
Fig. 2.
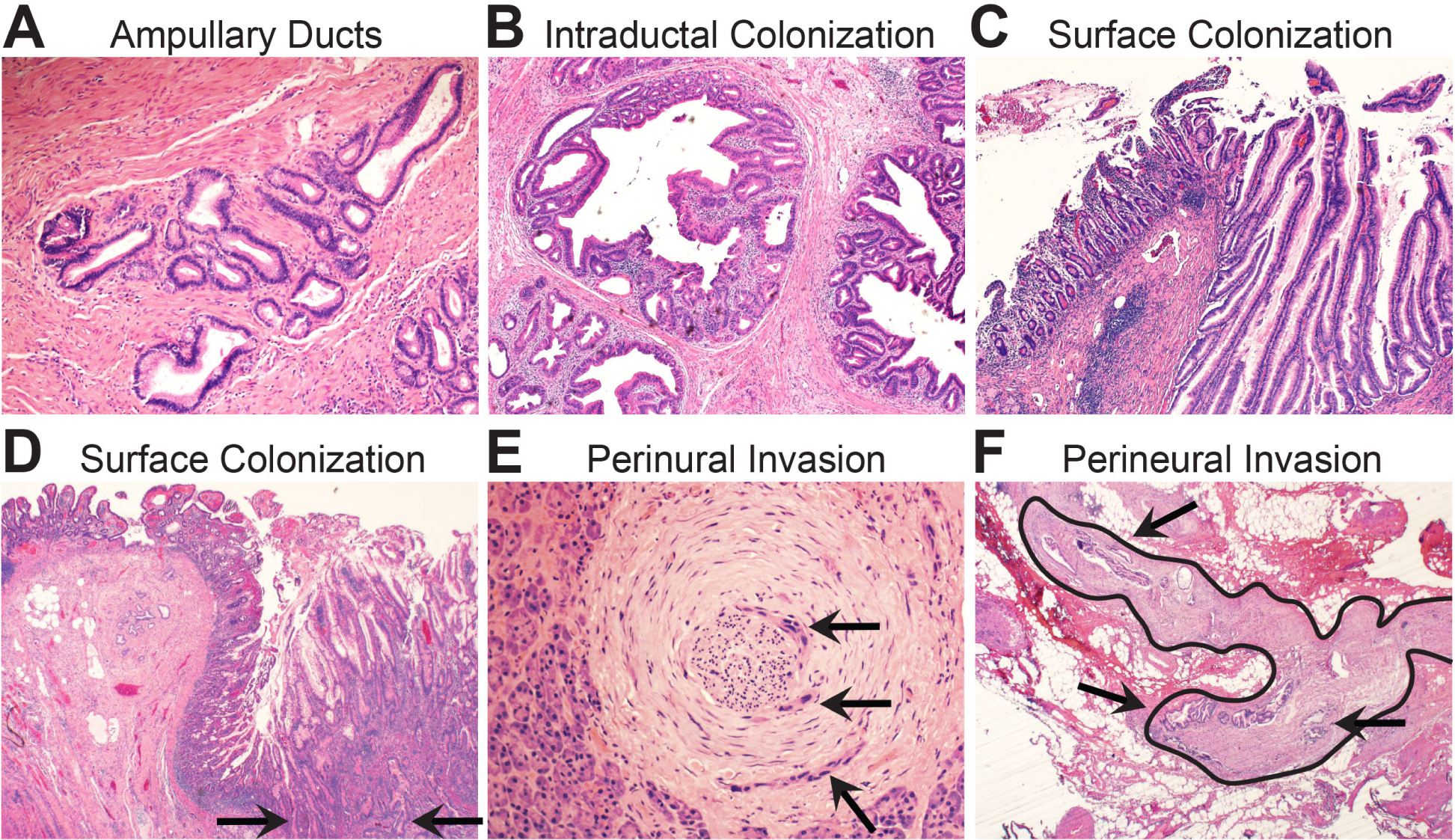
Biomorphology of neoplastic surface spread. (A) Periampullary ducts from the pancreas are situated within the ampullary wall muscle bundles. (B) Intraductal spread of invasive PDAC into the periampullary lumens. (C) An intestinal type intraductal papillary mucinous neoplasm (IPMN) has spread through the periampullary ducts and colonised the surface of the ampullary mucosa. This will mimic an ampullary villous adenoma on a biopsy. (D) Invasive PDAC has invaded directly through the wall of the duodenum (arrows) and colonised the duodenal mucosal surface. This may also simulate a surface adenoma on a biopsy. (E) High power magnification shows focal perineural invasion (arrows) in otherwise normal appearing pancreatic parenchyma. This was a grossly negative resection margin located 1 cm from the primary tumour mass. (F) Low power magnification of peripancreatic fibroadipose tissues shows a large nerve (outlined) with perineural invasion (arrows). This was a frozen section of a resection margin with no grossly identified tumour mass.