
FIGURE 1.
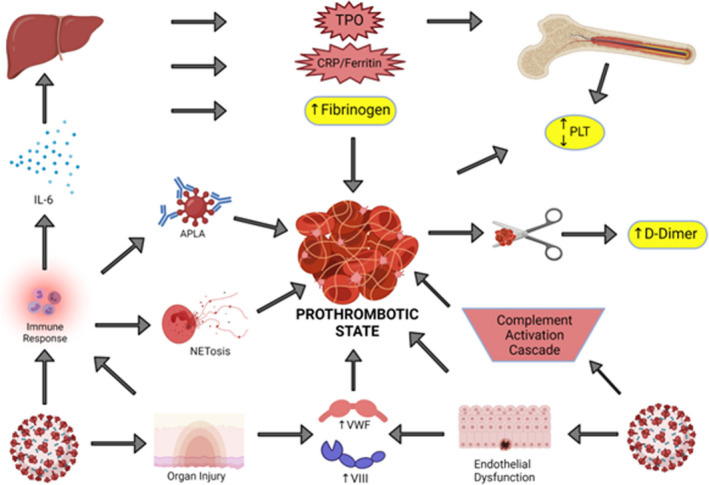
Prothrombotic state of COVID‐19 infection. The pathogenesis of the hypercoagulable state of COVID‐19 infection is depicted above. Bottom left: COVID‐19 infection can lead to a robust immune response with resultant secretion of cytokines (such as interleukin‐6 [IL‐6]), antiphospholipid antibodies (APLA), and neutrophil extracellular traps (NETosis). Bottom right: COVID‐19 infection also leads to complement activation in addition to endothelial dysfunction and organ injury which increases procoagulant molecules such as von Willebrand factor and factor VIII. Top left: Liver injury can occur due to endotheliopathy, which leads to an overall increase in inflammatory markers such as fibrinogen, CRP (C Reactive Protein) and thrombopoietin (TPO). Top right: Acute infection can have a variable effect on the platelet (PLT) count and the D‐dimer is elevated in the setting of fibrinolysis of micro‐ or macrovascular thrombosis