

Abstract
Purpose:
The purpose of this study was to determine the influence of outdoor activity on myopia progression.
Methods:
It was a hospital-based longitudinal prospective observational study. Children between 7 and 14 years of age with a myopia of − 0.5 D or worse were included. Myopia progression was evaluated by cycloplegic refraction, every 6 months for 18 months. Parents were asked to record the daily outdoor activity of the child in hours per day at school and at home during weekdays and at weekends separately, based on which the daily outdoor activity score was calculated. The independent variables measured included age and gender of the participant, degree of myopia, and the daily outdoor activity score. Progression of myopia was defined as an increase in the spherical equivalent (SE) over 18 months. The magnitude of the association was determined by two mixed-effects models.
Results:
A total of 495 participants (250 males and 245 females) completed three visits during the study period. On taking age groups and paired observations as a random effect and adding SE at the last visit as the random slope in Model 1, each unit increase in outdoor activity had a negative effect on change in SE of − 0.01 (−0.02 to 0.00; P = 0.045). The same inverse relationship between outdoor activity and absolute SE as − 0.06 (−0.07 to − 0.03; P < 0.001) is estimated in Model 2.
Conclusion:
The study demonstrates a statistically significant inverse relationship between outdoor activity and myopia.
Keywords: Myopia, outdoor activity, progression, risk factors
Myopia is one of the most common refractive errors, characterized by an increase in the axial length of the eyeball relative to the refractive power of the eye. There has been an increase in the prevalence of childhood myopia over the past few decades, and it has emerged as a significant public health problem across the globe.[1,2,3] Children from many ethnicities – such as the East Asians – have shown a prevalence of childhood myopia nearing or even crossing 50% of the total population.[3] It is estimated that half of the world’s population will become myopic by 2050.[4] An association between high myopia and vision-threatening ocular complications, such as cataract, glaucoma, retinal detachment, macular degeneration, and choroidal neovascularization, is well established.[5]
Despite evidence of the increasing prevalence of childhood myopia and the attendant increased risk of ocular complications with its progression, understanding of the factors associated with its onset and progression remain limited.
Although genetic factors play a significant role in the development of myopia,[6] the rapid increase in the incidence and prevalence of myopia in school-going children has prompted research into the role of some epigenetic factors specifically associated with the lifestyle that may have an impact on myopia progression.[7,8]
There seems to be a complex interaction between environmental factors such as near work, outdoor activity, and myopia progression. Some studies have suggested an association between near work and myopia[9,10] even after adjustment for parental history of myopia,[11] whereas some others have found no significant association between them.[12,13,14] Similarly, some studies have found that an increase in the amount of outdoor activity is associated with a reduction in the risk of occurrence and progression of myopia in children,[13,15] whereas others have found no association between time spent in outdoor activity and myopia.[16,17] Therefore, it seems that there might be intermediary factors such as the age of the participants in causal pathways that may influence the cause-to-effect relationship to be ambidirectional.
Although there has been a reportedly steep increase in the reported number of myopia cases over the past decade in schoolchildren in India,[18,19] there seems to be a paucity of longitudinal or follow-up studies that may ascertain the effect more deterministically. Thus, we planned a study to determine the influence of outdoor activities on myopia progression trajectories by following the participants longitudinally and using a mixed-effects model thereby accounting for data noises created by age and baseline spherical equivalent (SE).
Methods
This study was designed as a hospital-based longitudinal prospective observational study. Data were collected from June 2018 to March 2020 at a tertiary-care hospital. The study followed the tenets of the Declaration of Helsinki for biomedical research and was approved by the Institutional Human Ethics Committee (Letter of Permission No. IHEC-LOP/2018/IM0198, granted in May 2018).
A patient information sheet explaining the aims and objectives of the study and details of the ocular examination that would be carried out was given to the parents or guardians of all participants. The sheets were in both Hindi and English. Written informed consent was obtained from the parents or guardians, and verbal consent from each child was obtained before enrolling them in the study and also before each examination.
Children aged between 7 and 14 years who presented to the outpatient department with decreased vision and children with myopia were invited to participate in the study. Those children whose parents or guardians gave consent for including their wards in the study were included. Children were excluded if they had refractive errors other than myopia. Children having any other anterior or posterior segment ocular disorders, strabismus, glaucoma, and so on were also excluded. Other exclusion criteria included children with a family history of myopia and whose parents or guardians did not give consent to participate in the study.
A total of 580 children were enrolled over a period of 4 months. A detailed history was taken, including a history of presenting illness and any family history of myopia. History of spectacle use was also recorded. Visual acuity testing was done with Snellen chart at a distance of 6 m. A comprehensive ophthalmological examination was also done. All children with vision <6/9 underwent cycloplegic refraction. Cyclopentolate 1% eye drop was instilled every 10 minutes twice in both the eyes. After 45 minutes, if pupillary light reaction was present, then a third drop was instilled. Cycloplegia was considered complete if pupillary dilatation was ≥6 mm and there was no pupillary reaction to light. Retinoscopy was done with a streak retinoscope. Subjective acceptance was done on follow-up after a week. The refractive error was recorded, and spectacles were prescribed based on subjective acceptance. The SE for both eyes was calculated and recorded. The analysis was performed using data for the right eye only in all the participants.
Myopia was defined as an SE of − 0.5 D or worse, measured by cycloplegic refraction. SE was calculated as the sum of spherical power plus half of the cylindrical power.
Parents were asked to record the daily outdoor activity of the child in hours per day at school and at home during weekdays and at weekends separately on a calendar. The parents were asked to bring the calendar for follow-up visits every 6 months to show the total outdoor activity performed by the child every day.
Outdoor activity was defined as the time spent in outdoor activities in the daylight such as playing on the ground during a break period in the school, playing outdoor sports, riding a bicycle, swimming, running, playing in the park, and so on.
The average outdoor activity hours per day was calculated using the following formula: [20]

The outdoor activity score was obtained by calculating the mean number of hours spent on the total outdoor activity per day at every follow-up visit.
The independent variables measured included age and gender of the participant, degree of myopia on the basis of SE at every visit, and the outdoor activity score. All children were followed up at every 6 months for 18 months. At each visit, measurement of visual acuity using Snellen chart, comprehensive ocular examination, cycloplegic refraction, and period of outdoor activity (hour per day) was recorded. Progression of myopia was defined as an increase in the SE of the child over a period of 18 months.
Data analysis
Data thus collected were checked for the missing values, outliers, and redundancies. The mean ± SD was calculated for each age group as a descriptive summary measure for all four visits. The trends in SE and activity longitudinally from Visit 1 to Visit 4 (across the age groups) were visualized with the spaghetti diagrams, which showed the line of central tendency with dispersion as a shadowed area.
In the next step, the point estimate and 95% confidence interval (CI) for repeated measure correlation were calculated with the aid of rmcorr package in R software, which is available in the public domain. This correlation considers the interrelatedness among observations after accounting for interindividual variability through analysis of covariance (ANCOVA). Thus, the correlation graph created by this method offers the best linear fit for each participant using parallel regression lines (identical slope) but with varying intercepts. The computed paired r coefficient represented a common intraindividual association between refraction and outdoor activity score. Hence, this method gave an advantage over other correlational methods because it omitted the possibility of spurious association that could arise due to assigning nonindependent values as independent identical distribution.
After assessing the directional relationship, the magnitude of the association was determined
by two mixed-effects models that estimated the effect of per unit outdoor activity (here taken as an hour spent outdoor) to change in SE in subsequent visits after adjusting for baseline activity and age category. Subsequently, two mixed-effects models were built.
Box 1.
| Model 1: Difference in SE~activity + (1| age category) + (1| participant ID) |
| Model 2: SE~activity + (1|age category) + (SE during last visit|participant ID) |
The first model looks for the difference in the SE in subsequent visit (d SE) as the dependent variable, and the second model looks for absolute SE in the current visit in reference to the last visit (SE last as random slope) as the dependent variable. Both models address the variability created by paired observation (participant ID) and age (age category) by placing them as a random slope. Effect sizes were labeled following Cohen’s (1988) recommendations.
Results
A total of 495 participants (250 males and 245 females) completed three visits during the study period. Table 1 shows the descriptive profile of participants along with SE and outdoor activity score (in hours) distributed among the age group (determined during first visit) of participants.
Table 1.
Demographic profiles of participants and relevant attributes (spherical equivalent and outdoor activity) across the four visits
| Variable | <9 years (n=124)a | 9-11 years (n=96)a | 11-13 years (n=178)a | >13 years (n=97)a | P b |
|---|---|---|---|---|---|
| Gender | 0.2 | ||||
| Female | 64 (26%) | 49 (20%) | 93 (38%) | 39 (16%) | |
| Male | 60 (24%) | 47 (19%) | 85 (34%) | 58 (23%) | |
| Visit 1 | |||||
| Spherical equivalent | 2.09 (1.07) | 2.24 (1.10) | 2.24 (0.95) | 2.34 (1.26) | 0.5 |
| Outdoor activity | 2.40 (1.06) | 1.98 (0.91) | 2.05 (0.93) | 2.15 (0.96) | 0.002* |
| Visit 2 | |||||
| Spherical equivalent | 2.31 (1.11) | 2.44 (1.14) | 2.45 (0.99) | 2.54 (1.29) | 0.5 |
| Outdoor activity | 2.50 (1.21) | 1.91 (1.02) | 2.27 (1.40) | 2.04 (1.15) | 0.018* |
| Visit 3 | |||||
| Spherical equivalent | 2.51 (1.06) | 2.61 (1.12) | 2.61 (0.94) | 2.70 (1.25) | 0.7 |
| Outdoor activity | 2.15 (1.07) | 1.79 (1.13) | 2.13 (1.49) | 2.04 (1.28) | 0.13 |
| Visit 4 | |||||
| Spherical equivalent | 2.63 (1.08) | 2.74 (1.15) | 2.71 (0.96) | 2.78 (1.25) | 0.8 |
| Outdoor activity | 2.12 (1.05) | 1.76 (1.04) | 1.92 (0.97) | 1.80 (1.12) | 0.11 |
*Significant at 95%C; aStatistics presented: n (%); mean (SD). bStatistical tests performed: Chi-square test of independence; Kruskal-Wallis test
We also constructed a composite spaghetti diagram to explore the longitudinal trends in SE and the corresponding outdoor activity (in hours) [Fig. 1]. This figure assigns a visual gradient of simultaneous change in both variables with reference to time and age category.
Figure 1.
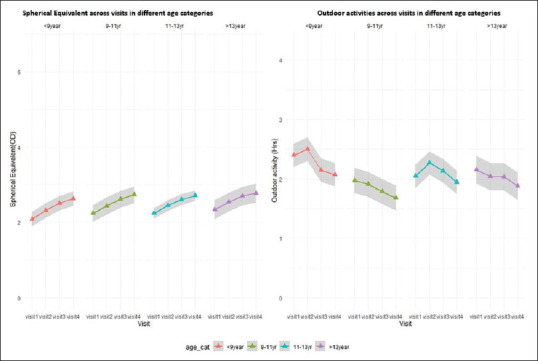
Spaghetti plot representing the progression of myopia and the number of hours spent in outdoor activity across four visits categorized according to age groups
In the next step, intraindividual assocation between SE and activity scores (in hours) for three subsequent visits was determined by repeated measures correlation. This was calculated as − 0.26 (−0.21 to − 0.30; P = 0.001), which showed a statistically significant negative directional relationship [Fig. 2]. In Fig. 2, the best linear fit for each participant is shown using parallel regression lines (to account for interindividual variability) but with varying intercepts representing the intraindividual association between activity and refraction across the three visits. The dashed line represents the overall negative correlational trend.
Figure 2.
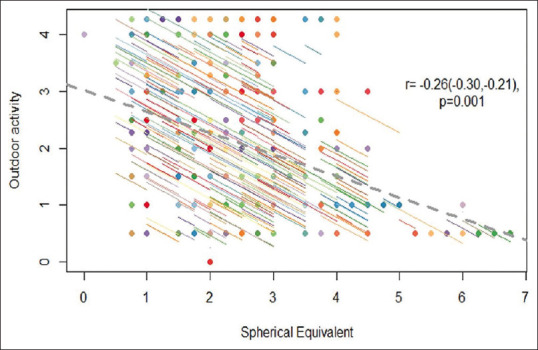
Repeat measures correlation showing statistically significant inverse relationship between outdoor activity and spherical equivalent
After determining the directional relationship, the magnitude of the relationship was established by two mixed-effects models as mentioned in Bo × 1.
The model’s total explanatory power is substantial (conditional R2 = 1.00) and the part related to the fixed effects alone (marginal R2) is 6.42e − 06. The model’s intercept is 3.47 (SE = 0.02, 95% CI [3.44, 3.51]; P < 0.001). Within this model, the effect of outdoor activity was detected as negative and found to be significant (b = −6.64e − 03, SE = 2.59e − 03, 95% CI [−0.01, −1.56e − 03]; P < 0.05). As seen in Table 2, on taking age groups and paired observations as random effect and adding SE at last visit as random slope in Model 1, each unit increase in outdoor activity (i.e. every extra hour spent outdoors) has a negative effect on change in SE of − 0.01 (−0.02 to 0.00; P = 0.045). The same inverse relationship between activity and absolute SE as − 0.06 (−0.07 to − 0.03; P < 0.001) is estimated in Model 2.
Table 2.
Model 1 and Model 2 as linear mixed-effects models showing fixed-effect coefficients, random-effect coefficients, and model summary
| Predictors | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| Estimates | CI | P | Estimates | CI | P | |
| (Intercept) | 0.18 | 0.16-0.21 | <0.001 | 3.08 | 3.02-3.14 | <0.001 |
| Outdoor activity | −0.01 | −0.02 to 0.00 | 0.045 | −0.06 | −0.07 to−0.03 | <0.001 |
| Random Effects | ||||||
| σ2 | 0.04 | 0.02 | ||||
| τ00 | 0.01id | 5.00id | ||||
| 0.00age_cat | 0.00age_cat | |||||
| τ11 | 0.63id.r.last# | |||||
| ρ01 | −0.99id | |||||
| ICC | 0.15 | 1.00 | ||||
| Marginal R2/Conditional R2 | 0.003/0.157 | 0.001/0.996 | ||||
CI=confidence interval, ICC=intraclass correlation. t2 or Tau2 / s2= symbols showing between-model variance in a random-effects model at null intercept and at an alternate model
Discussion
The present study was undertaken to evaluate the influence of outdoor activity on the progression of myopia. To our knowledge, this is the first hospital-based prospective longitudinal study done on a cohort of children presenting to a tertiary-care center in India. The study demonstrates a statistically significant inverse relationship between outdoor activity and myopia.
The rapid increase in the prevalence of myopia in recent decades suggests that besides genetic factors there are environmental factors – termed “myopigenic” – that strongly contribute to the development and the progression of myopia.[21]
A number of epidemiological studies from different geographical locations have shown that a lack of outdoor activity in childhood is an important environmental risk factor associated with myopia,[15,22,23] although the evidence regarding the effect of outdoor activity on the progression of myopia is still conflicted.
In a randomized clinical trial done among 6-year-old children in China, the addition of 40 minutes class of outdoor activity at school resulted in a statistically significant lower incidence of myopia in the intervention group compared with the control group.[24] Similarly, an Indian study found that the progression of myopia in children was significantly associated with hours of reading or writing per week, use of computers or video games, and watching television. At the same time, outdoor activity for more than 2 hours per day was found to be significantly associated with a protective effect against the progression of myopia.[19] Similar findings were also seen in a study conducted in rural Northeast China.[25] These findings are also reflected in our study, where a statistically significant negative relationship was found between outdoor activity and progression of myopia. On the other hand, other studies from China and the United States have found no association between hours spent in outdoor activity and the progression of myopia.[16,17]
The results of our study showed that the total time spent in outdoor activities per day at school and at home was protective, as a significant inverse relationship between outdoor activity and myopia was found with time spent in outdoor activity, with a protective effect of each extra hour spent outdoors on the difference in myopia in progressive visits. Each hour increase in outdoor activity per day had a negative effect on the change of SE by 0.06 D on a subsequent visit, as compared with the previous visit. Thus, the purpose of the mixed-effects model is to translate the biological effect (of absolute change in SE values to change in outdoor activity) to the language of mathematics and to assign quantitative terms to this change. This small change in SE may not be perceived as significant from the clinical perspective at first glance as one might overlook the “direction” of change. Looking at the phenomenon from vectorized perspective, it does indicate that one may expect to see a lesser gradient of myopia progression in a child having more physical activity compared with a less physically active child, and this effect seems to be there after adjusting with age and baseline category of activity.
The exact mechanism by which outdoor activity decreases the progression of myopia is not known. Outdoor activity or playing outdoors is usually associated with exposure to bright sunlight. It has been suggested that there is a release of dopamine from the retina in response to bright light, and increased dopamine release inhibits axial elongation of the eyeball.[26,27] This hypothesis was supported by an investigation in chickens in which it was found that D2-dopamine antagonist partially reduced the protective effect of bright sunlight.[28]
Our study has multiple strengths. In addition to it being an institution-based study with a high follow-up rate, we ensured minimal recall bias by asking the parents to record the daily outdoor activity of the child at school and at home, as the number of hours per day by writing on a calendar provided to them. They were requested to bring the calendar at each follow-up visit, and we calculated the total outdoor activity per week from it. This helped us maintain observational rigor as compared with the studies where outdoor activity was calculated based on retrospective questionnaires administered to parents. Also, because the current study is longitudinal, it helps us establish a causal association between hours spent in outdoor activities and the progression of myopia. The large sample size also adds credence to the findings of our study. The mixed-effects modeling used in this study and ANCOVA-based paired correlation duly check the effect modification. Our study is limited by its institutional nature, which does not allow us to extend the findings from this study onto the general population.
Conclusion
Myopia has become an important health issue in India with a progressive increase in the prevalence of myopia.[29] Changes in the lifestyle of children resulting in more time being spent indoors with a plethora of activities – entertaining, educational, and otherwise – at their disposal have rendered them more vulnerable to the progression of myopia. Our study found a statistically significant negative directional relationship between outdoor activity and myopia. Each hour increase in outdoor activity per day had a protective effect on the progression of myopia. Spending time in outdoor activities has multiple benefits other than just reducing the chances of progression of myopia – it is of benefit in a range of disorders from attention-deficit/hyperactivity disorder to asthma and life stress.[30,31,32,33] The protective effect of daylight outdoor activities suggests that a public health measure aimed at preventing the progression of myopia could be based on increasing hours of outdoor activity for children, targeting not only the parents but also the schools to bring about changes in the school curriculum to increase the outdoor activity. This may prove to be a simple strategy to reduce the progression of myopia and may also help in the general health of the children.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1. Rudnicka AR, Kapetanakis VV, Wathern AK, Logan NS, Gilmartin B, Whincup PH, et al. Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis:Implications for aetiology and early prevention. Br J Ophthalmol. 2016;100:882–90. doi: 10.1136/bjophthalmol-2015-307724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Hsiao M, Malhotra A, Thakur JS, Sheth JK, Nathens AB, Dhingra N, et al. Road traffic injury mortality and its mechanisms in India:Nationally representative mortality survey of 1.1 million homes. BMJ Open. 2013;3 doi: 10.1136/bmjopen-2013-002621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Williams KM, Bertelsen G, Cumberland P, Wolfram C, Verhoeven VJ, Anastasopoulos E, et al. Increasing prevalence of myopia in europe and the impact of education. Ophthalmology. 2015;122:1489–97. doi: 10.1016/j.ophtha.2015.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Holden BA, Fricke TR, Wilson DA, Jong M, Naidoo KS, Sankaridurg P, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123:1036–42. doi: 10.1016/j.ophtha.2016.01.006. [DOI] [PubMed] [Google Scholar]
- 5. Foster PJ, Jiang Y. Epidemiology of myopia Eye. 2014. 28:202–8. doi: 10.1038/eye.2013.280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Goldschmidt E, Jacobsen N. Genetic and environmental effects on myopia development and progression. Eye. 2014;28:126–33. doi: 10.1038/eye.2013.254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Recko M, Stahl ED. Childhood myopia:Epidemiology, risk factors, and prevention. Mo Med. 2015;112:116–21. [PMC free article] [PubMed] [Google Scholar]
- 8. Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012;31:622–60. doi: 10.1016/j.preteyeres.2012.06.004. [DOI] [PubMed] [Google Scholar]
- 9. Hepsen IF, Evereklioglu C, Bayramlar H. The effect of reading and near-work on the development of myopia in emmetropic boys:A prospective, controlled, three-year follow-up study. Vision Res. 2001;41:2511–20. doi: 10.1016/s0042-6989(01)00135-3. [DOI] [PubMed] [Google Scholar]
- 10. Huang HM, Chang DST, Wu PC. The association between near work activities and myopia in children-A systematic review and meta-analysis. PLoS One. 2015;10:ne0140419. doi: 10.1371/journal.pone.0140419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Zadnik K, Satariano WA, Mutti DO, Sholtz RI, Adams AJ. The Effect of parental history of myopia on children's eye size. JAMA J Am Med Assoc. 1994;271:1323–7. [PubMed] [Google Scholar]
- 12. Lin Z, Gao TY, Vasudevan B, Ciuffreda KJ, Liang YB, Jhanji V, et al. Near work, outdoor activity, and myopia in children in rural China:The Handan offspring myopia study. BMC Ophthalmol. 2017;17:203. doi: 10.1186/s12886-017-0598-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Jones LA, Sinnott LT, Mutti DO, Mitchell GL, Moeschberger ML, Zadnik K. Parental history of myopia, sports and outdoor activities, and future myopia. Investig Ophthalmol Vis Sci. 2007;48:3524–32. doi: 10.1167/iovs.06-1118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Ip JM, Saw SM, Rose KA, Morgan IG, Kifley A, Wang JJ, et al. Role of near work in myopia:Findings in a sample of Australian school children. Investig Ophthalmol Vis Sci. 2008;49:2903–10. doi: 10.1167/iovs.07-0804. [DOI] [PubMed] [Google Scholar]
- 15. Rose KA, Morgan IG, Ip J, Kifley A, Huynh S, Smith W, et al. outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115:1279–85. doi: 10.1016/j.ophtha.2007.12.019. [DOI] [PubMed] [Google Scholar]
- 16. Lu B, Congdon N, Liu X, Choi K, Lam DS, Zhang M, et al. Associations between near work, outdoor activity, and myopia among adolescent students in rural China:The Xichang pediatric refractive error study report no. 2. Arch Ophthalmol. 2009;127:769–75. doi: 10.1001/archophthalmol.2009.105. [DOI] [PubMed] [Google Scholar]
- 17. Jones-Jordan LA, Sinnott LT, Cotter SA, Kleinstein RN, Manny RE, Mutti DO, et al. Time outdoors, visual activity, and myopia progression in juvenile-onset myopes. Investig Ophthalmol Vis Sci. 2012;53:7169–75. doi: 10.1167/iovs.11-8336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Saxena R, Vashist P, Menon V. Is myopia a public health problem in India? Indian J Community Med. 2013;38:83–5. doi: 10.4103/0970-0218.112436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Saxena R, Vashist P, Tandon R, Pandey RM, Bhardawaj A, Gupta V, et al. Incidence and progression of myopia and associated factors in urban school children in Delhi:The North India Myopia Study (NIM Study) PLoS One. 2017;12:e0189774. doi: 10.1371/journal.pone.0189774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Dirani M, Tong L, Gazzard G, Zhang X, Chia A, Young TL, et al. Outdoor activity and myopia in Singapore teenage children. Br J Ophthalmol. 2009;93:997–1000. doi: 10.1136/bjo.2008.150979. [DOI] [PubMed] [Google Scholar]
- 21. Morgan I, Rose K. How genetic is school myopia? Prog Retin Eye Res. 2005;24:1–38. doi: 10.1016/j.preteyeres.2004.06.004. [DOI] [PubMed] [Google Scholar]
- 22. Mutti DO, Mitchell GL, Moeschberger ML, Jones LA, Zadnik K. Parental myopia, near work, school achievement, and children's refractive error. Investig Opthalmology Vis Sci. 2002;43:3633–40. [PubMed] [Google Scholar]
- 23. Sherwin JC, Reacher MH, Keogh RH, Khawaja AP, MacKey DA, Foster PJ. The association between time spent outdoors and myopia in children and adolescents:A systematic review and meta-analysis. Ophthalmology. 2012;119:2141–51. doi: 10.1016/j.ophtha.2012.04.020. [DOI] [PubMed] [Google Scholar]
- 24. He M, Xiang F, Zeng Y, Mai J, Chen Q, Zhang J, et al. Effect of time spent outdoors at school on the development of myopia among children in China a randomized clinical trial. JAMA. 2015;314:1142–8. doi: 10.1001/jama.2015.10803. [DOI] [PubMed] [Google Scholar]
- 25. Jin JX, Hua WJ, Jiang X, Wu XY, Yang JW, Gao GP, et al. Effect of outdoor activity on myopia onset and progression in school-aged children in northeast china:The sujiatun eye care study. BMC Ophthalmol. 2015;15:73. doi: 10.1186/s12886-015-0052-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. French AN, Ashby RS, Morgan IG, Rose KA. Time outdoors and the prevention of myopia. Exp Eye Res. 2013;114:58–68. doi: 10.1016/j.exer.2013.04.018. [DOI] [PubMed] [Google Scholar]
- 27. McCarthy CS, Megaw P, Devadas M, Morgan IG. Dopaminergic agents affect the ability of brief periods of normal vision to prevent form-deprivation myopia. Exp Eye Res. 2007;84:100–7. doi: 10.1016/j.exer.2006.09.018. [DOI] [PubMed] [Google Scholar]
- 28. Nickla DL, Totonelly K. Dopamine antagonists and brief vision distinguish lens-induced- and form-deprivation-induced myopia. Exp Eye Res. 2011;93:782–5. doi: 10.1016/j.exer.2011.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Sheeladevi S, Seelam B, Nukella PB, Modi A, Ali R, Keay L. Prevalence of refractive errors in children in India:A systematic review. Clin Exp Optom. 2018;101:495–503. doi: 10.1111/cxo.12689. [DOI] [PubMed] [Google Scholar]
- 30. Taylor AF, Kuo FE, Sullivan WC. Coping with add:The surprising connection to green play settings. Environ Behav. 2001;33:54–77. [Google Scholar]
- 31. Kuo FE, Faber Taylor A. A potential natural treatment for attention-deficit/hyperactivity disorder:Evidence from a national study. Am J Public Health. 2004;94:1580–6. doi: 10.2105/ajph.94.9.1580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Lovasi GS, Quinn JW, Neckerman KM, Perzanowski MS, Rundle A. Children living in areas with more street trees have lower prevalence of asthma. J Epidemiol Community Health. 2008;62:647–9. doi: 10.1136/jech.2007.071894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Thompson Coon J, Boddy K, Stein K, Whear R, Barton J, Depledge MH. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors?A systematic review. Environ Sci Technol. 2011;45:1761–72. doi: 10.1021/es102947t. [DOI] [PubMed] [Google Scholar]