
FIGURE 1.
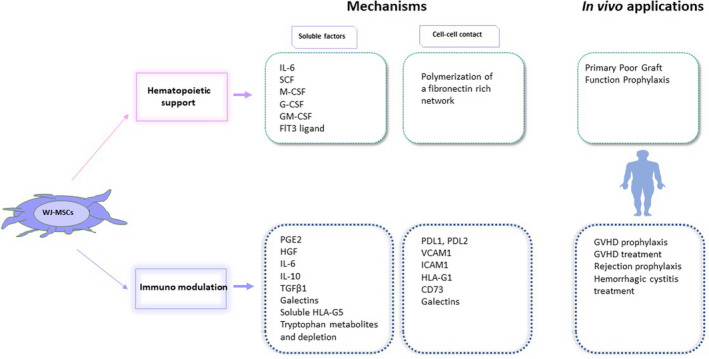
WJ‐MSCs support haematopoiesis and modulate immunity via soluble factors and cell‐cell contact. Upper: WJ‐MSCs secrete growth factors that may enhance haematopoietic cell renewal or stemness, and they may create a fibronectin network that supports haematopoietic cell homeostasis. Thus, they are of interest in the treatment of poor graft function after HSCT. IL‐6: Interleukin‐6, SCF: stem‐cell factor, M‐CSF: macrophage colony‐stimulating factor, G‐CSF: granulocyte colony‐stimulating factor, GM‐CSF: granulocyte macrophage colony‐stimulating factor, Flt3: Fms‐like tyrosine kinase 3; Lower: WJ‐MSCs secrete cytokines and other molecules that decrease activated T‐cell proliferation, or induce Tregs, and act on other immune cells. They also produce cytosolic IDO, an enzyme that depletes tryptophan in the medium and converts tryptophan into secreted metabolites (like kynurenine) that prevent T‐cell proliferation. WJ‐MSCs also express several membrane molecules that interact with activated T cells to induce exhaustion or apoptosis, or to prevent T‐cell activation. The expression of soluble and membrane factors varies according to the level of inflammation in the environment. These properties make WJ‐MSCs good candidates for GVHD prophylaxis or cure, for graft rejection prophylaxis, and for some disorders of uncontrolled inflammation, such as haemorrhagic cystitis. PGE2, prostaglandin E2; HGF, hepatic growth factor; IL, interleukin; TGF β1, transforming growth factor β1; HLA, human leukocyte antigen; PDL (1/2), programmed‐death ligand; VCAM, vascular cell adhesion molecule; ICAM, intercellular adhesion molecule