
FIG 1.
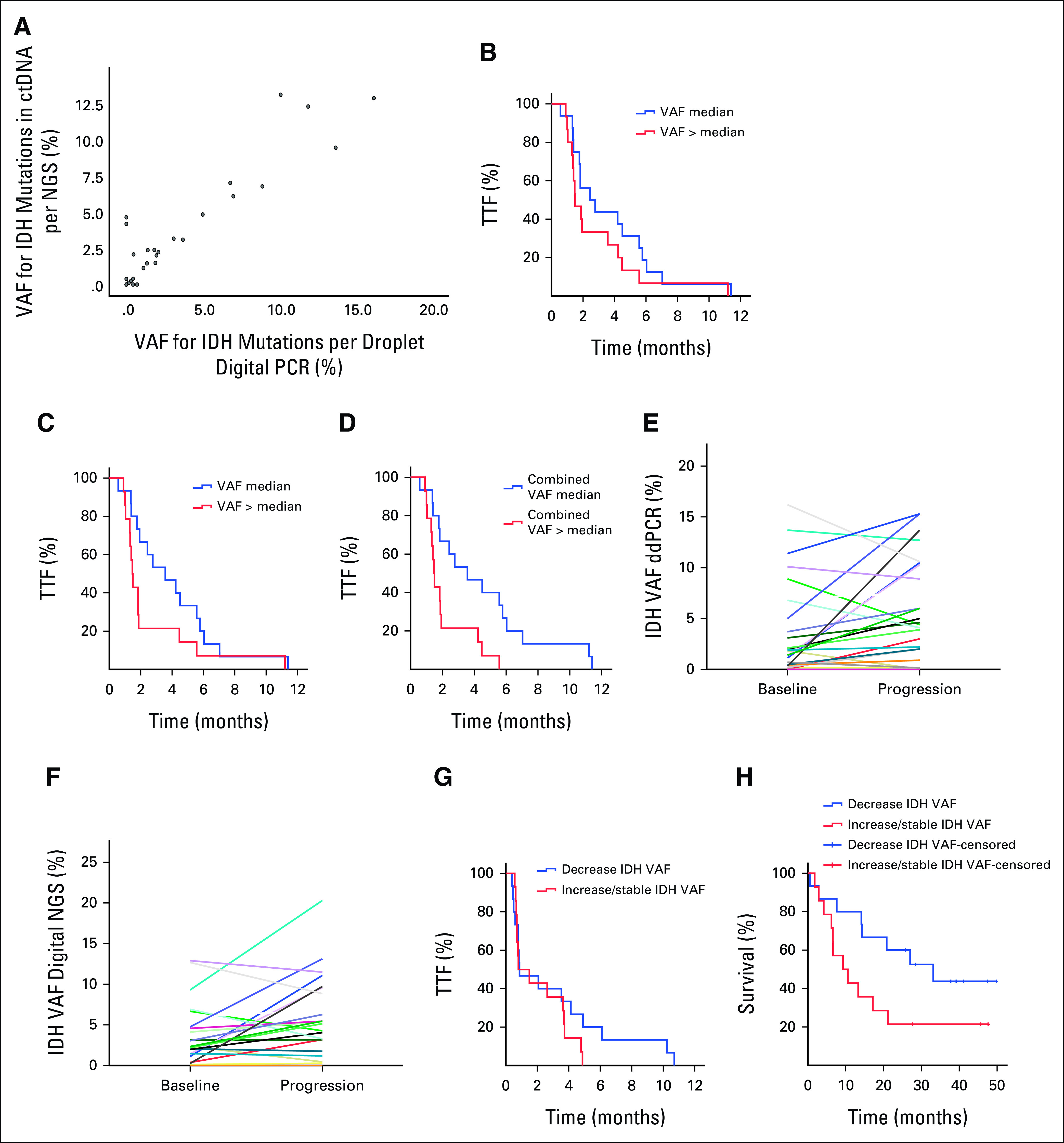
(A) There was a correlation (0.8, P < .001) between ddPCR and digital NGS for reported VAF in ctDNA. (B) Kaplan-Meier curves for TTF analyses per baseline quantity of ctDNA (≤ median v > median) in blood samples for IDH mutations detected by ddPCR (VAF ≤ 1.4% v VAF > 1.4 %; P = .21), (C) IDH mutations detected by digital NGS (VAF ≤ 2.2% v VAF > 2.2%; P = .09), (D) and the combined VAF for all alterations detected by digital NGS (VAF ≤ 4.6% v VAF > 4.6%; P = .008). (E) Comparisons of ctDNA samples for the levels of IDH mutation detected by ddPCR in baseline and progression samples from the same patient (P = .049) and (F) the levels of IDH mutation detected by digital NGS in baseline and in progression samples from the same patient (P = .06). (G) Kaplan-Meier curves of changes in VAF of IDH-mutated ctDNA during therapy demonstrated no difference in the median TTF between patients with decrease in IDH-mutated ctDNA on therapy compared with increase or no change (0.9 months; 95% CI, 0 to 2.5 v 0.8 months; 95% CI, 0 to 2.1; P = .29), (H) but there was a trend toward a longer median survival in patients with decrease in quantity of IDH-mutated ctDNA compared with patients with no change or increase in IDH-mutated ctDNA (33.1 months; 95% CI, 13 to 53.2 v 9.3 months; 95% CI, 2.1 to 16.4 months; P = .07). ctDNA, circulating tumor DNA; ddPCR, droplet digital polymerase chain reaction; IDH, isocitrate dehydrogenase; NGS, next-generation sequencing; VAF, variant allele frequency; TTF, time to treatment failure.