
Fig. 4. Application-specific trend toward increasing medical robot autonomy.
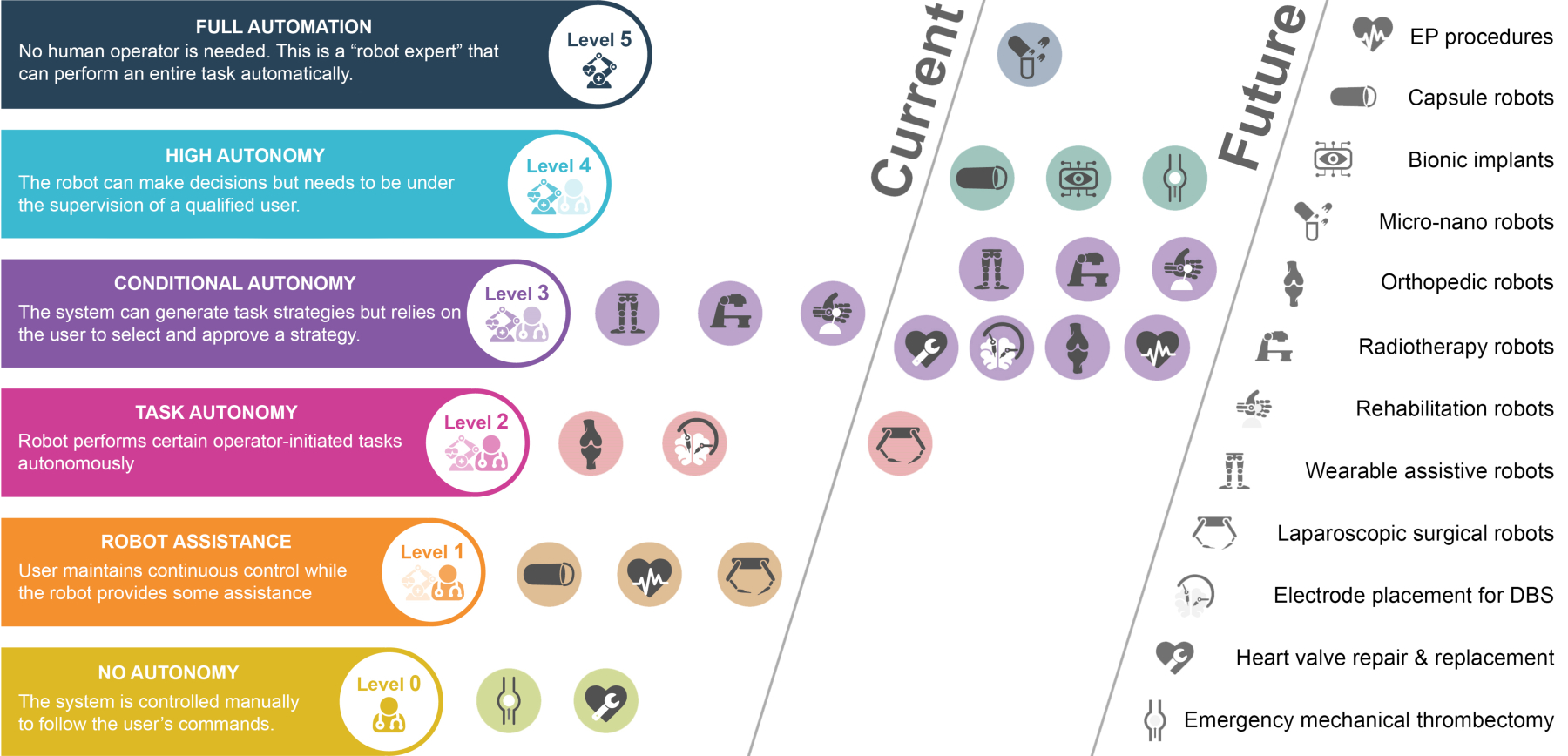
In current use, the level of autonomy is typically the minimum needed to be clinically useful. For example, radiotherapy robots operate at a level of conditional autonomy computing and executing a radiation exposure trajectory to provide the desired radiation dose inside a patient while minimizing exposure of surrounding tissues. Orthopedic robots are capable of autonomously milling out a prescribed cavity for knee and hip implants. In contrast, laparoscopic surgical robots have proven successful under continuous operator control and so currently offer only limited robotic assistance. Transcatheter mechanical thrombectomy and heart valve repair are examples of clinical applications for which robotic solutions have yet to be developed although both could potentially benefit from robotic solutions. In the future, it is anticipated that the level of autonomy of current robotic systems will increase. The biggest increases will be for those applications for which autonomy is vital to their function. For example, highly autonomous systems for remotely performing emergency mechanical thrombectomies to treat stroke would significantly increase the accessibility of this treatment while also decreasing the time to treatment. As a second example, bionic implants which improve or restore body functions will be sufficiently integrated with their host to not require continuous conscious control.