

Abstract
BACKGROUND:
The emergency department is one of the most important parts of all hospitals. For this reason, many simulation programs are performed in this department to increase the knowledge, skills, and productivity of health-care workers. The purpose of this study was to identify the benefits of simulation in hospital emergency departments.
MATERIALS AND METHODS:
In the present systematic study, using “AND” and “OR” operators, we searched for the keywords “benefits,” “simulation,” and “hospital emergency department” in PubMed, Web of Science, Scopus, Google Scholar as well as Persian language databases such SID, Magiran, Irandoc, and Iran Medex. Then, a three-step screening process was used to select studies relevant to simulation and hospital emergency from 2005 to 2021 using the PRISMA checklist, and finally, the obtained data were analyzed.
RESULTS:
A total of three main groups, each with several subgroups, were extracted and identified as the benefits of using simulation in hospital emergency departments. They included improving the diagnosis of the disease (rapid prediction of the disease, rapid diagnosis, and patient triage), improving the treatment process (improvement of treatment results, anticipation of admission and discharge of patients, acceleration of interventions, and reduction of medical errors), and improving knowledge and skills (improvement of the speed of decision-making, staff's acquisition of knowledge and skills, simple, convenient, and low-cost training, improvement of staff's preparedness in crisis).
CONCLUSION:
Based on the results of the present study, it is suggested to develop some training programs in order to help staff upgrade their knowledge and performance as well as acquire practical skills and also to improve the diagnosis and treatment process in hospital emergency departments. Virtual methods are also proposed to be applied as potential and cost-effective platforms for learning, teaching, and evaluating the staff of hospital emergency departments.
Keywords: Benefits, emergency department, hospital, simulation, training
Introduction
Simulation is a method used in health-care training to replace or reinforce the patient's actual experiences with different scenarios designed to replicate actual clinical encounters. These experimental learning simulations are designed to evoke or replicate significant aspects of the real world in a fully interactive manner. The simulations allow learners to practice time-sensitive skills without risk to the patient or learner.[1]
The use of computer simulation in the health-care industry to improve staff planning dates back to the late 1970s. Several studies have been conducted to solve the problem of congestion in emergency departments using simulation techniques.[2,3] Simple simulation systems[4] have been used for medical training purposes around the world for many years. The priority in designing modern medical training systems is to maximize patient's safety and minimize the risks to them.[5]
Various methods are used to improve the quality and efficiency of services and flow of patients in the emergency department. Among these methods, the tendency to use computer simulations is increasing to assist in effective decision-making in health care and to improve operations. It seems that computer simulation and specifically the discrete-event simulation method are effective for simulating processes and improving the performance in medical units such as hospitals and they are a suitable replacement with less time and more reasonable cost compared to most traditional statistical methods used in this field.[6]
Providing better training to physicians and medical staff responsible for medical care and treatment of patients, is a major contribution to this fundamental principle. Computer simulation-based training programs which highlight visual assessment, have been successful, confirming that the use of simulation-based training provides a promising ability to gain experiences in a variety of fields.[7]
Emergency departments work 24 h a day, 7 days a week, and their high operating costs are the reason for the lack of funding) and, most importantly, they deal with human health.[6] Therefore, an error in emergency department procedures is likely to lead to disability or death. Several studies over the recent years have shown that the number of people referring to a hospital emergency department has increased to 14 million per year in Canada and more than 15 million per year in the UK[8] and treatment is performed according to this amount of congestion.[9,10] However, the definition of emergency and nonemergency services varies from country to country, patients are classified with different models in different countries to receive emergency, semi-emergency, or nonemergency services.[9,10]
In addition, the high rate of emergency patients and their need for urgent hospitalization and delays in the provision of services not only decrease the level of satisfaction of patients but also minimize resource efficiency in the hospital.[11] In a survey conducted in 2009 on nurses working in hospital emergency departments in Australia, it was shown that nurses had limited training opportunities and this could affect their awareness and self-confidence.[12]
Congestion in a hospital emergency department threatens public health by endangering the patient's safety and the reliability of the entire emergency care system. Although there are different reasons for the congestion of hospital emergency departments, the main reason is the insufficient hospitalization capacity for patients with increasing disease severity. Potential solutions for the congestion of hospital emergency departments require system-level multidisciplinary support.[3]
Therefore, some vital decisions must carefully be made to avoid wasting time and money and providing low-quality treatment. For complex systems such as the emergency department, there is no standard model to help organize system performance and the use of trial and error methods can also be dangerous. Because there may be a gap in face-to-face training among emergency personnel, simulation-based training can be very effective and practical. As a result, simulation methods can become the main approach to organize the emergency department without disrupting its routine.[9] Simulation is one of the decision support techniques, which analyzes risk factors and strategies in decision-making.
Simulations have been used in various health and medical fields and different simulation techniques and simulation-based training programs have attracted attention of many health-care centers over the recent years.[13]
Hospital emergency departments, wherein diagnostic and therapeutic interventions must be performed quickly and continuously, have been encountered with an increase in the number of clients, which has made the usual techniques insufficient and inefficient. Studies indicate that using simulation in the health-care system may have numerous benefits for managers and decision-makers.[6] Hence, using simulations has benefits, reduces human errors as well as time and costs, and improves the speed of service delivery. Therefore, the aim of this study was to identify the benefits of simulation in a hospital emergency department.
Materials and Methods
Study design and setting
The present systematic review that was conducted in the period from 2005 to March 2021 aimed at collecting the information published about the benefits of simulation in the hospital emergency department. To that end, the keywords “benefits,” “simulation,” and “hospital emergency department” were searched in different databases to find relevant articles. The PRISMA statement[14] was used to report the total 349 articles which were found in ProQuest (51), Web of Science (49), Scopus (40), PubMed (110), Google Scholar (50) Iranian databases of medical research: including SID, Magiran, Irandoc, and Civilica, (115) and those other scientific databases were excluded because of overlap with the selected databases mentioned above in terms of the related papers or due to having few relevant articles.
Searching for resources was electronically conducted through the abovementioned scientific databases. Based on the preliminary investigations, all the articles related to the present work were extracted from them.
Information sources and search
The search strategy was defined by merging the words related to benefits, emergency department, and simulation by using operators AND (between word groups) and OR (within each word group). Manual search was also applied to find other reports and documents.
Search strategy
The researchers searched all the articles under Medical Subject Headings (MeSH). The following keywords and terms were accordingly searched. The operators (AND and OR) were used in a database. After searching the strategy at each stage, the Number of Need Record (NNR) was identified. It was searched several times to get the NNR to its score of 12–15, and then, it could be used in search engines. Of course, this must be separately done for each database because tagging is different in each one.
Search concepts and keywords in the PubMed database
([“Emergency department” (ti)] OR [“Emergency Unit” (tiab)] OR [Unit AND Emergency (tiab)] OR [“Emergency Department” (ti)] OR [“Emergency room”] OR [Department AND Emergency] OR [“Emergency Ward”] OR [Ward AND Emergency] OR [Benefit AND “Emergency Department”]) AND ([Advantages (tiab)] OR [Emergency] OR [Emergencies (tiab)] OR [Benefit] OR [Profile]) OR (Advantage [tiab]) ffu OR ([“Emergency department”] OR [“Emergency Unit”] OR [Unit AND Emergency] OR [“Emergency Department”] OR [Department AND Emergency] OR [“Emergency Ward”] OR [Ward AND Emergency] OR [Advantage AND “Emergency Department”]) AND ([Simulation (tiab)] OR [“virtual reality” (ti)] OR [virtual (ti)] OR [“Computer Simulations”] OR [“Computerized Model”] OR [Model AND Computerized]) AND 2005/1/1:2021/1/3(dp).
Therefore, to check each syntax search, the NNRs were specified and attached to the table according to the type of the database. The search syntax and keywords in the database are presented in [Table 1].
Table 1.
Search syntax in the PubMed, Scopus, and Web of Science
| Round | Search syntax | Description | NNR |
|---|---|---|---|
| PubMed | ([“Emergency department” (ti)] OR [“Emergency Unit” (tiab)] OR [Unit AND Emergency (tiab)] OR [“Emergency Department” (ti)] OR [“Emergency room”] OR [Department AND Emergency] OR [“Emergency Ward”] OR [Ward AND Emergency] OR [Benefit AND “Emergency Department”]) AND ([Advantages (tiab)] OR [Emergency] OR [Emergencies (tiab)] OR [Benefit] OR [Profile]) OR (Advantage [tiab]) OR ([“Emergency department”] OR [“Emergency Unit”] OR [Unit AND Emergency] OR [“Emergency Department”] OR [Department AND Emergency] OR [“Emergency Ward”] OR [Ward AND Emergency] OR [Advantage AND “Emergency Department”]) AND ([Simulation (tiab)] OR [“virtual reality” (ti)] OR [virtual (ti)] OR [“Computer Simulations”] OR [“Computerized Model”] OR [Model AND Computerized]) AND 2005/1/1:2021/1/3(dp) | Systematic reviews Books and documents Clinical trials Meta-analysis Reviews randomized trials Controlled trials |
16 |
| Scopus | (TITLE [“Emergency department”] OR TITLE-ABS [“Emergency Unit”] OR ALL [Unit AND Emergency] OR TITLE-ABS [“Emergency Department”] OR TITLE [Advantages] OR TITLE-ABS [Benefit] OR ALL [Department AND Emergency] OR TITLE-ABS [“Emergency Ward”] OR ALL [Ward AND Emergency] OR TITLE-ABS [Advantages AND “Emergency Department”]) AND (TITLE [Benefit] OR ALL [Emergency] OR TITLE [Emergencies] OR TITLE-ABS [“Benefit”] OR ALL [Profile AND Emergency]) OR (TITLE-ABS [“Emergency department”] OR TITLE-ABS [“Emergency Unit”] OR ALL [Unit AND Emergency] OR TITLE-ABS [“Emergency Department”] OR ALL [Department AND Emergency] OR ALL [“Emergency Ward”] OR ALL [Ward AND Emergency] OR ALL [Advantages AND “Emergency Department”]) AND (TITLE [Simulation] OR ALL [modeling] OR TITLE [“virtual reality”] OR TITLE-ABS [virtual] OR ALL [“Computer Simulations”] OR ALL [“Computerized Model”] OR ALL [Model AND Computerized]) AND (PUBYEAR <2021 AND PUBYEAR >2005) | Articles conferences Reviews Chapters books Notes Letters Editorials |
13 |
| Web of Science | (TI=[“Emergency department”]OR TI=[“Emergency Unit”] OR TI=[Unit AND Emergency] OR TS=[“Emergency Department”] OR TS= [Department AND Emergency] OR TI=[“Emergency Ward”] OR TS=[Ward AND Emergency] OR TI=[Accident AND “Emergency Department”]) AND (TI=[Advantages] OR TI=[Emergency] OR TI=[Emergencies] OR TS=[“ Benefit”] OR TI=[Benefit AND Emergency]) OR (TS=[“Emergency department”] OR TS=[“Emergency Unit”] OR TS=[Unit AND Emergency] OR TS=[“Emergency Department”] OR TS= [Department AND Emergency] OR TS=[“Emergency Ward”] OR TS=[Ward AND Emergency] OR TS=[Advantages AND “Emergency Department”]) AND (TI=[Simulation] OR TS= [modeling] OR TI=[“virtual reality”] OR TI=[virtual] OR TS=[“Computer Simulations”] OR TS=[“Computerized Model”] OR TS=[Model AND Computerized]) AND PY=(2005-2021) | Articles Abstracts Reviews Proceedings papers Letters Editorials Early access Corrections Books chapters New items Books reviews Reprints Retracted publications |
15 |
NNR=Number of Need Record, TS=Topic ،TI=Title
Selection of studies
By so doing, articles, summaries, and documents related to the study were collected. The selection of keywords is based on a review of texts and expert opinions. A search of English articles in various databases yielded a total of 349 documents. Bibliographic information (title, author name, journal name, year of publication, period, and number) was entered into EndNote software and duplicates were removed using Find Duplicate. At this point, 200 documents remained after eliminating duplicate studies. The next step was to carefully study the title and abstract to identify documents eligible to enter the study and to remove unrelated documents from the study. At this stage, the titles and abstracts of the articles were obtained and reviewed by two experts in the field of stimulation databases to ensure their relevance to the study area. At this point, 80 articles were selected. The next step was to carefully study the full text of the articles to determine their relevance to the purpose of the research. Thus, 60 unrelated articles for the purpose of research and 10 other duplicate articles were removed. Finally, 10 articles were included in this study [Figure 1].
Figure 1.
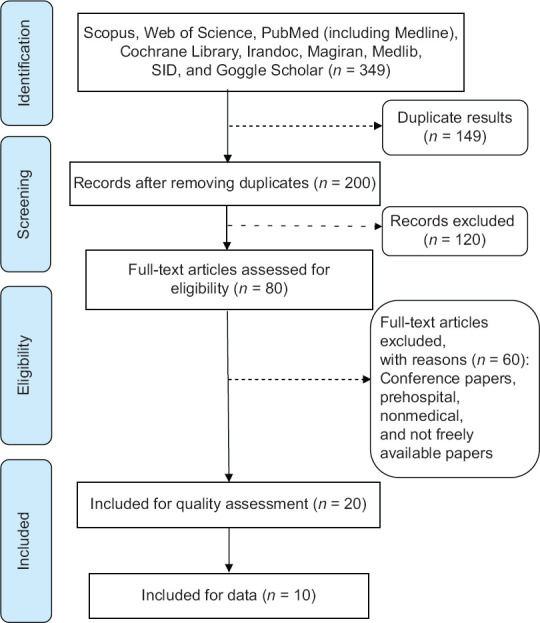
Flow diagram of the final article selection process
Inclusion and exclusion criteria
Articles which were collected in the period from 2005 to 2021 in both English and Persian, discussed the methods, and benefits of simulation-based training in hospital emergency departments, were included criteria in the study. Studies not having the minimum level of quality, narrative reviews, meta-analysis, and case reports discussing prehospital emergency care, prehospital emergency staff training, and prehospital emergency management, gray literature (conference papers) as well as research not considering the benefits of simulation or not being accessible in full texts were excluded criteria from the present study.
Extracting the data
First, the articles were reviewed by two researchers completely independently. They reviewed the title and abstract and considered the inclusion and exclusion criteria. Then, the full text of the articles was reviewed by these experts, and if both rejected the articles, the reason was mentioned, and in case of disagreement between them, these studies were judged by a third researcher. Data extraction was performed using a checklist.
Quality assessment of articles
Regarding the type of studies considered here, the checklist of the Critical Appraisal Skills Programme was used to evaluate the quality of studies.[15] This includes eight different checklists, and the selected checklist here consisted of 10 questions that divided articles into three levels of quality: high, medium, and low and most investigated studies in this systematic review were of the intermediate level.
Results
Out of 349 studies that were reviewed, 10 articles were recognized eligible and related to our goal and thus were analyzed. In the case of groups and subgroups, content analysis of the articles was performed and they were extracted from them. The PRISMA statement was used to report articles [Table 2].
Table 2.
Titles and specifications of articles included in the study for the final review
| Author | Year | Design | Quality | Purposes | Main findings |
|---|---|---|---|---|---|
| Ohu et al.[16] | 2020 | Qualitative | High | Reviewing the applications of artificial intelligence and machine learning to acute care research and highlighting commonly used machine learning techniques | The application of machine learning techniques in acute care research is at its infancy, and the incorporation of artificial intelligence techniques through machine learning can help advance acute care research |
| Wang and Podlinski[24] | 2020 | Qualitative | Moderate | Discussing the current state of hospital-based simulation, including the unprecedented events of the global COVID-19 pandemic | Hospital-based simulation training adds value to health-care systems, but its quantitative and qualitative impacts are required to be more investigated |
| Poore and Cooper[19] | 2021 | Qualitative | Moderate | Addressing interprofessional simulations from both academic and practical perspectives | It leads to education simulation, better understanding of professional roles and responsibilities, development of communication, and teamwork skills |
| Nye[25] | 2020 | Qualitative | High | Presenting an overview of research designs and the Kirkpatrick model used in simulation research | Simulation has a positive impact on changes in knowledge, skills, and attitudes |
| Prion and Haerling[26] | 2020 | Qualitative | Moderate | Providing a brief overview of simulation evaluation | Nursing simulation-based education is increasing to educate health-care professionals, develop and increase their expertise, and help them gain competency in key interprofessional skills |
| Aebersold and Dunbar[27] | 2020 | Qualitative | Moderate | Studying the use of simulation in education and learning | These new technologies should be used in the same way as other learning methodologies as many new ideas and ways of learning are emerging in this area |
| Shafaf and Malek[13] | 2019 | Qualitative | Moderate | Studying the use of artificial intelligence and machine learning techniques in different medical fields, especially emergency medicine | By early prediction and diagnosis of high-risk diseases, such necessary interventions can be performed more rapidly in emergency departments to prevent multiple disease progression complications |
| McGrath et al.[1] | 2015 | Qualitative | High | Studying the computer-based virtual simulation technology widely used in the emergency department | The virtual simulated examination is a feasible alternative to the traditional examination format for emergency patients |
| Karakuş et al.[21] | 2014 | Qualitative | High | Evaluating the effectiveness of computer simulation-based training in improving the last year medical students’ knowledge | Computer simulation-based training will significantly affect the learning of medical treatment algorithms |
| Paul et al.[2] | 2010 | Qualitative | High | Highlighting the contributions of these simulation studies to our understanding of emergency department overcrowding and discussing how simulation can be better used as a tool to address this problem | Simulation studies provide important insights into emergency department overcrowding while having major limitations that must be addressed |
A total of three main groups, each with several subgroups, were identified to be about the simulation of hospital emergency departments. They included improving the diagnosis of the disease (rapid prediction of the disease, rapid diagnosis, and patient triage), improving the treatment process (improvement of treatment results, anticipation of admission and discharge of patients, acceleration of interventions, and reduction of medical errors), and improving knowledge and skills (improvement of the speed of decision-making, staff's acquisition of knowledge and skills, simple, convenient, and low-cost training, and improvement of staff preparedness in crisis) [Table 3].
Table 3.
Findings from the study of the simulation benefits in hospital emergency departments
| Improving the diagnosis of the patient |
| Rapid prediction of the disease[16] |
| Rapid diagnosis of the disease[2] |
| Patient triage[6,17] |
| Improving the treatment process |
| Improvement of treatment results[18] |
| Anticipation of admission and discharge of patients[11] |
| Acceleration of interventions[1,19] |
| Reduction of medical errors[20] |
| Improving knowledge and skills |
| Improvement of the speed of decision-making[16,21] |
| Staff’s acquisition of knowledge and skills[4,12,20] |
| Simple, convenient, and low-cost training[1,22] |
| Improvement of staff preparedness in crisis[21,23] |
Improving the diagnosis of the disease
The rapid growth of technology has led to the development of health programs aimed at treating and preventing a wide range of health conditions. However, there is evidence that the use of simulations in overcrowded environments, including hospital emergency departments, plays an important role in the rapid diagnosis and treatment of the disease.[28]
Rapid prediction of the patient
Simulation-based training can improve the diagnosis of the disease and, consequently, help the patients' treatment and reduce their waiting time in emergency departments. In fact, it can be effective in rapid prediction, diagnosis, and triage. Researchers (2020), in a systematic review of 22 articles published from 2015 to 2019 about the use of simulators in the diagnosis of diseases, showed that artificial intelligence techniques were an excellent method in diagnosing chronic diseases that could affect the quality of patient care and reduce medical costs.[16]
Rapid diagnosis of the patient
Paul in 2010 conducted a systematic study on simulating the emergency department.[29] The study was done in two stages; in the first stage, databases were searched from 1970 to 2006, and in the second stage, resources were reviewed. The results showed that simulation was effective in understanding emergency department congestion and reducing patient waiting time.[2]
Patient triage
Given the importance of the simulation approach, the implementation of a virtual reality-based training program can be effective in improving the performance of nurses in the field of hospital triage.[6] The study conducted by Hartman et al.(2020) with the aim of simulating and triaging the mass casualties, using qualitative data collected from 44 survey participants, showed that the level of stress during the simulation was significantly higher in patients while the confidence significantly increased after the simulation.[17]
Improving the treatment process
Simulation-based training of emergency department staff can improve the treatment process which includes the improvement of treatment results, anticipation of admission and discharge of patients, acceleration of interventions, and reduction of medical errors.
Improvement of treatment results
Abdullah Nofal et al. (2018) conducted a cross-sectional study at a health-care hospital in the center of Riyadh, which aimed at assessing knowledge, practices, and attitudes related to natural and emergency disasters among emergency department staff in order to improve treatment outcomes. To that end, a survey was used to collect data from physicians and nurses. The results showed that the level of health-care providers' knowledge, attitude, practice, and familiarity about disaster preparedness was satisfactory, and also, follow-up was essential to maximize emergency preparedness.
Anticipation of admission and discharge of patients
Ajami et al. (2012) performed a cross-sectional and analytical study to find out the effects of stimulation on the reduction of the patient waiting time in the emergency department. The patient waiting time refers to the length of time a patient waits to receive diagnostic and treatment services in the emergency room. Sometimes, the rescue of a human being depends only on the relief operation being carried out a second earlier, and it is the duty of the emergency to shorten the seconds. Therefore, the speed and accuracy of services in medical centers, especially in the emergency department, to reduce mortality and disability is of particular importance. A basic strategy is to reduce the waiting time for triage or to prioritize patients according to the urgency of the clinical situation.[30] Ajami et al. (2021) A study aimed at Wait Time in Emergency Department (ED) Processes do this study The questionnaires of the mentioned study were sent to 663 patients over a 2-week period. For data analysis, SPSS software was used, showing that the use of simulation was very effective in better management and in reduction of the patient waiting time.[11] Ingrassia et al. (2021) studied the effects of simulation on disaster interventions and training. In this systematic review, after searching the databases and reviewing the found articles, they finally reached 18 articles. The results of this study showed that simulation was an effective training tool in disaster medicine education, and although simulation-based training was a commonly-used method, there was still a lack of uniformity in the use of simulation in hospital emergency departments.[19]
Acceleration of interventions and reduction of medical errors
McGrath et al.(2015) carried out a research on the use of virtual reality for physical examinations and medical interventions in a hospital emergency department and concluded that the virtual simulated oral examination was a practical alternative to the traditional examinations for the assessment of emergency department staff. Virtual environments for examinations and treatment interventions should continue to be explored, especially because they are a cheaper, easier, more accurate, and convenient and, at the same time, a good quality option they are a cheap and more convenient and, at the same time, a good quality option.[1]
Another study entitled “Inter-professional Simulation: From the Classroom to Clinical Practice,[20] revealed that simulation has been widely studied in nursing and medical education and has been proposed as a valuable strategy to increase communication and collaboration between health professionals. Interdisciplinary simulation to create high-performing health-care teams can reduce medical errors and increase patients' safety. Wang et al. (2020) also found that simulation-based training in hospitals needed a new approach. The social realities and performance demands of hospital staff can be better shown in simulation-based training compared with traditional training methods. Hospitals train health-care workers and students through simulation and use the simulation systems and equipment to improve patients' outcomes. Simulation-based training is incorporated into the training programs of health-care workers to prepare them for appropriate action. Simulation is also used to prepare staff for medical emergencies such as active shooting incidents. Although it is known that training based on simulation gives a value to health-care systems, more evidence is required regarding its quantitative and qualitative effects.[24]
Improving knowledge and skills
Other findings highlighted the positive effect of simulation on improving knowledge and skills, which includes the improvement of the speed of decision-making, staff's acquisition of knowledge and skills, simple, convenient, and low-cost training, and improvement of staff preparedness in crisis.
Improvement of the speed of decision-making
Prion and Haerling et al.(2020), in a study focused on simulation evaluation, demonstrated that simulation-based learning experiences and the steady use of simulation-based training could be effective in developing and enhancing key interprofessional skills and practices among health-care professionals. These simulation models could be employed to increase the level of knowledge and skills of health-care staff.[26] Ohu et al.(2020) studied the use of simulators in learning and indicated that artificial intelligence has been successfully utilized in many health-care applications and its use in emergency medicine was expanding. Its advantages included rapid decision-making and the opportunity for working with unstructured data, which increased with access to larger bodies of data. Artificial intelligence algorithms are currently being used to enable faster prediction and diagnosis of diseases and improve patients' outcomes.[16]
Staff's acquisition of knowledge and skills
According to Aebersold et al (2020), who studied virtual reality and skill acquisition in training, the use of simulation in training was a comprehensive part of the curriculum which played an important role in student learning at all levels. Simulation-based training applies a wide range of existing new technologies including virtual reality, use of which involves provision of standard definitions, new research opportunities, and assessment of their impact on learning. Efforts are underway to provide standard definitions and disseminate preliminary findings of conducted research, using these new technologies. There are many available opportunities for educators to incorporate virtual reality into their curriculum and create new simulation-based learning methods. The current state of knowledge and skills shows promising results, and virtual products are growing to increase knowledge and skills. These new technologies should be used in the same way as other learning methods because many new learning ideas and methods are emerging in this field. It is also critical to determine simulation methods and their applications for educators and professors.[4] Michelle et al. (2018) carried out a study on 69 participants, using simulators with the aim of enhancing simulation-based learning. The subjects were divided into two groups: the case group and the control group and then their works were evaluated by a checklist. The results showed that in general, the use of simulators in the control group promoted their learning and understanding compared with those of the other group, improving the learning and skills of hospital emergency department staff.[22]
Simple, convenient, and low-cost training
In a study by Barnes et al. (2017) at the Malawi Hospital, a simulation-based training course was held for emergency department staff. The results showed that, although basic equipment was used in the simulation, very positive feedback was received, indicating that the use of a relatively simple and inexpensive intervention that could be easily continued, might lead to significant improvements in staff skills and consequently patients' outcomes. Therefore, it was found that similar courses in other sections with poor resources could help improve patients' outcomes without significant financial costs and might be more useful and practical than many other health-care measures taken in developing countries.[12]
Improvement of staff preparedness in crisis
In 2014, Karakuş examined computer simulation-based training in a hospital emergency department and concluded that it significantly contributed to the learning of medical treatment algorithms and could improve the success rate of the staff of the hospital emergency department, especially in performing complex medical emergencies.[21]
Duong et al.(2019) also conducted a survey in 2009 on Australian emergency department nurses with 152 participants (60% of whom were responsive), aimed to raise the level of awareness and education in emergencies. The survey was performed in four main areas: (1) training and disaster training, (2) disaster awareness, (3) confidence to respond to a disaster event, and (4) previous experiences. The results of this study revealed that South Australian emergency nurses understood that disaster preparedness decreased. Limited training opportunities and previous experiences of responding to disasters might account for declining disaster awareness and self-confidence among emergency nurses in South Australia. Although 95% of nurses agreed that emergency disaster education was important, 39% of participants had never received disaster training while 63% of participants had never been involved in a disaster response in their careers. Therefore, the nurses' preparedness and self-confidence in emergencies could be directly affected by a combination of previous experiences, natural disasters, and training. Standardizing disaster education and making it available not only increase disaster awareness but also make nurses less vulnerable in the face of unexpected disasters.[31]
Discussion
The simulation technique is a process that helps organizations predict, compare, and optimize the results of their performance and decision-making process, without incurring the cost and risk of changing current processes and new implementation. Therefore, the present study aimed to investigate the benefits of simulation-based training in hospital emergency departments. The results showed that excessive congestion in hospital emergency departments is a global issue that has become even more challenging due to the steady increase in patients' demands, the growing complexity of cases, and the limited resources available in hospitals. This problem is vital to be addressed because the provision of necessary medical services to patients may be delayed due to the congestion and lead to various adverse consequences.[32]
To cope with this problem, research techniques in operations are widely used to analyze and optimize emergency department operations.[32] Emergency department staff are the first staff who address the patients in natural and normal conditions. However, their responsibilities are multiplied in hospital emergencies. Thus, appropriate skills, efficiency, and real capabilities are essential for them to save human lives and improve their health.[18]
To develop and evaluate a multimode simulation-based training program for the staff of hospital emergency departments to increase their competencies in response to incidents, Noh et al.(2108) conducted a study involving 40 participants in October 2016. According to the results, a multimode simulation-based training program must be developed for the staff of hospital emergency departments in a way that all participants significantly improved their disaster response capabilities.[33]
Today, the focus is on simulation-based research as it is the most appropriate way to make important decisions on the patients' flow through the emergency department. The results of the study indicated that education and training was limited due to the lack of realistic evaluation tools. The virtual world provides a platform for education, which raises the level of knowledge, abilities, and skills of health-care staff.[34] The implementation of high-quality care is enhanced by improvement of nursing competencies such as time management skills.[35]
Joing et al. (2020) conducted a descriptive cross-sectional study aimed at developing a computer simulation-based training program for hospital nurses to enhance their competencies in response to disasters. In this work, which was done on emergency department nurses, the Pearson correlation coefficient was used to analyze the data. The assessment of needs, using the modified Delphi method, led to the following competencies in hospital nursing: triage, incident management, hospital capacity management at the time of incidents, and methods of saving in specific circumstances. Each competency was adapted to appropriate simulation methods. Evaluation of the program revealed the improved understanding, disaster management, problem-solving, and technical skills in nurses and increased competencies of nurses in response to disasters. The program developed in this study can be used as an essential tool in future research on curriculum development.[33]
The results of the study showed that emergency departments have usually been responsible for managing the initial response and building capacity. Training is needed so that health-care staff can make an effective response. Assessing the effects of this training is very complex because the real skill can only be demonstrated when there is an emergency patient. The use of computer simulation-based training provides opportunities for nurses to improve management skills and increase their overall self-efficacy.[36]
Different methods are used to improve the quality and efficiency of patients' services and flow in the emergency department. From these methods, the tendency to use computer simulations to assist in effective decision-making in health care and to improve operations is increasing.[37] Furthermore, it was found that the simulation-based training could improve the quality of medical services and provide a framework for modeling other hospital processes, which affected the provision of services to patients.[38]
In a study in 2020, Suhee Jeong et al (2020). examined the knowledge and competencies of 234 clinical nurses working in a public hospital in Korea. The nurses' awareness of emergency codes was measured by recognition and confidence in eight emergency laws, and nursing competencies were assessed using the Disaster Nursing Preparedness Response Competency Scale. The results showed that recognizing emergencies among clinical nurses was associated with their high self-confidence and nursing competencies in disasters. Further studies should develop strategies to improve nurses' awareness and self-confidence in emergencies. Furthermore, for nursing management, special attention should be paid to provide more opportunities for training in natural and human-made disasters to improve nurses' self-confidence and competencies.[39]
This study further indicated that the level of self-confidence as well as practical skills of emergency department staff could be very effective in improving their skills through practical and training methods in a simulated environment. Rivera et al (2019). evaluated and compared the effectiveness of two training interventions of emergency preparedness, using traditional training methods and simulation-based training. They found that integrating simulation-based training into emergency preparedness curricula could improve the knowledge and responsibilities of hospital emergency staff.[38]
Nejadshafiee et al. (2020) in a descriptive cross-sectional study, using questionnaires completed by 142 hospital emergency department staff, showed that in order to improve the main competencies and increase the level of knowledge and skills of the staff, strategies such as ongoing virtual practices and training programs should be used.[39]
Limitations and recommendations
One of the limitations of the present study was the limited scope of search and lack of the adequate number of studies conducted in this field. A small number of simulations in emergency department studies have emphasized the field of simulation-based training in the hospital emergency department and they have been mostly implemented in other fields. Based on the findings of the present study, development of training programs and strategies such as the use of virtual reality in future studies is suggested.
Conclusion
The simulation techniques used to evaluate the systems are a very good tool for improving the quality of a hospital emergency room. On the other hand, using simulation techniques, costs can be predicted and priorities can be determined. Therefore, emergency departments belong to the emergency medical services which represent the most important health-care services and the task of an emergency department is providing health-care services for people who need urgent medical treatments. Therefore, based on the results, simulation-based training workshops and participation of staff in simulations will increase their knowledge, skills, confidence, and preparedness and also save time and resources to face future challenges.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.McGrath J, Kman N, Danforth D, Bahner DP, Khandelwal S, Martin DR, Nagel R, Verbeck N, Way DP, Nelson R. Virtual alternative to the oral examination for emergency medicine residents. Western Journal of Emergency Medicine. 2015 Mar;16(2):336. doi: 10.5811/westjem.2015.1.24344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Paul SA, Reddy MC, DeFlitch CJ. A systematic review of simulation studies investigating emergency department overcrowding. Simulation. 2010;86:559–71. [Google Scholar]
- 3.Trzeciak S, Rivers EP. Emergency department overcrowding in the United States: An emerging threat to patient safety and public health. Emergency medicine journal. 2003 Sep 1;20(5):402–5. doi: 10.1136/emj.20.5.402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Aebersold M, Voepel-Lewis T, Cherara L, Weber M, Khouri C, Levine R, Tait AR. Interactive anatomy-augmented virtual simulation training. Clinical simulation in nursing. 2018 Feb 1;15:34–41. doi: 10.1016/j.ecns.2017.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dikshit A, Wu D, Wu C, Zhao W, Desser TS. Simulation-based training: The next revolution in radiology education. J Am Coll Radiol. 2007;4:816–24. doi: 10.1016/j.jacr.2007.07.013. [DOI] [PubMed] [Google Scholar]
- 6.Delshad V, Shirazi FB. The effectiveness of participation-based education on nurse performance in hospital Triage at disaster. Med Sci. 2019;23:404–9. [Google Scholar]
- 7.Ziba FN, Shirazi FB. Effect of nurses' awareness on myocardial infarction pain management. J Crit Care Nurs. 2017;10(1):e10020. [Google Scholar]
- 8.Yousefi M, Ferreira RP. An agent-based simulation combined with group decision-making technique for improving the performance of an emergency department. Braz J Med Biol Res. 2017;50:e5955. doi: 10.1590/1414-431X20175955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Byars DV, Tozer J, Joyce JM, Vitto MJ, Taylor L, Kayagil T. Emergency Physician-performed transesophageal echocardiography in simulated cardiac arrest. West J Emerg Med. 2017;18:830–4. doi: 10.5811/westjem.2017.5.33543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ajami S, Ketabi S, Yarmohammadian MH, Bagherian H. Wait time in emergency department (ED) processes. Medical Archives. 2012;66(1):53. doi: 10.5455/medarh.2012.66.53-57. [DOI] [PubMed] [Google Scholar]
- 11.Dong S, Lau H, Chavarria C, Alexander M, Cimler A, Elliott JP, Escovar S, Lewin J, Novak J, Lakey JR. Effects of periodic intensive insulin therapy: An updated review. Current Therapeutic Research. 2019 Jan 1;90:61–7. doi: 10.1016/j.curtheres.2019.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shafaf N, Malek H. Applications of machine learning approaches in emergency medicine; a review article. Archives of academic emergency medicine. 2019;7(1) [PMC free article] [PubMed] [Google Scholar]
- 13.Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic reviews. 2015 Dec;4(1):1–9. doi: 10.1186/2046-4053-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Purssell E. Can the Critical Appraisal Skills Programme check-lists be used alongside Grading of Recommendations Assessment, Development and Evaluation to improve transparency and decision-making. Journal of advanced nursing. 2020;76(4):1082–9. doi: 10.1111/jan.14303. [DOI] [PubMed] [Google Scholar]
- 15.Ohu I, Benny PK, Rodrigues S, Carlson JN. Applications of machine learning in acute care research. Journal of the American College of Emergency Physicians Open. 2020 Oct;1(5):766–72. doi: 10.1002/emp2.12156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hartman EN, Daines B, Seto C, Shimshoni D, Feldman ME, LaBrunda M. Sort, assess, life-saving intervention, triage with drone assistance in mass casualty simulation: Analysis of educational efficacy. Cureus. 2020;12:e10572. doi: 10.7759/cureus.10572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nofal A, Alfayyad I, Khan A, Al Aseri Z, Abu-Shaheen A. Knowledge, attitudes, and practices of emergency department staff towards disaster and emergency preparedness at tertiary health care hospital in central Saudi Arabia. Saudi medical journal. 2018;39(11):1123. doi: 10.15537/smj.2018.11.23026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ingrassia PL, Pigozzi L, Bono M, Ragazzoni L, Della Corte F. Disaster Med Public Health Prep. 2021;15:99–104. doi: 10.1017/dmp.2019.111. [DOI] [PubMed] [Google Scholar]
- 19.Poore JA, Cooper DD. Interprofessional Simulation: From the Classroom to Clinical Practice. Annual Review of Nursing Research. 2021 Jan 11;39(1):105–25. doi: 10.1891/0739-6686.39.105. [DOI] [PubMed] [Google Scholar]
- 20.Karakuş A, Duran L, Yavuz Y, Altintop L, Çalişkan F. Computer-based simulation training in emergency medicine designed in the light of malpractice cases. BMC medical education. 2014 Dec;14(1):1–5. doi: 10.1186/1472-6920-14-155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Barnes J, Paterson-Brown L. Improving care of critically unwell patients through development of a simulation programme in a Malawian Hospital. J Educ Train Stud. 2017;5:90–6. [Google Scholar]
- 22.Duong K. Disaster education and training of emergency nurses in South Australia. Aust Emerg Nurs J. 2009;12:86–92. [Google Scholar]
- 23.Wang JC, Podlinski L. Hospital-Based Simulation. Annual Review of Nursing Research. 2021 Jan 11;39(1):83–103. doi: 10.1891/0739-6686.39.83. [DOI] [PubMed] [Google Scholar]
- 24.Nye C. State of Simulation Research in Advanced Practice Nursing Education. Annual Review of Nursing Research. 2021 Jan 11;39(1):33–51. doi: 10.1891/0739-6686.39.33. [DOI] [PubMed] [Google Scholar]
- 25.Prion S, Haerling KA. Evaluation of simulation outcomes. Annu Rev Nurs Res. 2020;39:149–80. doi: 10.1891/0739-6686.39.149. [DOI] [PubMed] [Google Scholar]
- 26.Aebersold M, Dunbar DM. Virtual and augmented realities in nursing education: State of the science. Annu Rev Nurs Res. 2020;39:225–42. doi: 10.1891/0739-6686.39.225. [DOI] [PubMed] [Google Scholar]
- 27.Osei, Ernest, Desmond Kuupiel, Portia Nelisiwe Vezi, Tivani P, Mashamba-Thompson Mapping evidence of mobile health technologies for disease diagnosis and treatment support by health workers in sub-Saharan Africa: A scoping review. BMC Med Inform Decis Mak. 2021;21:11. doi: 10.1186/s12911-020-01381-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Benatti B, Albert U, Maina G, Fiorillo A, Celebre L, Girone N, Fineberg N, Bramante S, Rigardetto S, Dell’Osso B. What happened to patients with obsessive compulsive disorder during the COVID-19 pandemic? A multicentre report from tertiary clinics in northern Italy. Front Psychiatry. 2020;11:720. doi: 10.3389/fpsyt.2020.00720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Golaghaie F, Sarmadian H, Rafiie M, Nejat N. A study on waiting time and length of stay of attendants to emergency department of Vali-e-Asr Hospital, Arak-Iran. J Arak Univ Med Sci. 2008;11:74–83. [Google Scholar]
- 30.Ivanov O, Wolf L, Brecher D, Masek K, Lewis E, Liu S. Improving Emergency Department ESI acuity assignment using machine learning and clinical natural language processing arXiv preprint. arXiv. doi: 10.1016/j.jen.2020.11.001. 200405184 2020 Mar 9. [DOI] [PubMed] [Google Scholar]
- 31.Noh J, Oh EG, Kim SS, Jang YS, Chung HS, Lee O. Development and evaluation of a multimodality simulation disaster education and training program for hospital nurses. International journal of nursing practice. 2020 Jun;26(3):e12810. doi: 10.1111/ijn.12810. [DOI] [PubMed] [Google Scholar]
- 32.Pietsch U, Lischke V, Sollid SJ, Prückner S, Theiler L, Greif R, Albrecht R. Efficacy and efficiency of indoor nighttime human external cargo mission simulation in a high-fidelity training Centre. Scand J Trauma Resusc Emerg Med. 2020;28:61. doi: 10.1186/s13049-020-00755-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Farokhzadian J, Miri S, Doostkami M, Rezahosseini Z, Shahrbabaki PM. Promoting the psychosocial and communication aspects of nursing care quality using time management skills training. Journal of Education and Health Promotion. 2020:9. doi: 10.4103/jehp.jehp_549_20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Jonson CO, Pettersson J, Rybing J, Nilsson H, Prytz E. Short simulation exercises to improve emergency department nurses' self-efficacy for initial disaster management: Controlled before and after study. Nurse Educ Today. 2017;55:20–5. doi: 10.1016/j.nedt.2017.04.020. [DOI] [PubMed] [Google Scholar]
- 35.Salimifard k, Keshtkar L, Moradi M. Improving emergency department performance using simulation. JHOSP. 2014;13:9–15. [Google Scholar]
- 36.Abo-Hamad W, Arisha A. Simulation-based framework to improve patient experience in an emergency department. Eur J Operat Res. 2013;224:154–66. [Google Scholar]
- 37.Jeong S, Lee O. Correlations between emergency code awareness and disaster nursing competencies among clinical nurses: A cross-sectional study. J Nurs Manage. 2020;28:1326–34. doi: 10.1111/jonm.13086. [DOI] [PubMed] [Google Scholar]
- 38.Rivera LR, Rivera CR, Soler AZ, Rivera RP, Rodriguez L, Garcia-Gubern C. The use of simulation games and tabletop exercises in disaster preparedness training of emergency medicine residents. Prehosp Disaster Med. 2019;34:s82. [Google Scholar]
- 39.Nejadshafiee M, Mirzaee M, Aliakbari F, Rafiee N, Sabermahani A, Nekoei-Moghadam M. Hospital nurses’ disaster competencies. Trauma Mon. 2020;25:89–95. [Google Scholar]