
Figure 1. Key reproductive exposures associated with future risk of cardiovascular disease in women.
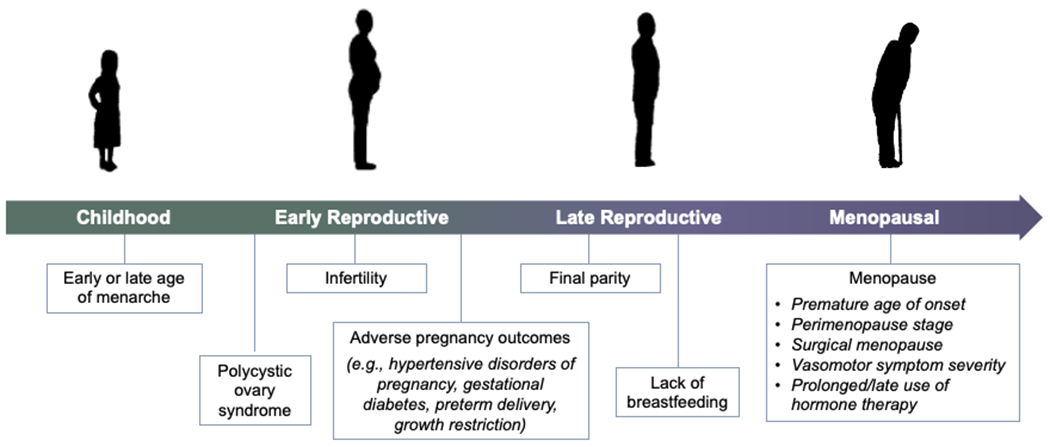
Key stages of a woman’s reproductive history may influence or reveal short- and long-term cardiometabolic and cardiovascular trajectories. Early and late menarche, polycystic ovary syndrome, infertility, adverse pregnancy outcomes (e.g., hypertensive disorders of pregnancy, gestational diabetes, preterm delivery, and intrauterine growth restriction), and absence of breastfeeding may all be adversely associated with a woman’s cardiovascular risk. In addition, the menopause transition represents a period of accelerated cardiovascular disease risk, with timing (e.g., premature menopause), mechanism, and symptoms of menopause, as well as treatment of menopause symptoms, each modifying these risks.