

Abstract
Objectives
The goals of this study are to identify and analyse interventions that aim to treat post-traumatic stress disorder (PTSD) and complex PTSD in people who are vulnerably housed and to describe how these treatments have been delivered using trauma-informed care.
Design
Scoping review.
Search strategy
We searched electronic databases including MEDLINE, Embase, PsycINFO, CINAHL, the Cochrane Library, Web of Science and PTSDpubs for published literature up to November 2021 for any studies that examined the treatment of PTSD in adults who were vulnerably housed. Websites of relevant organisations and other grey literature sources were searched to supplement the electronic database search. The characteristics and effect of the interventions were analysed. We also explored how the interventions were delivered and the elements of trauma-informed care that were described.
Results
28 studies were included. We identified four types of interventions: (1) trauma focused psychotherapies; (2) non-trauma psychotherapies; (3) housing interventions and (4) pharmacotherapies. The trauma-informed interventions were small case series and the non-trauma focused therapies included four randomised controlled trials, were generally ineffective. Of the 10 studies which described trauma-informed care the most commonly named elements were physical and emotional safety, the experience of feeling heard and understood, and flexibility of choice. The literature also commented on the difficulty of providing care to this population including lack of private space to deliver therapy; the co-occurrence of substance use; and barriers to follow-up including limited length of stay in different shelters and high staff turnover.
Conclusions
This scoping review identified a lack of high-quality trials to address PTSD in people who are vulnerably housed. There is a need to conduct well designed trials that take into account the unique setting of this population and which describe those elements of trauma-informed care that are most important and necessary.
Keywords: adult psychiatry, psychiatry, quality in health care
Strengths and limitations of this study.
First review of how trauma-informed care is being operationalised in the treatment of post-traumatic stress disorder for people who are vulnerably housed.
Largely homogeneous populations (primarily women and US Veterans) included in studies, may not be representative of broader population.
Often no mention of ethnic or cultural factors to consider when providing treatment.
Many of the studies available were of low methodological quality.
Background
People who are vulnerably housed have higher mortality and morbidity rates compared with the general population.1 2 A common vulnerability factor for many disorders is the experience of trauma. It is estimated that as many as 91% of people who are homeless have experienced at least one traumatic event3 and up to 99% have experienced childhood trauma.4 5 A recent qualitative study examining the pathways of men who become homeless long-term in Ontario, found that all of them had experienced complex childhood traumas.6
One consequence of exposure to trauma is either post-traumatic stress disorder (PTSD) or complex PTSD (cPTSD). PTSD results in re-experiencing the event, avoidance of reminders of the event and persistent hypervigilance and awareness of threat. cPTSD results from prolonged threatening events which the individual cannot escape from (such as childhood abuse) and, in addition to PTSD symptoms, results in problems with affect regulation, negative beliefs about oneself and difficulty in sustaining relationships.7 Diagnosed PTSD rates in individuals who are homeless are significantly higher than the Canadian population, ranging between 21% and 53%8–11 which may still be an underestimate of the actual prevalence.
Accessing healthcare poses a unique and difficult challenge in people who are vulnerably housed, and a history of trauma, often perpetrated by people in caring roles such as parents or other family, makes accepting and engaging in treatment difficult.6 12 Being vulnerably housed also exposes people to further traumas and revictimisation, such as further physical or sexual assault and an inability to meet basic needs such as food, safety and personal hygiene.5 13 14 Further, PTSD is often poorly recognised as many people who are vulnerably housed living with PTSD self-medicate with alcohol or other substances. There are also difficulties with accessing appropriate healthcare because of poverty and organisational barriers within healthcare providers.15 These issues result in an underserved population with complex health needs that traditional mental healthcare is poorly equipped to serve.10 16 17 Therefore, providing healthcare services to the vulnerably housed requires a degree of flexibility in terms of how services are provided, who provides them, when, and where. One approach recommended in clinical guidelines is trauma-informed care.18–20
The Substance Abuse and Mental Health Services Administration has defined trauma-informed care as a programme, organisation, or system that realises the widespread impact of trauma and understands potential paths for healing; recognises the signs and symptoms of trauma in staff, clients, and others involved with the system; and responds by fully integrating knowledge about trauma into policies, procedures, practices, and settings.21 In 2010, Hopper18 described the four core principles of trauma-informed care in homeless services as trauma awareness, safety, choice and empowerment and a strengths-based approach. The National Centre on Family Homelessness outlined several reasons why programmes need to be trauma informed,22 including that trauma can impact how people access services, including viewing people and services as unsafe; recognition that people adapt to trauma to keep themselves safe including abusing substances, becoming aggressive, or withdrawing; and, programmes and services cannot be ‘one size fits all’.
None of the five major Clinical Practice Guidelines for the treatment of PTSD23 address the treatment of people who are homeless apart from the National Institute for Health and Care Excellence guidance which states, ‘that methods of access to services take into account the needs of specific populations of people with PTSD, …including people who are homeless’. It does not describe what these methods of access may be. A recent clinical practice guideline for individuals who are homeless and vulnerably housed does not include treatment for PTSD although it does recommend trauma-informed care without defining what this is.20
People who are vulnerably housed are unique among those who have PTSD because of the very high rates of exposure to trauma; the frequent use of substances to self-medicate symptoms; high rates of physical and mental comorbidities; the difficulty of forming caring relationships; and the difficulty of engaging with traditional health services often due to poverty and systemic barriers. We conducted this scoping review to explore the literature on what treatments have been used in this population and how trauma-informed care has been used to deliver these treatments.
Objectives and rationale
This scoping review aims to provide an overview of the literature on the treatment of PTSD and cPTSD in people who are vulnerably housed, how these treatments have been delivered and, if trauma-informed care was used, how that was operationalised.
The specific research questions guiding this scoping review are:
What interventions are described in the literature for the treatment of PTSD and cPTSD in individuals who are vulnerably housed?
Are there any interventions for treatment of PTSD and cPTSD in the vulnerably housed which are described as trauma-informed, and how is this operationalised?
Methods
We conducted a scoping review following the methodological framework proposed by Arksey and O’Malley24 in addition to the methods manual published by the Joanna Briggs Institute’s Methodology for Scoping Reviews.25 Our review also complies with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA) checklist.26 27
Information sources and literature search
A health librarian (AH) conducted electronic database searches in MEDLINE, Embase, PsycINFO (via Ovid), CINAHL (via EBSCO), The Cochrane Library (via Wiley), Web of Science and PTSDpubs (via Proquest) from inception until March 2020, and updated in November 2021. The search was peer reviewed following the Peer Review of Electronic Search Strategies (PRESS) guidelines.28 The full search strategy is available in an additional file (online supplemental appendix 1). No limits to language or publication date were applied. A thorough targeted search of the grey literature was conducted to identify any non-indexed studies including unpublished trial data, dissertations, theses and conference proceedings. The Canadian Agency for Drugs and Technologies in Health Grey Matters Checklist was used to structure our grey literature search as well as identify key websites (ie, organisations that focus on homelessness). We also hand-searched the reference list of identified reports for additional relevant studies that were not captured in the initial search.
bmjopen-2021-051079supp001.pdf (1.1MB, pdf)
Study selection: inclusion criteria
We included published and unpublished primary research studies reporting any quantitative, qualitative, mixed-methods or multimethods research which includes comparative and non-comparative methods evaluating an intervention that looks to treat PTSD in adults (18 years of age or older) who are vulnerably housed. For the purposes of this review, vulnerably housed populations are defined as those who are unsheltered, emergency sheltered, provisionally accommodated, and/or at risk of homelessness.29 Study designs include randomised controlled trials (RCTs), cluster RCTs, quasi-experimental studies, cohort studies, cross-sectional/survey studies, case studies and controlled before and after studies. We excluded reviews, commentaries, and editorials.
Study selection: screening process
The citations from our comprehensive search strategy were uploaded into Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org). The screening process included phase I (titles and abstracts) and phase II (full texts) to identify relevant studies. In both phases, titles were screened by two independent reviewers (AB, KC and MK; NEE in Nov 2021) following the eligibility criteria previously outlined. Prior to each stage of screening, all reviewers ran pilot screening on a random sample of 25 titles and abstracts and 10 full-text studies to identify and address any inconsistencies in applying the inclusion and exclusion criteria. Disagreements between reviewers were resolved by discussion and consultation of a third party (SH) if a consensus could not be reached.
Data abstraction and charting
All included full-text studies were reviewed and abstracted by a single reviewer (AB) using a pilot-tested data abstraction form in Excel. Data that was abstracted included study characteristics, study design, population characteristics, details about the intervention and the trauma-informed approach, and any key findings. A secondary reviewer (KC and MK) verified the abstracted data and any discrepancies between reviewers were resolved through discussion.
The charting process included organising and interpreting data by sifting, categorising, and sorting material according to key issues and themes.24 We charted the data based on intervention type (eg, trauma focused psychotherapies, non-trauma psychotherapies, housing interventions and pharmacotherapy).
We assessed evidence level by the approach outlined by Burns et al in The Levels of Evidence and their role in Evidence-Based Medicine (see Burns et al, p.10, table 4 for Levels of Evidence for Therapeutic Studies).30 We decided if the treatment was delivered by a trauma-informed approach by examining the components as outlined by Hooper et al.18 Studies were marked as ‘Yes’ if they explicitly stated using a trauma-informed approach, while those that used components of a trauma-informed approach, but did not explicitly state a trauma-informed approach were marked as ‘partial’.
Patient involvement
Persons with lived experience were included in the design stage of this project, but were not directly involved with the scoping review.
Results
The electronic search resulted in a total of 2564 citations. We identified one study in our grey literature search. After deduplication, 2522 unique titles and abstracts were screened at phase I, of which 2367 records were excluded, and 154 full-text articles were moved to phase II screening. A total of 28 articles met our inclusion criteria. The details of our selection process are illustrated in our PRISMA flow chart in figure 1.
Figure 1.

PRISMA flow chart of included studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PTSD, post-traumatic stress disorder.
Most studies were conducted in the USA, apart from three studies which were from Canada, Spain and the Netherlands published between the years 1999 and 2020. We identified seven randomised controlled trials (RCT), 1 quasi-RCT, 10 pre–post observational studies, 1 retrospective chart review, 4 case studies, 4 pilot trials and 1 qualitative and quantitative analysis of trial participant focus groups. A description of included studies is provided in table 1.
Table 1.
Summary of study characteristics
| Author (year) | Country | Study design | Sample size | Mean age (SD) | Population | PTSD measurement | Intervention | Intervention length and dose | Was it a trauma-informed approach? | Evidence level |
| Abramovich, (2020)55 | Canada | Case study | 1 | 23 | Trans-woman, recent refugee claimant residing in emergency shelter | Physician made a diagnosis | Pharmacological, psychotherapy | Weekly psychotherapy, daily mirtazapine and prazosin taken at bedtime | Partial, the care team integrated a social determinants of health– based approach into her treatment plan | 4 |
| Bani-Fatemi, (2020)51 | Canada | Pre–post observational study | 70 | 21.47 (3.79) | Homeless female youth (16–24 years old); Gender-based violence | UCLA-PTSD Reaction Index – DSM-5. | Psychoeducation programme | Weekly trauma-informed psychoeducation groups over 16 weeks | Yes | 2B |
| Blitz (2006)52 | USA | Pre–post observational study (Dissertation) | 23 | 28.3 | Black and Latina Women; residing in domestic violence shelter in a large urban centre (NYC) | Self-report using the Davidson Trauma Scale | Psychoeducation, individual therapy sessions, psychiatric consultation, case management meetings | Length of shelter stay (study measured up to 90 days) | Partial, used SELF model | 4 |
| Brewer (2019)49 | USA | Pre–post observational study | 48 | 37.5 | Parents residing in a shelter (Men (25%), Women (75%)), primarily Hispanic/Latinx (62.5%). | Provisional diagnosis for PTSD, as self-reported by the PCL-5 questionnaire. Participants were considered to qualify for a provisional diagnosis of PTSD if they had a total score exceeding 33 points | Psychoeducation, process oriented, and experiential exercises | 9 week intervention. Each group met once per week and each meeting lasted approximately one and a half hours. | Yes | 2B |
| Burns, (2010)44 | USA | RCT | 206 | 40.1 (7.1) | Individuals receiving care at community-based clinic, experiencing homelessness, cocaine dependence, primarily Men (72.3%) | Structured Clinical Interview for the DSM-IV (SCID) (clinician) and Post-traumatic Diagnostic Scale (self-report) | Contingency management for cocaine dependence (behavioural treatment for substance use disorders) | Counselling as needed and weekly goal setting in CM+ | No | 2B |
| Carpenter, (1999)31 | USA | Quasi-RCT (Dissertation) | 10 | 35 | Battered Women residing in a shelter | Not diagnosed, PTSD symptomology was measured pretreatment and post-treatment in each patient with the Impact of Events Scale | Eye Movement Desensitisation and Reprocessing | Following an initial 2 hour session, subjects received up to seven 1 hour sessions on a twice a week basis | No | 1B |
| de Vicente, (2004)34 | Spain | Single arm pilot study | 8 | 47.8 (6.9) | Adults accessing a day centre for homeless in a large urban centre, enrolled; Women (50%) | Two participants were diagnosed with PTSD by using the Composite International Diagnostic Interview, PTSD was diagnosed using ‘Section K’ of the Composite International Diagnostic Interview (CIDI) 2.1 | Written and verbal emotional disclosure | Four 1 hour sessions over 2 weeks | No | 2B |
| Desai, (2008)40 | USA | Pre–post observational study | 643 | 43.3 (8.1) | Female veterans who were homeless or at high risk of becoming homeless; Not receiving VA services>6 weeks | Not diagnosed, PTSD symptomology was measured pretreatment and post-treatment in each patient using PTSD Checklist scores | CBT | The Phase I intervention lasted if women remained residents of the shelter. The Phase II intervention lasted for 6 months. After the baseline interview, follow-up interviews were obtained every 3 months over the course of 1 year | Partial, used Seeking Safety model | 4 |
| Feingold, (2018)42 | USA | Retrospective chart review | 81 | 39.3 (10.98) | Men (53%), Women (48%), Other (1%) who were identified in St. Louis Jail Diversion Programme records | Trauma exposure and post-traumatic distress were evaluated by a clinical interview conducted by trauma therapists and supplemented by patient self report measures using the Diagnostic and Statistical Manual for Mental Disorders Fourth Edition (DSM–IV) and PTSD diagnostic Criterion A event | Cognitive processing therapy, CBT, motivational interviewing | Cognitive Processing Therapy was provided in 12 sessions, CBT was provided in eight sessions, Motivational Interviewing is brief in 3–5 sessions | Yes | 2B |
| Garland, (2016) | USA | RCT | 180 | MORE: 37.7 (10.4) CBT: 36.5 (11.2) TAU: 38.7 (9.8) |
Men with concurrent disorders in a modified therapeutic community programme. | Diagnostic interviews were conducted by a psychiatrist and/or clinical social worker with training in making addiction and psychiatric disorder diagnoses Semi structured psychiatric interview similar to the Mini-International Neuropsychiatric Interview (MINI) and the PCL-C | CCBT | 10 session group interventions at 2 hours each | No | 1B |
| Gorzynski, (2018) | USA | Pre–post observational study (Dissertation) | 63 | 30.7 (7.6) | Women who were homeless but residing in a non-profit inpatient substance use rehab centre. | Self-report, participants were administered the Trauma Symptom Inventory −2 (TSI-2) during the first treatment session | Cognitive-behavioural | 8 sessions for 2 hours each over 4 weeks (1 month, with two sessions per week) | Partial, used Seeking Safety model | 3B |
| Harpaz-Rotem, (2011)53 | USA | Pre–post observational study | 451 | No RT: 43.5 (8.9) RT: 43.9 (6.7) | Female veterans who were homeless or at high risk of becoming homeless; Not receiving VA services>6 weeks | Self-report using the PTSD Symptom Checklist (PCL) was used to assess PTSD symptoms | Residential treatment | Minimum of 30 days residence in the programme | No | 3B |
| Harris, (2019)54 | USA | Pre–post observational study | 421 | 54 (7.52) | Men (71%), Women (28.5%), and Other (0.5%) who were homeless and moved into Permanent Supportive Housing in a large urban centre (LA) | Self-report using the 4‐item Primary Care PTSD Screen | Supportive Housing | Not reported | No | 3B |
| Held, (2015)47 | USA | Pilot study | 47 | 51.3 (8.4) | Male veterans who were homeless and living in transitional housing | Self-report, PTSD Checklist–Specific Stressor Version at baseline | Self-compassion therapy | 4 weeks | No | 2B |
| Helfrich, (2011)50 | USA | Pre–post observational study | 72 | 46.5 | Men (55.6%) and Women (44.4%) living in either emergency housing or single room occupancy programme. | PTSD symptomology was measured pretreatment and post-treatment in each patient with the IES-R (Impact of Event Scale Revised) | Life skills intervention | Not reported | No | 2B |
| Johnson, (2006)38 | USA | Pilot study | 18 | 32 (7) | Women residing in one of 2 eligible shelters and experience of domestic abuse in the month prior | One-week-symptom severity and PTSD diagnostic criteria was assessed by shelter staff using the Clinician Administered PTSD Scale and the Beck Depression Inventory at first presentation | CBT | Twice per week | Partial, used Health to Overcome PTSD through Empowerment (HOPE) model | 3B |
| Johnson, (2009)37 | USA | Case study | 1 | 29 | Woman with experience of IPV residing in a shelter | The patient first presented with significant IPV-related PTSD symptoms and no Axis I (American Psychiatric Association, 1994) comorbidity | CBT | 12 biweekly sessions over 7 weeks | Partial, used HOPE model | 4 |
| Johnson, (2011)36 | USA | RCT | 70 | 32.55 (8) | Women residing in one of 2 eligible shelters and experience of domestic abuse in the month prior | Shelter staff used the Clinician Administered PTSD Scale (CAPS) at first presentation | CBT | 12 sessions, twice weekly that lasted approximately an 1–1.5 hours | Partial, used HOPE model | 1B |
| Johnson, (2016)35 | USA | RCT | 60 | HOPE +SSS: 33.30 (10.48) SSS: 33.20 (10.39) |
Women residing in one of 4 eligible shelters; and experience of IPV in past month | All assessments were conducted by trained and blinded doctoral students in psychology Clinician-Administered PTSD Scale (CAPS) | HOPE, a CBT and empowerment-based individual treatment | Participant received 10 sessions in shelter over 10 weeks and then up to six sessions post shelter for 3 months for a total of 16 sessions throughout the treatment period | Partial, used HOPE model | 1B |
| Johnson, (2020)35 | USA | RCT | 172 | 35.13 (9.12) | Women residing in an eligible shelter; and experience of IPV in past month | Clinician-Administered PTSD Scale | HOPE, a CBT and empowerment-based individual treatment | 16-session intervention during shelter and first 3 months post-shelter | Partial, used HOPE model | 1B |
| Kip, (2016)33 | USA | Pre–post observational study | 117 | 43 (13.2) | Veterans who had been deployed to a major conflict zone, were homeless; primarily Men (92.1%) | A clinical interview and screening that included use of the 17-item Military PTSD Checklist (PCL-M) and PTSD subscale of the 125- item Psychiatric Diagnostic Screening Questionnaire (PDSQ) | Accelerated Resolution Therapy | 1 hour session per week for 1 month | No | 2B |
| Lako, (2018)46 | Netherlands | RCT | 136 | CTI: 34.24 (8.52) TAU: 33.58 (8.08) |
Women residing at a participating shelter ≥6 weeks with an experience of IPV or honor-related violence | Not diagnosed, PTSD symptomology was measured pretreatment and post-treatment in each patient with the Impact of Events Scale | Critical time intervention (CTI) | The duration of each phase was predetermined at 3 months (thus 9 months total for CTI). | No | 1B |
| Lester, (2007)45 | USA | RCT | 206 | CM+: 40.54 (7.35) CM: 40.02 (7.01) |
Individuals receiving care at community-based clinic, experiencing homelessness or at imminent risk of homelessness, and cocaine use disorders; primarily male (CM+: 74% male; CM: 75% male) |
PTSD symptomology was measured pretreatment and post-treatment in each patient with the SCID and PDS | Behavioural day treatment, abstinence contingent housing, and abstinence-contingent vocational training | Phase I (months 1–2), Phase II (months 3–6), Phase III (months 7–12), and Phase IV (months 13–18) | No | 1B |
| Liu-Barbaro, (2015)56 | USA | Case study | 1 | 63 | Man residing at shelter for 5 months | The patient met DSM-IV criteria for PTSD and major depressive disorder | Pharmacological | He was started on treatment with sertraline 50 mg, which was titrated to 150 mg over 1 month, and prazosin 1 mg titrated to 4 mg over 2.5 months. | No | 4 |
| Morrison, (2007)57 | USA | Case study | 1 | 49 | Woman residing in shelter | Not reported | Supportive and pharmacological therapy | Not reported | No | 3B |
| Schueller, (2019)43 | USA | Pilot study | 35 | 19.06 (0.85) | Young adults, aged 18–24, (Men (31%), Women (65%), Transgender (3%)) who were homeless and spent at least 4 of the previous seven nights in a shelter. |
Current symptoms of PTSD were assessed using the 20-item PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders-5 (PCL-5) at baseline and 1 month post intervention | Mobile phone-based therapy (in line with CBT principles) | Three 30 min phone sessions over 1 month | No | 3B |
| Van Voorhees, (2019)48 | USA | Qualitative and quantitative study of focus groups | 22 | 55.2 | Convenience sample of Veterans (sample 100% Men) who were homeless and receiving VA Primary Care services | PTSD was self-reported using a modified version of the Basic Shelter Inventory | Peer mentors | Four focus groups of 5–8 participants over 90 min. Participants had taken part in one of two RCT’s of peer mentoring to deliver primary care. | No | 3B |
| Wong (2019)32 | USA | Pre–post observational study | 5 | Unclear | Men residing for at least 90 days in a men’s shelter for people who use substances working towards sobriety | PTSD symptomology was measured pretreatment and post-treatment in each patient with the SPRINT scale | Flash Technique | Treatment consisted of eight 50 min sessions, 1 session per week (thus lasting 8 weeks total) | Yes | 2B |
CBT, cognitive–behavioural therapy; IPV, intimate partner violence; PTSD, post-traumatic stress disorder.
Research question 1: what interventions are described in the literature for the treatment of PTSD and cPTSD in individuals who are vulnerably housed?
Trauma focused psychotherapies
We identified four studies that used an intervention where participants were asked to recall details of the traumatic events. One non-randomised study evaluated the effectiveness of using eye movement desensitisation and reprocessing (EMDR) in 10 women living in a battered women’s shelter in Michigan.31 Both the five women who received EMDR and the five women who received only the standard shelter programme experienced significant reductions in PTSD symptoms although the reduction was greater in the EMDR group. One case series of five men attending a trauma group in a Californian Homeless Shelter study used the Flash Technique,32 which is part of the preparatory phase of EMDR treatment. Another observational study evaluated the feasibility of using accelerated resolution therapy33 in a cohort of 23 homeless veterans compared with 94 community living veterans in Tampa, Florida. Accelerated resolution therapy involves brief recall of traumatic events, imagery rescripting and some elements of EMDR. About half of individuals who were in the homeless group completed treatment compared with 80% of community veterans. The reasons for non-completion in people who were homeless were moving away from the shelter, conflict with work, and other life circumstances. The authors comment that therapies for individuals who are homeless need to be brief and need to take into account a range of comorbidities and significant life challenges. They also commented on the difficulties of finding a private quiet setting which isn’t always available in a homeless shelter. de Vicente et al34 described a case series of eight people who were homeless, two of whom were diagnosed with PTSD, attending a day centre in Madrid, Spain for people who are homeless. They received an emotional disclosure protocol where participants were asked to write or speak about their thoughts and feelings associated with their trauma.
Non-trauma focused psychotherapies
Johnson et al evaluated a cognitive-behavioural therapy (CBT) and empowerment-based individual treatment called Health to Overcome PTSD through Empowerment (HOPE). They reported a case study, pilot study, and three RCTs in women with PTSD or subthreshold PTSD from ‘battered women’s shelters’ comparing HOPE with ‘standard shelter treatment’.35–38 The HOPE therapy focused on addressing PTSD resulting from intimate partner violence (IPV), while using many traditional components of CBT for PTSD (eg, cognitive-restructuring, skill building) with a focus on stabilisation, safety and empowerment. In the first RCT of 70 people, they found no difference in PTSD outcomes with one in four participants attending all 12 HOPE sessions and about two-thirds attending five or more sessions. Participants were excluded if they were experiencing symptoms of psychosis, suicidal thoughts, had been diagnosed with bipolar disorder or had any change in psychotropic medication in the previous month. In the second RCT of 60 women in shelters, the treatment was continued after the women had left the shelter but again did not find a significant difference in PTSD outcomes. Johnson et al also conducted a third RCT, an expansion of prior RCTs, comparing the HOPE intervention to an adapted version of present-centred therapy (PCT+). They evaluated the efficacy relative to a time- and attention-matched control condition over a 12-month period. Results of multivariate models found that both HOPE and PCT+ were associated with significant and large reductions in IPV related PTSD symptoms. Further, both treatments resulted in significant small to medium effects on IPV, depression, empowerment, post-traumatic cognitions, and health-related quality of life. The study authors found that both HOPE and PCT+ are viable and efficacious treatments of IPV-related PTSD in women residing in shelters.39
Two observational studies aimed to evaluate the effectiveness of a CBT-based group therapy, Seeking Safety, in women who were homeless.40 41 Seeking Safety is a manualised CBT intervention consisting of 25 individual modules that address issues of safe behaviours and relationships, life skills and relapse prevention. In the 2008 observational cohort study, 91 female US veterans who were vulnerably housed were offered Seeking Safety and were compared with a historical cohort of 359 women who did not receive Seeking Safety. It is unclear how many of the women had PTSD but there was a significant decrease in PTSD symptoms over the whole group although the differences were small. The Seeking Safety group significantly increased their drug use. In the 2017 pretest post-test interventional study, 63 women who were homeless in an in-patient residential setting who had been exposed to trauma and had substance use disorders were offered an abbreviated version of Seeking Safety. The abbreviated version was developed in response to criticism that the full version was too long, required high levels of participant commitment, and was unsuitable for ‘transient’ populations. The authors found that after eight 2 hour sessions over 4 weeks there was a significant improvement in perceived self-efficacy in the two-thirds of the sample who completed a minimum of six out of eight sessions. The Veterans Affairs Clinical Practice Guidelines concludes that there is insufficient evidence to recommend for or against Seeking Safety for treatment of PTSD in the general population.
Feingold et al42 reported an observational cohort study of cognitive processing therapy, CBT and motivational interviewing in adults within a US jail diversion programme. About a third of their population of 81 participants were vulnerably housed and 62% were diagnosed with PTSD. The main finding was that about half of the sample did not complete their treatment. Increased completion rates were associated with emergency therapy sessions and the authors comment on the need for flexibility in delivering care to this population. In those who did complete their treatment there was a significant decrease in PTSD symptoms.
Schueller43 reported a single group pilot study evaluating the feasibility and acceptability of a mobile phone-based therapy that used an app designed to help provide coping skills to 35 young adults (18–24 years) recruited from homeless shelters in Chicago. Participants received a mobile phone, a data plan, the app and 1 month of support from a coach consisting of up to three brief sessions. Just over half of the participants completed all three coaching sessions but there were no significant changes in clinical outcomes.
Contingency management
In one unblinded RCT, 187 people who were homeless from Alabama, dependent on cocaine, were randomised to contingency management or contingency management plus. At the start of the study 21 participants had a diagnosis of PTSD. Housing was dependent on negative urine screens for cocaine. There did not appear to be any difference in outcomes between the two groups.44 45
Educational interventions
One RCT examined the effectiveness of a critical time intervention for abused women who were transitioning from women’s shelters to community living.46 Critical time intervention is a time-limited, strengths-based intervention designed to support vulnerable people during transitions in their lives. This study of 136 Dutch women found a significant decrease in PTSD symptoms after 9 months which was mainly due to a reduction in symptoms in non-Dutch speaking women. Another pilot study evaluated the effect of self-compassion therapy compared with stress inoculation on trauma-related guilt and PTSD severity.47 The authors randomised 47 US veterans living in transitional housing to receive workbooks on the different therapies. Symptoms of PTSD did not significantly differ between the two groups after treatment. Twenty of the participants did not complete the workbooks. One qualitative study of 22 homeless US veterans hypothesised that feeling disconnected was associated with poor outcomes in those with PTSD.48 A pretest and post-test study of 8 adults looked to evaluate the treatment effects of Building Bridges, a group-based psychotherapy adapted for parents living in homeless shelters in San Francisco.49 Building Bridges consisted of nine 90 min groups that included psychoeducation, mindfulness and experiential exercises. There was no significant impact on PTSD symptoms. The authors comment on the difficulty of providing groups in a shelter setting because of staff turnover and restrictions, such as length of stay, at different sites. Another pretest post-test study examined the impact of a life skills group and individual programme on 72 individuals who had been recently homeless living in emergency housing.50 Eight out of ten participants reported a history of abuse. Symptoms of PTSD significantly decreased after the intervention. The life skills intervention consisted of one or more modules which focused on food management, money management, room and self-care management and safe community participation. A longitudinal observational study evaluated the changes in quality of life (primary outcome), psychological distress, traumatic symptoms, substance use, resilience, victimisation and sense of mastery (secondary outcomes) in young women experiencing gender-based violence and homelessness in Toronto, Canada after their enrollment in the Peer Education and Connection through Empowerment (PEACE) programme. The PEACE programme is a community-based, trauma-informed, group psychoeducation intervention launched in 2017, for female identified youth aged 16–24 experiencing gender-based violence and homelessness. The programme aims to empower and support survivors of gender-based violence, offering weekly trauma-informed psychoeducation groups over 16 weeks to promote health and well-being. Overall, the study found that after 12 months, quality of life increased significantly among participants (p=0.009), and the 12-month victimisation score was significantly decreased relative to baseline (p=0.05). Changes in other outcomes were not statistically significant. The study authors concluded that a brief, community-based, trauma-informed, group psychoeducation intervention may be helpful in improving the quality of life and reducing experiences of victimisation among female identified youth.51
Housing interventions
We identified three studies that used housing and shelter as a way to provide therapy.52–54 One study used a shelter as a restorative milieu that integrated trauma recovery and social justice empowerment for Black and Latino women in New York.52 This pretest/post-test descriptive and qualitative study of about 20 women found a reduction in PTSD symptoms over time and an appreciation by the residents that the shelter milieu felt safe and nurturing. Another study focused on providing supportive housing to 421 adults who were homeless in Los Angeles.54 This descriptive pretest/post-test study found that about half the sample had probable PTSD at baseline which reduced to 40% at three, six and 12 months. A cohort study of US female veterans who were homeless compared 234 who received at least 30 days of residential treatment with 217 who received less than 30 days. The study was able to follow-up about half the participants after 1 year. The authors found a small but significant improvement in PTSD symptoms in those who received residential treatment.53
Pharmacotherapy
There were three single person case studies describing successful pharmacological treatments.55–57 In one study, a 23-year-old transgender refugee woman in an emergency shelter in Canada was prescribed mirtazapine 60 mg for PTSD and insomnia, and prazosin 6 mg for nightmares.55 Liu-Barbaro and Stein56 describe treating a 63-year-old Ethiopian man living in a homeless shelter with major depressive disorder and PTSD with dissociative symptoms. He was treated successfully with sertraline 150 mg and prazosin 4 mg. The authors note that this patient had suffered for years before being diagnosed and treated.56 Finally, the last study reported a ‘composite case’ of a 49-year-old woman with PTSD prescribed sertraline 150 mg and supportive therapy.57
Research question 2: Are there any interventions for treatment of PTSD and cPTSD in the vulnerably housed which are described as trauma informed, and how is this operationalised?
We identified four studies that explicitly stated using a trauma-informed approach to deliver treatment.32 42 49 51 Two studies did not clearly describe how they operationalised their trauma-informed approach.32 42 One study investigating the Building Bridges intervention described using a trauma-informed approach based on the work by Guarino et al.58 As a result Building Bridges is based on understanding how trauma affects parents’ and children’s cognitions, emotions and behaviours. The authors stressed that emotional safety, and the desire to feel heard, protected, comforted, and understood is an important aspect in treating populations who have experienced trauma. Bani-Fatemi et al conducted a longitudinal observational study of a psychoeducation group intervention, PEACE, which they described as trauma-informed. The PEACE programme is peer led and community-based and was designed using a participatory action framework to return power to those in the programme and a focus on participant safety in the group.51
There were seven studies that did not explicitly state using a trauma-informed approach; however they did describe components of their treatment that align with the concepts of a trauma-informed care.35–38 40 41 52 55 The HOPE intervention focused on the impact of present trauma of interpersonal violence and did not focus on trauma from the past. The research group investigating HOPE used Herman’s59 multistage model of recovery which addresses the treatment needs of battered women and incorporates three stages of recovery: (1) establishing safety, self-care, and protection, (2) remembrance and mourning, and (3) reconnection. The authors also note the importance of flexibility and being available when people are ready to engage.60 Two studies used Seeking Safety40 41 which they describe as based on five central ideas: ‘(1) safety as the priority of this first stage treatment; (2) integrated treatment of PTSD and substance abuse; (3) a focus on ideals; (4) four content areas: cognitive, behavioural, interpersonal, and case management; and (5) attention to therapeutic processes.’ The goals of the treatment are to create an empathetic approach where the clients ‘own’ the trauma, to provide education, to validate the connection between trauma and substance abuse, and to offer safe coping skills to manage the symptoms, impulses, and emotions that often come with these co-occurring disorders. One case study integrated a social determinants of health based approach into the treatment plan.55
Discussion
Despite the high prevalence of PTSD in the vulnerably housed there is little evidence of what is effective treatment. Figure 2 outlines how the 28 studies identified map onto the four components of trauma-informed care. The four trauma-informed interventions were small case series, and the non-trauma focused therapies were generally ineffective with respect to PTSD symptoms, which is consistent with the broader literature. A novel intervention in this population is using housing as an intervention but the impact on PTSD symptoms was relatively modest and the strength of evidence low. A systematic review of permanent supportive housing for people who were homeless found no impact on psychiatric symptoms although there was greater housing stability compared with usual care.61
Figure 2.
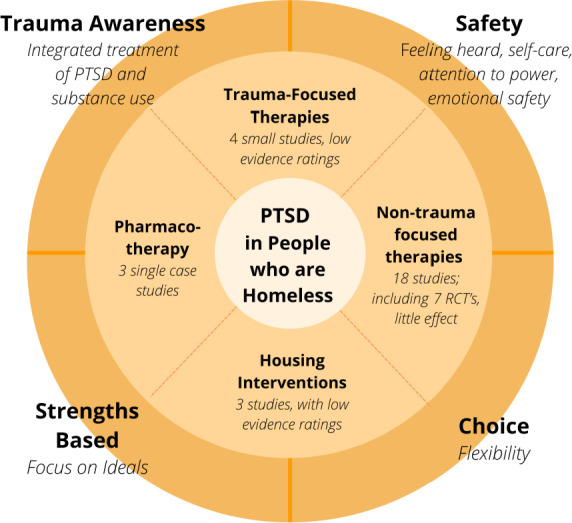
Summary of findings. PTSD, post-traumatic stress disorder; RCTs, randomised controlled trials.
We found three studies that explicitly stated using a trauma-informed approach, while seven described a method that incorporated all or some components of a trauma-informed care approach. Although guidelines and organisations recognise the need for a trauma-informed approach,20 21 58 62 it is unclear how this translates into action or what the most important components are. This review highlights the need to operationalise trauma-informed care and to identify the necessary and most important components in the vulnerably housed. Another area that is unexplored is whether what people with lived experience consider to be trauma-informed care is different to what providers would consider. The impact of an intervention that is trauma-informed is most likely to be seen in increased rates of engagement and completion of treatment.
Guidelines on the treatment of PTSD recommend trauma focused therapies as the most effective interventions. This review clearly identifies a research gap in the application of trauma focused therapies in those who are homeless. The strengths of the studies included in this review demonstrate that it is possible to deliver interventions in this population. However, an important limitation is the difficulty of keeping people in treatment with most studies reporting low engagement with treatment or low follow-up rates. Few studies described what proportion of people agreed to participate in the treatments but the small numbers in most studies suggest that engagement in treatment is difficult. Further the literature in this area is primarily focused on women and US Veterans. Many studies did not mention any ethnic or cultural factors to consider when providing treatment for the vulnerably housed. Also there is a lack of qualitative and experiential data to illustrate any other meaningful changes that may have occurred during treatment. Measuring the effects of trauma in this population can also be difficult as functional improvement such as stopping using substances and stability in housing may paradoxically result in individuals experiencing more PTSD symptoms as they no longer self-medicate. There is also the issue of ongoing exposure to trauma, such as assault, while the person is homeless. Continuing trauma may result in acute stress reactions which could obscure any improvements in PTSD symptoms. Future studies in this population should also ask about recent trauma. Lastly, many of the studies had low levels of evidence and reporting of studies. Although a formal quality assessment was not performed, the levels of evidence were rated for each study and most studies were found to have lower levels of evidence due to small sample sizes or low rates of follow-up. While these studies have added value to the literature, any conclusions made from these studies should be interpreted with caution.
Conclusion
There is currently little evidence on how trauma-informed care for PTSD in the vulnerably housed should be delivered and whether it is effective. A limited number of small trials make interpretation of acceptability, feasibility and effectiveness difficult. Evaluation of interventions should be expanded to include not only symptom improvement, but experiential data informed by the engagement of patients as partners. Measures of symptom severity alone often do not provide a complete picture of the patient experience, excluding factors that may be important such as increased understanding of their illness, skill building, coping and well-being.
This review has also highlighted the need for pragmatic trial designs instead of ‘one-size fits all’ interventions and delivery approaches. The development of a trauma-informed care strategy should be adaptable to multiple cultural or geographical situations to ensure that healthcare providers are able to deliver meaningful, evidence-based care and no individuals are ‘left behind’. Any guidance should include recommendations for implementation or adaptation to ensure fidelity for comparison of effectiveness while allowing for flexibility in delivery.
Managing PTSD or cPTSD and navigating social support systems, including access to effective mental healthcare options, is a significant challenge to people who are vulnerably housed. It can also be challenging for many service providers working with a population where appropriate treatment approaches are poorly understood, under-researched and lack a patient-oriented perspective. It is unclear in this population if treatments for cPTSD need to be different from PTSD. This scoping review has identified several gaps in providing trauma-informed care to a vulnerable population. There is a need to conduct well-designed trials of trauma focused therapies with mixed-methods approaches, focusing on trauma-informed care principles to improve treatments for the vulnerably housed experiencing or at high risk of developing mental health issues. Research needs to clarify which components of trauma informed care are the most important and how to operationalise these.
The main implications from this review for individuals working with this population are that there is no evidence that contradicts recommendations from existing guidelines that trauma focused therapies are effective treatments for PTSD. Trauma focused treatments should be accessible to people who are homeless or vulnerably housed. The delivery of effective interventions should focus on trauma informed approaches with an emphasis on safety, choice, awareness of how trauma affects the acceptability of care and a strengths-based approach.
Supplementary Material
Acknowledgments
We acknowledge that all authors have contributed to this paper mandated by the International Committee of Medical Journal Editors.
Footnotes
Contributors: This research was conceptualised by SH, while AB and NEE contributed to the study design. Search Strategy and searches were completed by AH. While title, abstract and full screenings, and data extraction were carried out by AB, KC, MK and NEE under guidance from SH. Manuscript was drafted by AB, NEE and SH. Critical review of manuscript was undertaken by all authors. SH is the guarantor and accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publish. All authors approved the final manuscript.
Funding: This research was funded by the Canadian Institutes of Health Research (CIHR), Catalyst Grant Program—Strategy for Patient Oriented Research (SPOR). Funding Reference Number 169392.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
This study does not involve human participants.
References
- 1.Fazel S, Khosla V, Doll H, et al. The prevalence of mental disorders among the homeless in Western countries: systematic review and meta-regression analysis. PLoS Med 2008;5:e225. 10.1371/journal.pmed.0050225 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hwang SW. Mortality among men using homeless shelters in Toronto, Ontario. JAMA 2000;283:2152–7. 10.1001/jama.283.16.2152 [DOI] [PubMed] [Google Scholar]
- 3.Buhrich N, Hodder T, Teesson M. Lifetime prevalence of trauma among homeless people in Sydney. Aust N Z J Psychiatry 2000;34:963–6. 10.1080/000486700270 [DOI] [PubMed] [Google Scholar]
- 4.Keane CA, Magee CA, Kelly PJ. Is there complex trauma experience typology for Australian's experiencing extreme social disadvantage and low housing stability? Child Abuse Negl 2016;61:43–54. 10.1016/j.chiabu.2016.10.001 [DOI] [PubMed] [Google Scholar]
- 5.Taylor KM, Sharpe L. Trauma and post-traumatic stress disorder among homeless adults in Sydney. Aust N Z J Psychiatry 2008;42:206–13. 10.1080/00048670701827218 [DOI] [PubMed] [Google Scholar]
- 6.Woodhall-Melnik J, Dunn JR, Svenson S, et al. Men’s experiences of early life trauma and pathways into long-term homelessness. Child Abuse Negl 2018;80:216–25. 10.1016/j.chiabu.2018.03.027 [DOI] [PubMed] [Google Scholar]
- 7.Giourou E, Skokou M, Andrew SP, et al. Complex posttraumatic stress disorder: the need to consolidate a distinct clinical syndrome or to reevaluate features of psychiatric disorders following interpersonal trauma? World J Psychiatry 2018;8:12–19. 10.5498/wjp.v8.i1.12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Whitbeck LB, Armenta BE, Gentzler KC. Homelessness-Related traumatic events and PTSD among women experiencing episodes of homelessness in three U.S. cities. J Trauma Stress 2015;28:355–60. 10.1002/jts.22024 [DOI] [PubMed] [Google Scholar]
- 9.Carlson EB, Garvert DW, Macia KS, et al. Traumatic stressor exposure and post-traumatic symptoms in homeless veterans. Mil Med 2013;178:970–3. 10.7205/MILMED-D-13-00080 [DOI] [PubMed] [Google Scholar]
- 10.Baggett TP, O'Connell JJ, Singer DE, et al. The unmet health care needs of homeless adults: a national study. Am J Public Health 2010;100:1326–33. 10.2105/AJPH.2009.180109 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Torchalla I, Strehlau V, Li K, et al. Posttraumatic stress disorder and substance use disorder comorbidity in homeless adults: prevalence, correlates, and sex differences. Psychol Addict Behav 2014;28:443–52. 10.1037/a0033674 [DOI] [PubMed] [Google Scholar]
- 12.Gordon AC, Lehane D, Burr J, et al. Influence of past trauma and health interactions on homeless women's views of perinatal care: a qualitative study. Br J Gen Pract 2019;69:e760–7. 10.3399/bjgp19X705557 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kim MM, Ford JD, Howard DL, et al. Assessing trauma, substance abuse, and mental health in a sample of homeless men. Health Soc Work 2010;35:39–48. 10.1093/hsw/35.1.39 [DOI] [PubMed] [Google Scholar]
- 14.Shelton KH, Taylor PJ, Bonner A, et al. Risk factors for homelessness: evidence from a population-based study. Psychiatr Serv 2009;60:465–72. 10.1176/ps.2009.60.4.465 [DOI] [PubMed] [Google Scholar]
- 15.Omerov P, Craftman Åsa G, Mattsson E, et al. Homeless persons' experiences of health- and social care: a systematic integrative review. Health Soc Care Community 2020;28:1–11. 10.1111/hsc.12857 [DOI] [PubMed] [Google Scholar]
- 16.Argintaru N, Chambers C, Gogosis E, et al. A cross-sectional observational study of unmet health needs among homeless and vulnerably housed adults in three Canadian cities. BMC Public Health 2013;13:1–9. 10.1186/1471-2458-13-577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fountain J, Howes S, Strang J. Unmet drug and alcohol service needs of homeless people in London: a complex issue. Subst Use Misuse 2003;38:377–93. 10.1081/JA-120017378 [DOI] [PubMed] [Google Scholar]
- 18.Hopper EK, Bassuk EL, Olivet J. Shelter from the storm: Trauma-Informed care in homelessness services settings. Open Health Serv Policy J 2010;3:80–100. 10.2174/1874924001003010080 [DOI] [Google Scholar]
- 19.Dinnen S, Kane V, Cook JM. Trauma-Informed care. Prof Case Manag 2014;19:161–70. 10.1097/NCM.0000000000000038 [DOI] [PubMed] [Google Scholar]
- 20.Pottie K, Kendall CE, Aubry T, et al. Clinical guideline for homeless and vulnerably housed people, and people with lived homelessness experience. CMAJ 2020;192:E240–54. 10.1503/cmaj.190777 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.SAMHSA . SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach, 2014. [Google Scholar]
- 22.Purbeck CA, Briggs EC, Tunno AM, et al. Trauma-informed measurement-based care for children: implementation in diverse treatment settings. Psychol Serv 2020;17:311–22. 10.1037/ser0000383 [DOI] [PubMed] [Google Scholar]
- 23.Hamblen JL, Norman SB, Sonis JH, et al. A guide to guidelines for the treatment of posttraumatic stress disorder in adults: an update. Psychotherapy 2019;56:359–73. 10.1037/pst0000231 [DOI] [PubMed] [Google Scholar]
- 24.Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005;8:19–32. 10.1080/1364557032000119616 [DOI] [Google Scholar]
- 25.Peters MDJ, Godfrey CM, Khalil H, et al. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc 2015;13:141–6. 10.1097/XEB.0000000000000050 [DOI] [PubMed] [Google Scholar]
- 26.Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med 2018;169:467–73. 10.7326/M18-0850 [DOI] [PubMed] [Google Scholar]
- 27.Bennett A, Edgar NEE, Hodgson A, et al. Interventions to treat post-traumatic stress disorder (PTSD) in vulnerably housed populations: a protocol for a scoping review 2020osf.io/mpjgn [DOI] [PMC free article] [PubMed]
- 28.McGowan J, Sampson M, Salzwedel DM, et al. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol 2016;75:40–6. 10.1016/j.jclinepi.2016.01.021 [DOI] [PubMed] [Google Scholar]
- 29.Gaetz S, Barr C, Friesen A. Canadian definition of homelessness. Toronto: Canadian Observatory on Homelessness Press, 2012: 1–5. https://www.homelesshub.ca/sites/default/files/COHhomelessdefinition.pdf [Google Scholar]
- 30.Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg 2011;128:305–10. 10.1097/PRS.0b013e318219c171 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Carpenter MN. Eye movement desensitization and reprocessing in battered women: alleviation of post-traumatic stress disorder, 1999. Available: https://www.proquest.com/openview/539b9f05735e14b833e9e989618c227d/1?pq-origsite=gscholar&cbl=18750&diss=y
- 32.Wong S-L. Flash technique group protocol for highly dissociative clients in a homeless shelter: a clinical report. J EMDR Prac Res 2019;13:20–31. 10.1891/1933-3196.13.1.20 [DOI] [Google Scholar]
- 33.Kip KE, D'Aoust RF, Hernandez DF, et al. Evaluation of brief treatment of symptoms of psychological trauma among veterans residing in a homeless shelter by use of Accelerated Resolution Therapy. Nurs Outlook 2016;64:411–23. 10.1016/j.outlook.2016.04.006 [DOI] [PubMed] [Google Scholar]
- 34.de Vicente A, Muñoz M, Pérez-Santos E, et al. Emotional disclosure in homeless people: a pilot study. J Trauma Stress 2004;17:439–43. 10.1023/B:JOTS.0000048958.99820.39 [DOI] [PubMed] [Google Scholar]
- 35.Johnson DM, Johnson NL, Perez SK, et al. Comparison of adding treatment of PTSD during and after shelter stay to standard care in residents of battered women's shelters: results of a randomized clinical trial. J Trauma Stress 2016;29:365–73. 10.1002/jts.22117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Johnson DM, Zlotnick C, Perez S. Cognitive behavioral treatment of PTSD in residents of battered women's shelters: results of a randomized clinical trial. J Consult Clin Psychol 2011;79:542–51. 10.1037/a0023822 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Johnson DM, Zlotnick C. Hope for battered women with PTSD in domestic violence shelters. Prof Psychol Res Pr 2009;40:234–41. 10.1037/a0012519 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Johnson DM, Zlotnick C. A cognitive-behavioral treatment for battered women with PTSD in shelters: findings from a pilot study. J Trauma Stress 2006;19:559–64. 10.1002/jts.20148 [DOI] [PubMed] [Google Scholar]
- 39.Johnson DM, Zlotnick C, Hoffman L. A randomized controlled trial comparing hope treatment and Present-Centered therapy in women residing in shelter with PTSD from intimate partner violence. Psychol Women Q 2020;44:539–53. 10.1177/0361684320953120 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Desai RA, Harpaz-Rotem I, Najavits LM, et al. Impact of the seeking safety program on clinical outcomes among homeless female veterans with psychiatric disorders. Psychiatr Serv 2008;59:996–1003. 10.1176/ps.2008.59.9.996 [DOI] [PubMed] [Google Scholar]
- 41.Gorzynski A. ‘ I Think I Can, I Think I Can…’ Seeking Safety and Its Effect on Self-Efficacy in Addicted and Trauma-Exposed Individuals, 2019. Available: https://www.proquest.com/openview/a33d9b0f05ee8c47ccebbd573b78ce1b/1?pq-origsite=gscholar&cbl=18750
- 42.Feingold ZR, Fox AB, Galovski TE. Effectiveness of evidence-based psychotherapy for posttraumatic distress within a jail diversion program. Psychol Serv 2018;15:409–18. 10.1037/ser0000194 [DOI] [PubMed] [Google Scholar]
- 43.Schueller SM, Glover AC, Rufa AK, et al. A mobile phone-based intervention to improve mental health among homeless young adults: pilot feasibility trial. JMIR Mhealth Uhealth 2019;7:e12347. 10.2196/12347 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Burns MN, Lehman KA, Milby JB, et al. Do PTSD symptoms and course predict continued substance use for homeless individuals in contingency management for cocaine dependence? Behav Res Ther 2010;48:588–98. 10.1016/j.brat.2010.03.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lester KM, Milby JB, Schumacher JE, et al. Impact of behavioral contingency management intervention on coping behaviors and PTSD symptom reduction in cocaine-addicted homeless. J Trauma Stress 2007;20:565–75. 10.1002/jts.20239 [DOI] [PubMed] [Google Scholar]
- 46.Lako DAM, Beijersbergen MD, Jonker IE, et al. The effectiveness of critical time intervention for abused women leaving women's shelters: a randomized controlled trial. Int J Public Health 2018;63:513–23. 10.1007/s00038-017-1067-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Held P, Owens GP. Effects of self-compassion workbook training on trauma-related guilt in a sample of homeless veterans: a pilot study. J Clin Psychol 2015;71:513–26. 10.1002/jclp.22170 [DOI] [PubMed] [Google Scholar]
- 48.Van Voorhees EE, Resnik L, Johnson E, et al. Posttraumatic stress disorder and interpersonal process in homeless veterans participating in a peer mentoring intervention: associations with program benefit. Psychol Serv 2019;16:463–74. 10.1037/ser0000231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Brewer TA. Building bridges: a trauma-informed relational intervention for parents experiencing homelessness, 2019. [Google Scholar]
- 50.Helfrich CA, Peters CY, Chan DV. Trauma symptoms of individuals with mental illness at risk for homelessness participating in a life skills intervention. Occup Ther Int 2011;18:115–23. 10.1002/oti.308 [DOI] [PubMed] [Google Scholar]
- 51.Bani-Fatemi A, Malta M, Noble A, et al. Supporting female survivors of gender-based violence experiencing homelessness: outcomes of a health promotion Psychoeducation group intervention. Front Psychiatry. : 2020;11:601540. 10.3389/fpsyt.2020.601540 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Blitz L. Using a culturally competent multicultural framework for trauma recovery milieu therapy with black and Latina women in a domestic violence shelter: an evaluation of services. ProQuest Diss Theses 2006:393 http://ezproxy.lib.ryerson.ca/login?url=http://search.proquest.com/docview/305358151?accountid=13631%5Cnhttp://sfx.scholarsportal.info/ryerson??url_ver=Z39.88-2004&rft_val_fmt=info:ofi/fmt:kev:mtx:dissertation&genre=dissertations+&+theses&sid=ProQ:ProQues [Google Scholar]
- 53.Harpaz-Rotem I, Rosenheck RA, Desai R. Residential treatment for homeless female veterans with psychiatric and substance use disorders: effect on 1-year clinical outcomes. J Rehabil Res Dev 2011;48:891–900. 10.1682/JRRD.2010.10.0195 [DOI] [PubMed] [Google Scholar]
- 54.Harris T, Rhoades H, Duan L, et al. Mental health change in the transition to permanent supportive housing: the role of housing and social networks. J Community Psychol 2019;47:1834–49. 10.1002/jcop.22230 [DOI] [PubMed] [Google Scholar]
- 55.Abramovich A, Lam JSH, Chowdhury M. A transgender refugee woman experiencing posttraumatic stress disorder symptoms and homelessness. CMAJ 2020;192:E9–11. 10.1503/cmaj.190974 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Liu-Barbaro D, Stein M. Psychopharmacologic treatment of dissociative fugue and PTSD in an Ethiopian refugee. J Clin Psychiatry 2015;76:958. 10.4088/JCP.14cr09334 [DOI] [PubMed] [Google Scholar]
- 57.Morrison A, McIlduff B. Re-Emergence of symptoms of posttraumatic stress disorder in a homeless woman. Psychiatry 2007;4:60–4. [PMC free article] [PubMed] [Google Scholar]
- 58.Guarino K, Soares P, Konnath K, et al. Trauma-Informed organizational toolkit, 2009. Available: https://www.air.org/sites/default/files/downloads/report/Trauma-Informed_Organizational_Toolkit_0.pdf [Accessed 3 Nov 2020].
- 59.Herman JL. Trauma and recovery. New York: Basic, 1992. [Google Scholar]
- 60.Johnson D, Zlotnick C, Perez S. Helping to overcome PTSD through Empowerment. Available: www.nationalcenterdvtraumamh.org [Accessed 2 Dec 2020].
- 61.Aubry T, Bloch G, Brcic V, et al. Effectiveness of permanent supportive housing and income assistance interventions for homeless individuals in high-income countries: a systematic review. Lancet Public Health : 2020;5:e342–60. 10.1016/S2468-2667(20)30055-4 [DOI] [PubMed] [Google Scholar]
- 62.Gaetz S, Dej E. A new direction: a framework for homelessness prevention.. Toronto: Canadian Observatory on Homelessness Press; 2017. https://homelesshub.ca/sites/default/files/attachments/COHPreventionFramework_1.pdf [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2021-051079supp001.pdf (1.1MB, pdf)
Data Availability Statement
Data sharing not applicable as no datasets generated and/or analysed for this study. All data relevant to the study are included in the article or uploaded as online supplemental information.