
Figure 5: PP2A inactivation predicts sensitivity and response to Gemcitabine treatment in a cohort of patients.
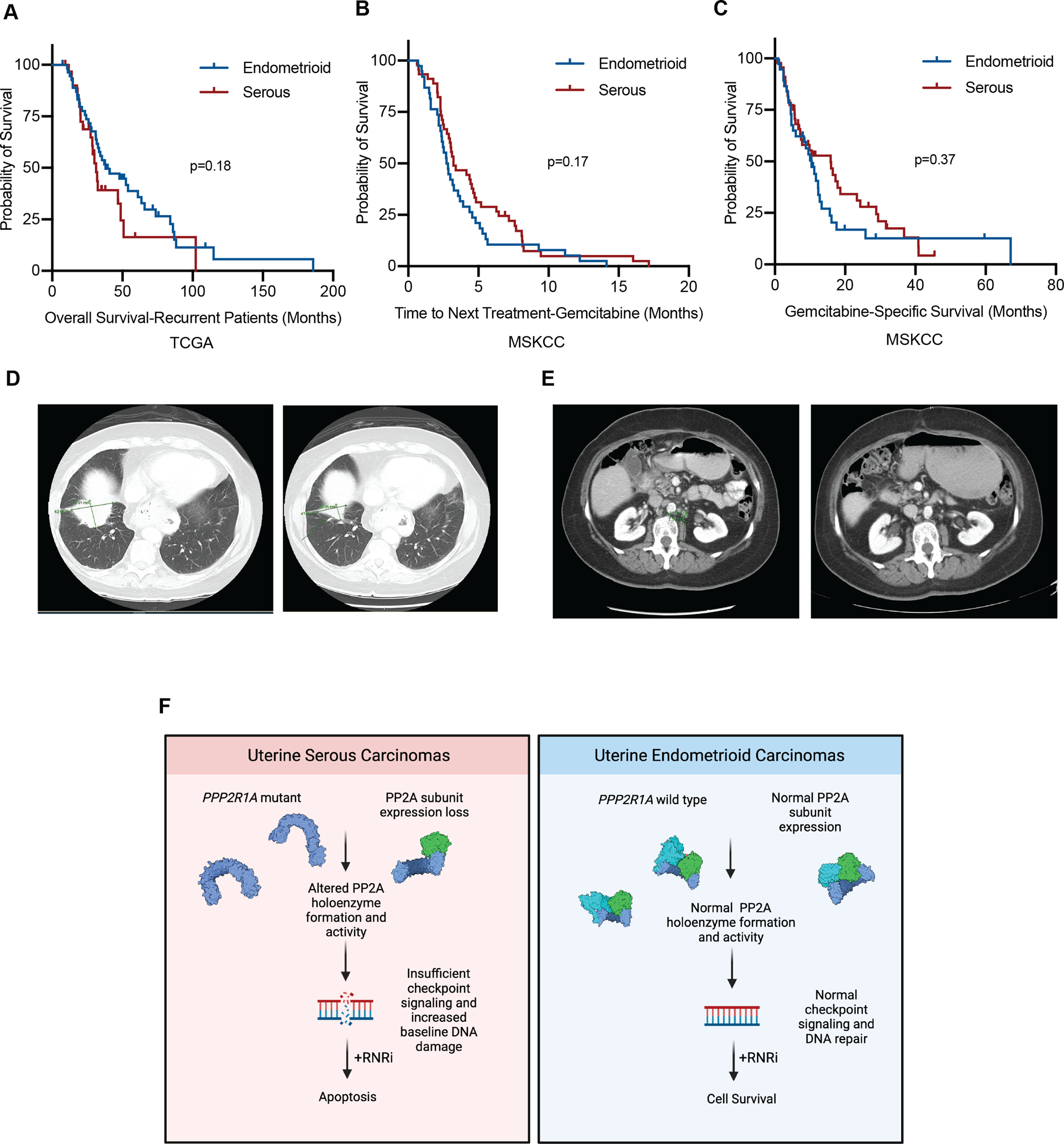
A-C, Kaplan-Meier estimates of survival as stratified by histology. Blue line represents endometrioid or mixed endometrioid (not serous) histology, red line represents serous or mixed serous histology. (A) Overall survival of patients with recurrent disease from the TCGA (B) Time to next treatment following initiation of gemcitabine. (C) Initiation of gemcitabine to date of death or last follow-up. D, CT images of the first patient before initiation of gemcitabine (left) and after (right). E, CT images of the second patient before the initiation of gemcitabine (left) and after (right). F, Schematic of the working model of the proposed studies. In USC (left) PP2A subunit expression is decreased, or PP2A Aα mutations are present, leading to a reduction in PP2A subunit expression. This in turn leads to altered PP2A activity, causing inefficient checkpoint signaling and increased DNA damage, leading to a synthetic lethal interaction with RNR inhibition. Conversely, in UEC PP2A Aα mutations and subunit expression loss are infrequent, allowing for normal checkpoint signaling and DNA damage repair. Under challenge with RNR inhibition, these cells are more capable of dealing with the DNA damage caused by these agents, and cells are more likely to survive. Created with BioRender.com.