

Abstract
Although an inverse relation between social support and psychological distress among chronic pain patients has been previously reported, little is known about what mediates this association. We examined mindfulness as a mediator of the relationship between social support and psychological distress. In this cross-sectional study, chronic pain patients (N=94) completed assessments of social support, mindfulness, and psychological distress. Greater social support was associated with less psychological distress. Greater mindfulness was associated with greater social support and less psychological distress. Mediation analyses demonstrated that mindfulness partially mediated the relationship between social support and psychological distress. Findings support and extend prior research by demonstrating a potentially important mediating effect of mindfulness within chronic pain patients. This suggests an important link between social support and mindfulness, and that their integration in the pursuit of mental health should be considered in future behavioral interventions.
Keywords: social support, mindfulness, anxiety, depression, psychological distress, chronic pain
1. Introduction
The mental and physical health benefits of social support have been demonstrated among various populations, including those with chronic pain (Harandi et al., 2017; Holt-Lunstad & Smith, 2012). During the COVID-19 pandemic, the global prevalence of psychological distress has increased among the general population (Mahmud et al., 2022). Individuals with chronic pain appear to be at particular risk for experiencing psychological distress, with impaired coping impacting quality of life (Piraccini et al., 2020). Chronic pain patients across countries who reported diminished social support during the pandemic reported greater distress (Serrano-Ibáñez et al., 2021) and worsened pain symptoms (Hruschak et al., 2021). There is a gap in knowledge of how social support protects against psychological distress among chronic pain patients. Chronic pain is often comorbid with psychopathology (Dersh et al., 2002), which can lead to a host of other maladaptive pain-related cognitions (e.g., pain catastrophizing) and worsen the experience of pain. Understanding how social support serves as a protective factor against psychological distress, especially during times of heightened social isolation, is important for identifying ways to promote better mental health among individuals with chronic pain.
Researchers have conceptualized an integrative model of social support, suggesting that social support can reduce distress through various pathways, three of which are emotional state (e.g.,decreased negative affect), appraisals of events (e.g.,positive appraisals), and situational-relevant behaviors (e.g.,effective coping strategies) (Feeney & Collins, 2014). Mindfulness, as a psychosocial construct that aligns with these three pathways, may serve as a mechanistic link between social support and decreased distress (Wilson et al., 2020). Mindfulness involves awareness of and ability to regulate experiences in the present moment, without judgment (Feldman et al., 2007). Mindfulness is consistently associated with less psychological distress (Baer, 2003). Importantly, mindfulness is also associated with greater social support (Klainin-Yobas et al., 2016; Wilson et al., 2020).
Our previous investigation in healthy adults revealed that mindfulness partially accounted for the link between social support and less distress, providing initial evidence that mindfulness is a mechanism through which social support may exert its psychological benefits (Wilson et al., 2020). However, this has not yet been tested among individuals with chronic pain, nor has mindfulness been investigated within the context of significant COVID-19-related stressors, where social distancing mandates disrupted many systems of social support. It is important to further investigate because mindfulness-based interventions (MBIs) can be used as stand-alone treatment or in combination with other treatment modalities to reduce psychological distress and opioid consumption (Majeed et al., 2018).
This cross-sectional study examined the extent to which social support was related to psychological distress in a cohort of chronic pain patients after a year of intermittent social distancing during the COVID-19 pandemic. Further, we explored whether mindfulness explained the association between social support and psychological distress.
2. Methods
2.1. Participants and Procedure
A sample of U.S. adults with chronic pain (N=94) completed an online survey from May 21-June 7, 2021. Patients were eligible to participate if they had persistent pain (≥ 3 months), were ≥ 18 years of age and English speaking, and were a resident of Massachusetts (Hruschak et al., 2021). The majority of patients (Mage=41.77, SD=16.23, range:21–77) were female (78.7%) and White (81.9%).
The study was part of a larger study investigating the impact of social distancing guidelines on pain during the COVID-19 pandemic, and was approved by the Partners Institutional Review Board. Patients provided electronic consent before completing validated surveys, which took approximately 30–45 minutes. Patients were compensated with a $20 Amazon electronic gift code for their participation.
2.2. Measures
Social support was measured using the 12-item Multidimensional Scale of Perceived Social Support (Zimet et al., 1988). Each item was rated on a scale from (1=very strongly disagree, 7=very strongly agree). Items were summed and higher scores indicated greater social support.
Mindfulness was measured with the 10-item Cognitive and Affective Mindfulness Scale – Revised (Feldman et al., 2007). Each item was rated on a scale from (1=rarely/not at all, 4=almost always). One item was reverse coded, and items were averaged. Higher scores reflected greater levels of mindfulness.
Anxiety was measured using the 7-item anxiety short form from the Patient Reported Outcome Measurement Information System (PROMIS; Cella et al., 2010). Patients indicated the frequency with which they experienced anxiety symptoms on a scale from (1=never, 5=always). Items were summed, and higher scores indicated greater anxiety.
Depression was assessed using the 8-item depression short form from the PROMIS. On a scale from (1=never, 5=always), patients indicated the frequency with which they experienced depressive symptoms. Items were summed, and higher scores indicated greater depression.
Stress was measured using the 10-item Perceived Stress Scale (Cohen et al., 1994). On a scale from (0=never, 4=very often), patients indicated the frequency with which they experienced symptoms of stress. Appropriate items were reverse coded, and items were summed. Higher scores reflected greater stress.
Ten items from the Brief Pain Inventory (Cleeland & Ryan, 1991) assessed how pain interfered with patients’ lives. Each item was rated on a scale from (0=did not interfere at all, 10=completely interfered). Items were summed, and higher score indicated greater pain interference. Because pain interference is associated with higher levels of psychological distress (Ryan & McGuire, 2016), it was explored as a potential covariate.
3. Results
Means, standard deviations, and Cronbach’s alphas for each variable are reported in Table 1. Spearman correlations for continuous variables and Mann-Whitney U tests for categorical variables assessed the associations among key study variables and potential covariates (Table 1). Greater social support was associated with higher levels of mindfulness and lower levels of psychological distress. Greater mindfulness was associated with less psychological distress.
Table 1.
Means, standard deviations, Cronbach’s alphas, and Spearman correlations.
| Social support | Mindfulness | Depression | Anxiety | Stress | Pain interference | |
|---|---|---|---|---|---|---|
|
| ||||||
| Social support | - | |||||
| Mindfulness | 39** | - | ||||
| Depression | −.45** | −.43** | - | |||
| Anxiety | −.38** | −.45** | .79** | - | ||
| Stress | −.42** | −.46** | 74** | .76** | - | |
| Pain interference | −.37** | −.26* | .47** | .46** | .47** | - |
|
| ||||||
| Mean | 63.48 | 2.65 | 17.27 | 19.41 | 18.69 | 37.65 |
| Standard deviation | 15.97 | 0.54 | 8.34 | 7.05 | 7.79 | 26.65 |
| Range | 17–84 | 1.70–4 | 8–40 | 7–35 | 0–37 | 0–94 |
| Cronbach’s alpha | 0.94 | 0.82 | 0.96 | 0.94 | 0.90 | 0.95 |
Note.
p <.001
p<.05.
The associations between patients’ psychological distress and other variables (pain, demographics) were explored for potential covariates. Greater pain interference and younger age were associated with greater psychological distress (ps<.05). Additionally, females reported greater psychological distress (ps<.05). Race, marital status, and income were not significantly related to psychological distress (ps>.11).
3.1. Mediation Analyses
Mediation models were constructed to test whether social support was indirectly associated with three aspects of psychological distress (anxiety, depression, stress) through mindfulness (Figure 1; see Supplemental material for alternative models). Mediation analyses were tested using 5000 bootstrapped samples with the PROCESS macro for SPSS. For each model, social support was entered as the independent variable (x variable), mindfulness as the mediator variable (m variable), and a psychological distress outcome (i.e., anxiety, depression, stress) as the dependent variable (y variable). Pain interference, age and gender were included as covariates.
Figure 1.
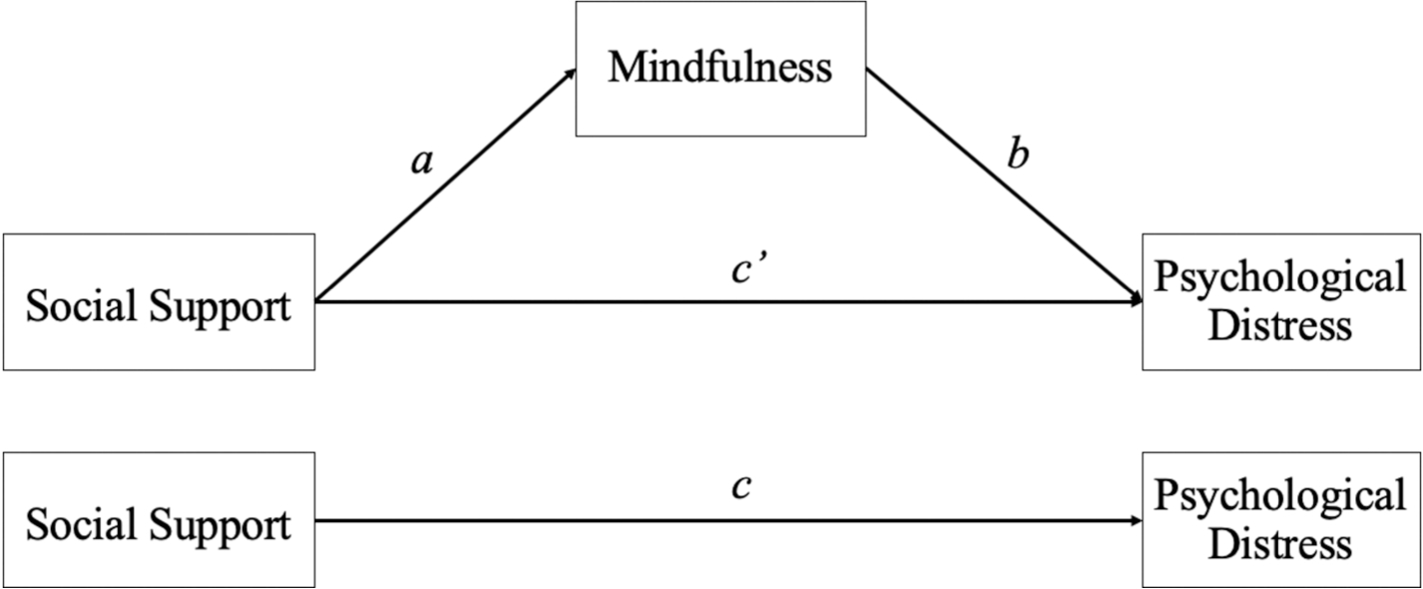
Conceptual mediation model testing mindfulness as a mediator of the association between perceived social support and psychological distress (i.e., depression, anxiety, and stress). Covariates included pain interference, age, and gender.
3.1.1. Anxiety
There was a significant indirect effect of social support on anxiety through mindfulness (b = −0.035, 95% CI [−0.08, −0.004]). The direct effect of social support on anxiety was no longer significant (b = −0.050, p=0.199) when mindfulness was included in the model.
3.1.2. Depression
There was a significant indirect effect of social support on depression through mindfulness (b = −0.029, 95% CI [−0.081, −0.003]). The direct effect of social support on depression was reduced (b = −0.146, p=.003) when mindfulness was included in the model.
3.1.3. Stress
There was a significant indirect effect of social support on stress through mindfulness (b = −0.040, 95% CI [−0.105, −0.004]). The direct effect of social support on stress was reduced (b = −0.094, p=.022) when mindfulness was included in the model.
4. Discussion
The current study examined the protective effects of social support and mindfulness against psychological distress among chronic pain patients after living through a year of the pandemic. Greater social support and greater mindfulness were associated with less distress. Further, our findings suggest that mindfulness partially mediates the relation between social support and psychological distress, even when accounting for patients’ pain interference, age, and gender.
Consistent with prior research, greater social support was associated with greater mindfulness. This finding adds to the limited research linking social support and mindfulness (described previously within healthy adults) by demonstrating this association within a different sample (chronic pain patients), and within a different context (reduced social support during social distancing). Greater mindfulness was also related to less psychological distress, consistent with previous findings in healthy adults during the pandemic (Haliwa et al., 2020). Replication of these associations between social support, mindfulness, and distress across samples and contexts demonstrates consistency and generalizability.
To our knowledge, only one other study has examined mindfulness as a mechanism through which social support can reduce psychological distress, finding that mindfulness significantly reduced the association between social support and distress (Wilson et al., 2020). The current findings replicate these findings, demonstrating that inclusion of mindfulness as a mediator weakened the association between social support and three assessments of psychological distress among individuals with chronic pain, at a time of relatively decreased access to that support.
Because chronic pain is often comorbid with psychopathology (Dersh et al., 2002), it is important to investigate ways of protecting against psychological distress. Reducing distress has shown to reduce other maladaptive pain-related cognitions and the experience of pain. Our findings extend current literature and provide potentially important clinical implications that mindfulness skills may be a promising therapeutic target to reduce distress among chronic pain. MBIs are increasingly employed as a psychological intervention for patients with pain. Group-based mindfulness interventions have shown to reduce depression in patients with chronic pain (Khoo et al., 2019). Supplementing social support with mindfulness skills may improve patients’ ability to cope with stressors, particularly in times of heightened distress and isolation.
There are limitations to consider in interpreting these findings. The observational nature precludes inference of causality, and the cross-sectional design limits temporal ordering of variables. Future experimental or longitudinal designs are necessary to test for causality and the directionality of relationships. Interestingly, we found no evidence that social support mediated the association between mindfulness and anxiety or stress (alternative model), in contrast to our previous study in healthy volunteers (Wilson et al., 2020), where a bidirectional mediating effect was observed. While we replicated findings based on healthy adult samples by using a sample of chronic pain patients, our sample was from Massachusetts and mostly White and female, which constrains the generalizability of these findings. Future studies will benefit from recruiting a more demographically and geographically diverse sample. The size of the sample was small, which raises potential concerns about Type I error. Future researchers should recruit a larger sample in hopes of replicating these findings.
Our results show that social support and mindfulness have protective effects against psychological distress in chronic pain patients. Further, mindfulness partially mediates the association between social support and distress. Our findings expand upon the limited research within this area by demonstrating these associations within a chronic pain sample, providing further empirical support for Feeney and Collins’ (2014) model of social support. Additionally, our findings suggest that integration of social support and mindfulness may be additive or synergistic in the pursuit of mental health, and future behavioral interventions may benefit from combining them.
Supplementary Material
Acknowledgments
Source of Funding: The conduct of this study was supported by a grant from the NIH/NIGMS: R35 GM128691.
Footnotes
Declarations of interest: none
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Baer RA (2003) Mindfulness training as a clinical intervention: a conceptual and empirical review. Clinical psychology: Science and practice 10(2): 125. [Google Scholar]
- Cella D, Riley W, Stone A, et al. (2010) The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005–2008. Journal of Clinical Epidemiology 63(11): 1179–1194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cleeland CS and Ryan K (1991) The brief pain inventory. Pain Research Group. 143–147. [Google Scholar]
- Cohen S, Kamarck T and Mermelstein R (1994) Perceived stress scale. Measuring stress: A guide for health and social scientists 10(2): 1–2. [Google Scholar]
- Dersh J, Polatin PB, & Gatchel RJ (2002). Chronic pain and psychopathology: Research findings and theoretical considerations. Psychosomatic Medicine, 64(5), 773–786. [DOI] [PubMed] [Google Scholar]
- Feeney B and Collins N (2014) A new look at social support: An integrative perspective on thriving through relationships. Personality and Social Psychology Review. Online First. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feldman G, Hayes A, Kumar S, et al. (2007) Mindfulness and emotion regulation: The development and initial validation of the Cognitive and Affective Mindfulness Scale-Revised (CAMS-R). Journal of psychopathology and Behavioral Assessment 29(3): 177–190. [Google Scholar]
- Haliwa I, Wilson J, Lee J, & Shook NJ (2021). Predictors of Change in Mental Health during the COVID-19 Pandemic. Journal of Affective Disorders. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harandi TF, Taghinasab MM and Nayeri TD (2017) The correlation of social support with mental health: A meta-analysis. Electronic physician 9(9): 5212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holt-Lunstad J and Smith TB (2012) Social relationships and mortality. Social and Personality Psychology Compass 6(1): 41–53. [Google Scholar]
- Hruschak V, Flowers KM, Azizoddin DR, et al. (2021) Cross-sectional study of psychosocial and pain-related variables among patients with chronic pain during a time of social distancing imposed by the coronavirus disease 2019 pandemic. Pain 162(2): 619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khoo EL, Small R, Cheng W, Hatchard T, Glynn B, Rice DB, … & Poulin PA (2019). Comparative evaluation of group-based mindfulness-based stress reduction and cognitive behavioural therapy for the treatment and management of chronic pain: A systematic review and network meta-analysis. Evidence-Based Mental Health, 22(1), 26–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klainin-Yobas P, Ramirez D, Fernandez Z, et al. (2016) examining the predicting effect of mindfulness on psychological well-being among undergraduate students: A structural equation modelling approach. Personality and Individual Differences 91: 63–68. [Google Scholar]
- Mahmud S, Mohsin M, Dewan M, & Muyeed A (2022). The global prevalence of depression, anxiety, stress, and insomnia among general population during COVID-19 pandemic: A systematic review and meta-analysis. Trends in Psychology, 1–28. [Google Scholar]
- Majeed MH, Ali AA, & Sudak DM (2018). Mindfulness-based interventions for chronic pain: Evidence and applications. Asian Journal of psychiatry, 32, 79–83. [DOI] [PubMed] [Google Scholar]
- Piraccini E, Byrne H and Taddei S (2020) Chronic pain management in COVID-19 era. Journal of Clinical Anesthesia 65: 109852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Podsakoff PM, MacKenzie SB, Lee JY, & Podsakoff NP (2003). Common method biases in behavioral research: A critical review of the literature and recommended remedies. Journal of Applied Psychology, 88, 879–903. [DOI] [PubMed] [Google Scholar]
- Serrano-Ibáñez ER, Esteve R, Ramírez-Maestre C, et al. (2021) Chronic pain in the time of COVID-19: Stress aftermath and central sensitization. British Journal of Health Psychology 26(2): 544–552. [DOI] [PubMed] [Google Scholar]
- Wilson JM, Weiss A and Shook NJ (2020) Mindfulness, self-compassion, and savoring: Factors that explain the relation between perceived social support and well-being. Personality and Individual Differences 152: 109568. [Google Scholar]
- Zimet GD, Dahlem NW, Zimet SG, et al. (1988) The multidimensional scale of perceived social support. Journal of Personality Assessment 52(1): 30–41. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.