30. Tseng CE, Chen CH, Chen SJ, Chi CL. Tumor rupture as an initial manifestation of malignant mesonephric mixed tumor: a case report and review of the literature. Int J Clin Exp Pathol. 2014;7:1212-1217. [PMC free article] [PubMed] [Google Scholar]
- 31. Maheshwari A, Gupta S, Shet T, Wuntkal R, Tongaonkar HB. Diagnostic dilemma in a case of malignant mixed mullerian tumor of the cervix. World J Surg Oncol. 2006;4:36. doi: 10.1186/1477-7819-4-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Wu YC, Yang CF, Hsu CN, Hsieh TC. Intramural metastases of rectum from carcinosarcoma (malignant müllerian mixed tumor) of uterine cervix. Clin Nucl Med. 2013;38:137-139. doi: 10.1097/RLU.0b013e318266d4bd. [DOI] [PubMed] [Google Scholar]
- 33. Ribeiro B, Silva R, Dias R, Patrício V. Carcinosarcoma of the uterine cervix: a rare pathological finding originating from mesonephric remnants. BMJ Case Rep. 2019;12:e227050. doi: 10.1136/bcr-2018-227050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Clement PB, Zubovits JT, Young RH, Scully RE. Malignant mullerian mixed tumors of the uterine cervix: a report of nine cases of a neoplasm with morphology often different from its counterpart in the corpus. Int J Gynecol Pathol. 1998;17:211-222. [PubMed] [Google Scholar]
- 35. Schipf A, Mayr D, Kirchner T, Diebold J. Molecular genetic aberrations of ovarian and uterine carcinosarcomas—a CGH and FISH study. Virchows Arch. 2008;452:259-268. doi: 10.1007/s00428-007-0557-6. [DOI] [PubMed] [Google Scholar]
- 36. Gotoh O, Sugiyama Y, Takazawa Y, et al. Clinically relevant molecular subtypes and genomic alteration-independent differentiation in gynecologic carcinosarcoma. Nat Commun. 2019;10:4965. doi: 10.1038/s41467-019-12985-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Kim M, Lee C, Choi H, Ko JK, Kang G, Chun KC. Carcinosarcoma of the uterine cervix arising from Müllerian ducts. Obstet Gynecol Sci. 2015;58:251-255. doi: 10.5468/ogs.2015.58.3.251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Zhu B, Liu Y, Li J, et al. Exceptional response of cryoablation followed by pembrolizumab in a patient with metastatic cervical carcinosarcoma with high tumor mutational burden: a case report. Oncologist. 2020;25:15-18. doi: 10.1634/theoncologist.2019-0739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Norris HJ, Taylor HB. Mesenchymal tumors of the uterus. 3. A clinical and pathologic study of 31 carcinosarcomas. Cancer. 1966;19:1459-1465. [DOI] [PubMed] [Google Scholar]
- 40. Barwick KW, LiVolsi VA. Malignant mixed müllerian tumors of the uterus. A clinicopathologic assessment of 34 cases. Am J Surg Pathol. 1979;3:125-135. [DOI] [PubMed] [Google Scholar]
- 41. Rodriguez-Escudero FJ, Martin Mateos M, Burgos J, Rementeria A, Lujan S. Malignant mixed müllerian tumor of the cervix in a 12-year-old girl. Eur J Gynaecol Oncol. 1988;9:365-369. [PubMed] [Google Scholar]
- 42. Abidi A, Menn K, Sherman A, Konia T, Azodi M. Cervical carcinosarcoma: a case report. J Reprod Med. 2008;53:138-140. [PubMed] [Google Scholar]
- 43. Wang L-H, Xiong Y, Li Y-F, et al. [Clinical analysis of 12 cases of uterine carcinosarcoma]. Ai Zheng. 2008;27:516-519. [PubMed] [Google Scholar]
- 44. Gan X-L, Li J-K, Yu T-H, Zhang Y, Hu LN. High expressions of bcl-2 and survivin, and decreased apoptosis in uterine cervical carcinosarcoma compared to cervical squamous cell carcinoma. Arch Gynecol Obstet. 2011;284:175-181. doi: 10.1007/s00404-010-1610-2. [DOI] [PubMed] [Google Scholar]
- 45. Miyazawa K, Hernandez E. Cervical carcinosarcoma: a case report. Gynecol Oncol. 1986;23:376-380. doi: 10.1016/0090-8258(86)90141-1. [DOI] [PubMed] [Google Scholar]
- 46. Kadota K, Haba R, Ishikawa M, et al. Uterine cervical carcinosarcoma with heterologous mesenchymal component: a case report and review of the literature. Arch Gynecol Obstet. 2009;280:839-843. doi: 10.1007/s00404-009-1017-0. [DOI] [PubMed] [Google Scholar]
- 47. Lopez-Chardi L, González-Bosquet E, Rovira Zurriaga C, Laïlla Vicens JM. Mesonephric carcinosarcoma of the uterine cervix: a case report. Eur J Gynaecol Oncol. 2013;34:336-338. [PubMed] [Google Scholar]
- 48. Lee SH, Kim J, Kim JH, Lee KH, Park JS, Hur SY. Malignant mixed mullerian tumor of the cervix including components of a rhabdomyosarcoma: case report and literature review. Eur J Gynaecol Oncol. 2010;31:462-466. [PubMed] [Google Scholar]
- 49. Takeshima Y, Amatya VJ, Nakayori F, et al. Co-existent carcinosarcoma and adenoid basal carcinoma of the uterine cervix and correlation with human papillomavirus infection. Int J Gynecol Pathol. 2002;21:186-190. [DOI] [PubMed] [Google Scholar]
- 50. Roma AA. Mesonephric carcinosarcoma involving uterine cervix and vagina: report of 2 cases with immunohistochemical positivity For PAX2, PAX8, and GATA-3. Int J Gynecol Pathol. 2014;33:624-629. doi: 10.1097/pgp.0000000000000088. [DOI] [PubMed] [Google Scholar]
- 51. Waxman M, Waxman JS, Alinovi V. Heterologous malignant mixed Müllerian tumor of the cervical stump. Gynecol Oncol. 1983;16:422-428. doi: 10.1016/0090-8258(83)90171-3. [DOI] [PubMed] [Google Scholar]
- 52. Piura B, Meirovitz M, Shaco-Levy R. Carcinosarcoma of the uterine cervix initially interpreted as myoma nascens. J Obstet Gynaecol. 2007;27:539-540 [DOI] [PubMed] [Google Scholar]
- 53. Munakata S, Iwai E, Tanaka T, Nakamura M, Kanda T. Malignant müllerian mixed tumor of the uterine cervix with a small cell neuroendocrine carcinoma component. Case Rep Pathol. 2013;2013:630859. doi: 10.1155/2013/630859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Connor JP. Aggressive carcinosarcoma of the uterine cervix associated with high levels of granulocyte colony stimulating factor: case report and laboratory correlates. Gynecol Oncol. 2006;103:349-353. doi: 10.1016/j.ygyno.2006.04.021. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, sj-jpg-1-onc-10.1177_11795549211056273 for Cervical Carcinosarcoma: Current Understanding on Pathogenesis, Diagnosis, Management and Future Perspectives by Xinyao Shu, Yuwen Zhou, Guixia Wei, Xiaorong Chen and Meng Qiu in Clinical Medicine Insights: Oncology