
FIGURE 2.
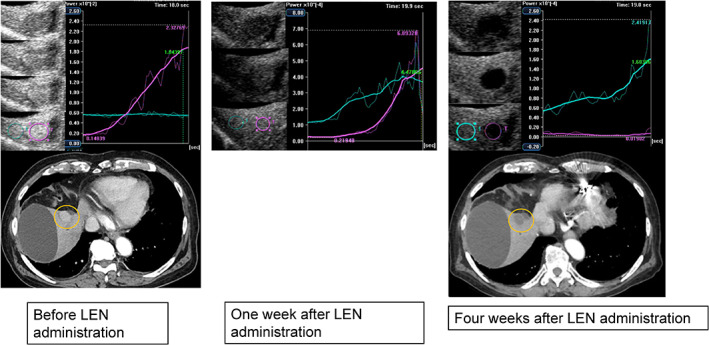
Clinical example of a good responder. An 87‐year‐old man with a history of hepatitis non‐B, non‐C virus cirrhosis underwent central hepatic bisection resection, and transcatheter arterial chemoembolization (TACE) for advanced hepatocellular carcinoma. Subsequently, he underwent radiofrequency ablation (RFA) under laparotomy for HCC recurrence. After RFA under laparotomy, the biliary cyst was complicated. HCC recurrence was observed in S5. TACE was difficult because of the presence of bile cysts. Radiation therapy was difficult near the intestine, and LEN administration (8 mg/day) was initiated. Gray‐scale ultrasonography showed a mosaic‐pattern tumor, of diameter 23 mm, in S5. This tumor was established as the target lesion. Images were taken with blood vessels and cysts near the tumor as landmarks. The left image was taken before LEN administration, the center was taken 1 week after LEN administration, and the right image was taken and TCA was performed 4 weeks after LEN administration. In each period, the CEUS, TCA, and CT were used for evaluation. TCA could measure the brightness of perflubutane. The brightness unit was automatically adjusted according to the numerical values of the HCC and background. Before administration, the peak intensity of the tumor was higher than that of the background liver. One week after LEN administration, the TCA results of the tumor and background liver were similar. Four weeks after LEN administration, it was reversed and the TCA result of the background liver was higher than that of the tumor. Four weeks after LEN treatment, a dynamic CT scan in the arterial phase showed a hypovascular lesion in S5, which was reduced. This therapeutic response was described as a partial response