

Abstract
Objective
To estimate the impact of Medicaid expansion on emergency department (ED) wait times.
Data sources
We used 2012–2017 hospital‐level secondary data from the CMS Hospital Compare data warehouse.
Study design
We used a state‐level difference‐in‐differences approach to identify the impact of Medicaid expansion on four measures of ED wait times: time before being seen by a provider; time before being sent home after being seen by a provider; boarding time spent in the ED waiting to be discharged to an inpatient room; and the percentage of patients who left without being seen. We compared outcomes in states that expanded Medicaid with those in states that did not expand Medicaid.
Data collection/extraction methods
Our sample included all US acute care hospitals with EDs in states that did not ever expand Medicaid or that fully expanded Medicaid in January of 2014.
Principal findings
Medicaid expansion was associated with a 3.1‐min increase (SE: 0.994, baseline mean: 30.8 min) in the time spent waiting to see an ED provider, a relative increase of 10%. Patients who were eventually sent home after being seen by a provider experienced a 7.5‐min increase (SE: 1.8, baseline mean 142.1 min) in wait time. Boarding time rose by 3.8 min (SE 1.9, baseline mean 111.4 min). The percentage of patients who left without being seen rose by 0.3 percentage points (SE: 0.09, baseline mean 2.0), a relative increase of 15.3%.
Conclusions
This study provides multistate evidence that Medicaid expansion increased ED wait times for patients, indicating that ED crowding may have worsened post‐expansion. Future work should aim to uncover the mechanisms through which insurance expansion increased ED wait times to provide policy direction.
Keywords: crowding, emergency service, Medicaid, Patient Protection and Affordable Care Act, policy
What is known on this topic
Long wait times in the ED are a sign of crowding, which poses a significant barrier to receiving timely care and is associated with undesirable health outcomes.
Medicaid expansion could affect ED input, throughput, and output factors, which in turn might have influenced wait times.
What this study adds
Medicaid expansion was associated with an increase in ED wait times.
Expansion was also associated with an increase in the percentage of patients who left the ED without being seen, which might have a harmful effect on at‐risk patients.
1. INTRODUCTION
The emergency department (ED) is a vital component of the U.S. health care system, providing treatment not only for emergencies but also for less urgent illnesses among those who have difficulty accessing care elsewhere. 1 The expanded role of the ED has led to significant crowding, which occurs when there are more patients than staffed ED treatment beds, and wait times exceed a reasonable period. 1 Crowding poses a significant barrier to receiving timely care and is associated with undesirable outcomes. 2 , 3 , 4 Of note, research has shown that as ED wait times lengthen, patients are more likely to leave without being seen (LWBS), which increases their risk for adverse events later. 5 , 6
The impact of Medicaid expansion on ED crowding was an often‐discussed topic prior to the Affordable Care Act's (ACA's) implementation, with many hoping that increased cost‐sharing for nonemergency ED visits would motivate patients to use lower‐cost care sites. 7 , 8 Crowding, however, arises due to many factors that may or may not have been affected by expansion. These can be grouped into three larger categories, per Asplin et al.'s conceptual model of ED crowding. 1 Input to the ED comprises the number and type of patients walking through the doors, which might have increased as ED services became covered for many who were previously uninsured or decreased as the newly insured gained access to primary care. 1 ED throughput contributes to crowding via a patient's length of stay or the time it takes to move through the ED. Throughput factors might have been affected by expansion if ED clinicians changed their evaluation and/or treatment practices as a response to more patients being insured. The primary way ED output contributes to crowding is through boarding, whereby patients who have been assessed in the ED and deemed appropriate for inpatient admission must wait in the ED until an inpatient bed becomes available. 1 Just as expansion might have increased the volume of ED visits, it could also have prompted more inpatient use, which in turn could worsen boarding bottlenecks in the ED.
Despite the many ways Medicaid expansion could have affected ED crowding, our study is among the first to examine this question empirically, using wait times as a proxy for crowding. We used 2012 to 2017 data from the Centers for Medicare and Medicaid Services (CMS) in an event study design to assess changes in ED wait times after Medicaid expansion. Further, we examined the impact of expansion on the number of patients who LWBS, because this outcome has direct impacts on health care outcomes and costs.
2. METHODS
The data for this study come from the CMS Hospital Compare website, a resource created to increase transparency in hospitals' care provision. 9 Hospitals are required to report quality metrics in exchange for receiving the full update to their CMS payment rate; the data are then assembled into a public‐facing website. The data are collected for all hospital patients, not just those insured by Medicare or Medicaid. This website allows consumers to select multiple hospitals and directly compare performance measures covering various dimensions. To ensure data accuracy, CMS annually selects up to 500 hospitals (450 randomly selected hospitals and up to 50 targeted hospitals) for a data audit and validation. 10
Our study used the ED wait time measures in the Hospital Compare database. Each wait time data point comes from a sample of patients in a given ED who sought services in the prior consecutive four quarters. Our sample included all US acute care hospitals with EDs in states that (a) did not ever expand Medicaid or (b) fully expanded Medicaid in January 2014. Information on the timing of states' decisions to expand Medicaid came from the Kaiser Family Foundation. 11 We excluded states (CA, CT, MN, NJ, WA) that expanded Medicaid substantially prior to January 2014 and were, therefore, not fully “treated” by the ACA expansion, as well as states (AK, IN, LA, MT, NH, PA) that expanded Medicaid at later dates. To avoid selection concerns due to hospitals potentially dropping in or out of the sample, we limited our analysis to hospitals that provided data throughout the entire study period. We excluded Critical Access Hospitals from our analysis because their participation in the reporting program is voluntary and their data are, therefore, at risk for selection bias. Our study period ranged from 2012 to 2017, which provided us with 6 rolling quarters of data before the 2014 Medicaid expansion and 13 quarters afterward. In the data, there were measurement periods (e.g., January 4, 2013 to January 4, 2015) that overlap with the time of expansion itself (January 1, 2014); we excluded these periods from our sample. Our final sample consisted of a panel of 2247 US acute care hospitals.
We used a state‐level difference‐in‐differences approach to identify the impact of ACA Medicaid expansion on ED wait times. We compared outcomes among hospitals in states that expanded Medicaid with those in states that did not expand Medicaid before and after the expansion occurred. We used the following model:
where y h,s,t is a wait time outcome for hospital h in state s in rolling quarter (or for one measure, year) t; is a binary variable that takes a value of 1 in the time period after expansion; is a binary variable that takes the value of 1 if a state is in our treatment group (i.e., expanded Medicaid); is a vector of hospital fixed effects to capture the effect of time‐invariant hospital characteristics; is a vector of period fixed effects to control for time‐varying shocks to all hospitals; and is an idiosyncratic error term.
Our key independent variable was the interaction term between and , which estimated the causal impact of expansion on wait times under the assumption that in the absence of expansion, the difference in wait times between treated and control states would have been constant over time. While there is no statistical test for this assumption, the event studies we conducted suggested that the treatment and control groups followed parallel trends prior to expansion. Standard errors were clustered at the state level, where policy variation occurs. Regression models were weighted by the number of patients for whom survey responses were collected.
Our first three outcomes measured wait times at different points throughout a patient's length of stay in the ED. The first outcome is the median number of minutes patients waited to see a provider upon arrival at the ED. The second outcome is the median time from ED arrival to ED departure for discharged patients. This measure excludes patients who were later admitted to the hospital as inpatients, admitted for observation, transferred to another acute care hospital, or left without being seen by a licensed provider. The third outcome captured boarding time, or the median time patients spent in the ED after a clinician decided to admit them as an inpatient but before leaving the ED for their inpatient room.
Our last outcome was the percentage of LWBS patients: those who signed in for emergency services but left the ED without being evaluated by a provider. We included this measure because it could indicate whether wait time changes impact patient decisions to pursue care. This outcome differed from the prior ones in two key ways: it measured a percentage of patients rather than a number of minutes; and it is reported by hospitals yearly rather than quarterly. We therefore had fewer data points to use in our analysis, and our results for this measure must be interpreted with appropriate caution.
One limitation of our analysis is that we could not determine whether wait times changed similarly across patients of different acuity levels because we did not have access to any patient‐level micro data. This is of interest because while rising wait times among less emergent cases may be inconvenient and increase patient discomfort, they are unlikely to have severe health consequences. They might signal a need for expanding primary care access rather than increasing ED capacity for these visits. If wait times are increasing among patients who are critically ill, such as those experiencing trauma or heart attack, the consequences could be deadly. Though the Hospital Compare data provide some measures of ED care for emergent cases (e.g., the number of minutes before patients with possible heart attack received treatment), much of these data (up to 97%) are missing, precluding their use in this analysis.
3. RESULTS
Summary statistics for the ED sample are provided in Table 1. Across the entire sample period, EDs in expansion states tended to have higher annual patient volumes than those in non‐expansion states and were more likely to be privately owned compared to non‐expansion states. In terms of care timeliness, hospitals in expansion states were more likely to be above (i.e., be more timely than) the national average (16.9%) compared with those in non‐expansion states (7.7%, p < 0.01). Hospitals in non‐expansion states, however, were more likely (35%) to be above the national average in terms of mortality (i.e., have lower mortality rates) than those in expansion states (26.8%, p < 0.01).
TABLE 1.
Characteristics of hospital emergency departments by expansion status
| Expansion states | Non‐expansion states | |
|---|---|---|
| Annual ED volume | ||
| Low (19,999 patients or fewer) | 21.4% | 34.0%*** |
| Medium (20,000–39,999 patients) | 35.1% | 28.9%*** |
| High (40,000–59,999 patients) | 21.6% | 16.8%*** |
| Very high (60,000 patients or more) | 21.9% | 20.4%* |
| Ownership status | ||
| Public | 9.6% | 22.9%*** |
| Private | 11.8% | 30.9%*** |
| Voluntary | 78.5% | 46.1%*** |
| Timeliness of care national comparison | ||
| Below the national average | 10.5% | 13.0%*** |
| The same as the national average | 66.9% | 69.4%** |
| Above the national average | 16.9% | 7.7%*** |
| Mortality national comparison | ||
| Below the national average | 29.9% | 22.1%*** |
| The same as the national average | 40.2% | 40.4% |
| Above the national average | 26.8% | 35.0%*** |
| Wait time outcomes at baseline | ||
| Number of minutes before being seen by a provider | 29.9 | 31.3* |
| Number of minutes patients waited before being sent home by a provider | 144.1 | 140.8* |
| Number of minutes patients waited after being admitted as inpatient but before leaving ED for inpatient room | 121.0 | 103.2*** |
| Percent of patients who left without being seen by a provider | 1.8 | 2.1*** |
| Observations (number of hospitals) | 991 | 1255 |
Note: Table displays means and statistical significance of differences in hospital characteristics in expansion versus non‐expansion states. Sample excludes early/late expansion states (CA, CT, MN, NJ, WA, NH, PA, IN, AK, MT, LA). Sample includes acute care hospitals with an emergency department. Timeliness of care and mortality national comparisons were calculated in 2014 as the time it was first released by CMS.
Source: Authors' analysis of Hospital Compare data 2012–2017.
p < 0.10; **p < 0.05; ***p < 0.01.
In Figure 1, we present our results in the form of event studies. We first note that these figures provide evidence that the parallel trends assumption holds for our difference‐in‐differences models. We found that prior to Medicaid expansion, there were no statistically significant differences in our outcomes across expansion and non‐expansion states. After expansion took place, however, we found sustained differences in median wait time before patients were seen by a provider (Panel A) and the total time patients spent in the ED before being sent home (Panel B). We found an increase in median boarding time (Panel C) that occurs just after expansion, although this effect is not sustained over time. The percent of ED patients who LWBS by a provider (Panel D) appeared to increase post‐expansion, although we reiterate that this measure is collected annually rather than quarterly and should thus be regarded with appropriate caution.
FIGURE 1.
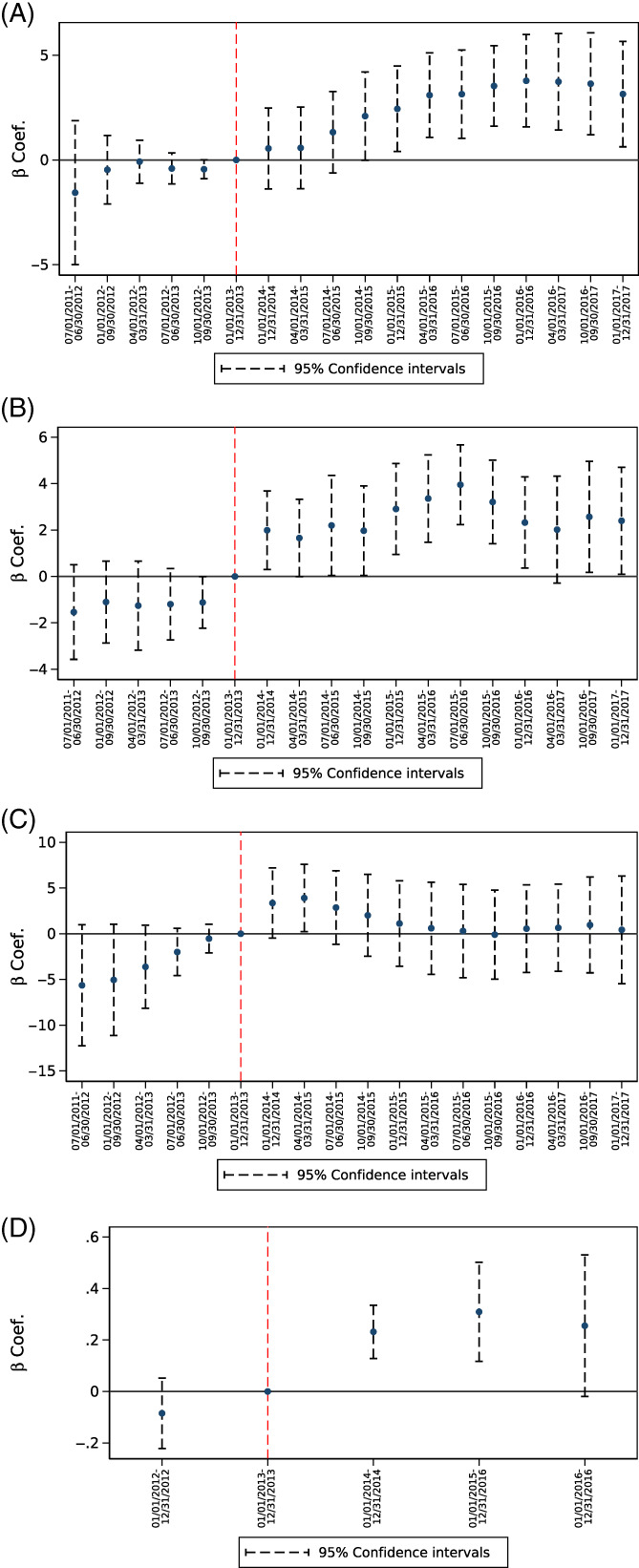
Event study analysis of impact of Medicaid expansion on emergency department wait times and percentage of patients who leave without being seen (LWBS). (A) # of minutes before being seen by a provider. (B) # of minutes patients spent in ED before being sent home. (C) # of minutes after being admitted as inpatient before leaving ED for inpatient room. (D) Percent of patients who left without being seen by a provider. Figure displays the coefficients of expansion × period interactions and their confidence intervals. Sample excludes early/late expansion states (CA, CT, MN, NJ, WA, NH, PA, IN, AK, MT, LA). Sample includes acute care hospitals with an emergency department. Models include period and state fixed effects. All regressions are unweighted. Exactly 95% confidence intervals are obtained from state‐clustered heteroscedasticity‐robust standard errors. Source: Authors' analysis of Hospital Compare data 2012‐2017 [Color figure can be viewed at wileyonlinelibrary.com]
The regression results from our main analysis are displayed in Table 2. Among all ED patients who eventually saw a provider, Medicaid expansion increased the median wait time before being seen by 3.0 min (p < 0.01), a relative increase of 10.0% over the pre‐ACA baseline of approximately 31 min. Turning next to patients who were eventually sent home after being seen by a provider, we find a 7.5‐min (p < 0.01) increase over a baseline of 142 min. This represents a 5.3% increase in median wait time. Boarding time increased by 3.8 min (p < 0.05), or 3.4%, over a baseline of 111 min. The last coefficient represents the change in the percentage of patients who left the ED without being seen. This measure increased by 0.31 percentage points (p < 0.01), a relative increase of 15.3% after expansion.
TABLE 2.
Impact of Medicaid expansion on emergency department wait times and percent of ED patients who left without being seen
| Coef. (SE) | Baseline mean | Change from baseline | |
|---|---|---|---|
| Number of minutes before being seen by a provider (N = 39,296) | 3.8*** (0.994) | 30.8 | 10.0% |
| Number of minutes patients waited before being sent home by a provider (N = 39,359) | 7.5*** (1.760) | 142.1 | 5.3% |
| Number of minutes patients waited after being admitted as inpatient, but before leaving ED for inpatient room (N = 39,161) | 3.8** (1.871) | 111.4 | 3.4% |
| Percent of patients who left without being seen by a provider (N = 11,251) | 0.3*** (0.088) | 2.0 | 15.3% |
Note: Baseline mean is calculated in Q4/2012–Q4/2013 and weighted by number of patients for which outcomes were recorded. Number of observations reflects numbers of hospitals reporting a measure multiplied by number of periods reported. All regressions are weighted by number of patients for which wait times are recorded. Sample excludes early/late expansion states (CA, CT, MN, NJ, WA, NH, PA, IN, AK, MT, LA). Sample includes acute care hospitals with an emergency department. Models include period and hospital fixed effects. Standard errors, heteroscedasticity‐robust and clustered by state, are in parentheses.
Source: Authors' analysis of Hospital Compare data 2012–2017.
p < 0.10; **p < 0.05; ***p < 0.01.
4. DISCUSSION
This study estimated the impact of Medicaid expansion on median wait times in a national sample of EDs. We found that expanding Medicaid increased the time patients waited to see an ED clinician by 10%. Our results can be placed in the context of several streams of literature to which they add new insight.
One possible explanation for our finding is that ED input (i.e., patient volume) increased without analogous improvements in throughput (i.e., supply‐side factors in the ED). Although it was hoped that the ACA might reduce ED volume as more patients connected with primary care outside the hospital, various empirical studies have not yet reached consensus on the extent to which this occurred. Although some have shown lower ED use post‐expansion, others have determined that ED volume did not fall and perhaps even increased as a result of expansion. 8 , 12 , 13 , 14 , 15 , 16 Although expansion did improve primary care appointment availability among Medicaid enrollees, the benefit was offset by slight increases in wait times for primary care appointments, which in turn might have limited expansion's ability to reduce ED use. 17
In addition to volume changes, selection effects among newly Medicaid‐eligible people (with sicker patients more likely to receive Medicaid) could also be responsible for rising ED wait times if higher‐acuity patients visit the ED post‐expansion. Studies on this question show mixed results, perhaps due to the heterogeneous effects of the expansion across states due to state‐level decision making. 18
Changes in throughput (i.e., supply responses within the ED) related to the expansion are under‐examined in the literature, although one study has demonstrated that the number of ED procedures per visit increased approximately 4% post‐expansion. The authors of that study posit that ED providers might be sensitive to insurance status and accordingly increase treatment intensity when budget constraints slacken. 19 Future research should examine additional supply‐side responses to Medicaid expansion in the ED, such as changes to staffing models, triage protocols, and clinical decision making.
Boarding is frequently acknowledged as a primary reason for ED crowding. We found a short‐term increase in boarding time immediately after expansion, which might have had a cascading effect on resource availability in the initial stages of ED workflow and which may explain some of the increase in our other outcomes. This is in line with prior work showing that greater boarding burden is associated with increased ED lobby crowding as well as a longer length of stay for patients discharged from the ED. 20 , 21
We found that longer boarding times eventually dissipated in contrast to our other wait time outcomes. A growing body of literature has shown that while Medicaid expansion shifted the inpatient payer mix toward Medicaid, it did not impact overall hospitalization volume, or patient acuity levels generally or among those admitted from the ED. 22 , 23 , 24 In the same way Medicaid expansion might have changed provider behavior (i.e., treatment intensity) in the ED, a change in payer distribution could have changed practice among those providing care for inpatients, possibly leading to bottlenecks at the point of inpatient admission. Future work should test this theory as well as explore reasons that the change was not sustained over time.
Regardless of the mechanism through which wait times increased post‐ACA Medicaid expansion, this finding has important implications for patients and policy makers. Using annual data, we found that expansion increased the percentage of ED patients who LWBS by a provider. Prior work has shown that the most common reason for leaving the ED without being seen is impatience with long wait times. 5 , 25 Notably, a small but significant proportion of patients who LWBS do experience adverse events or have persistent problems that can jeopardize their health. 5 , 6 Further, those who are least likely to receive care elsewhere (i.e., those who are uninsured or Medicaid enrollees) are more likely to LWBS. 6 Although reducing wait times is a clear policy target to reduce the LWBS rate, improving communication about wait times while patients are in the ED lobby might help in the meantime. 5
In this study, we found evidence that the ACA's Medicaid expansion increased median wait times in a national sample of EDs and increased the percentage of patients who left the ED without being seen by a provider. This suggests that the expansion might have worsened crowding, although isolating the mechanisms contributing to this effect requires further study.
ACKNOWLEDGMENT
The authors gratefully acknowledge support from Northwestern University and West Virginia University (Dr. Allen), and Indiana University (Dr. Simon and Mr. Gian).
Allen L, Gian CT, Simon K. The impact of Medicaid expansion on emergency department wait times. Health Serv Res. 2022;57(2):294-299. doi: 10.1111/1475-6773.13892
REFERENCES
- 1. Asplin BR, Magid DJ, Rhodes KV, Solberg LI, Lurie N, Camargo CA Jr. A conceptual model of emergency department crowding. Ann Emerg Med. 2003;42(2):173‐180. [DOI] [PubMed] [Google Scholar]
- 2. Sun BC, Hsia RY, Weiss RE, et al. Effect of emergency department crowding on outcomes of admitted patients. Ann Emerg Med. 2013;61(6):605‐611.e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Carter EJ, Pouch SM, Larson EL. The relationship between emergency department crowding and patient outcomes: a systematic review. J Nurs Scholarsh. 2014;46(2):106‐115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bernstein SL, Aronsky D, Duseja R, et al. The effect of emergency department crowding on clinically oriented outcomes. Acad Emerg Med. 2009;16(1):1‐10. [DOI] [PubMed] [Google Scholar]
- 5. Rowe BH, Channan P, Bullard M, et al. Characteristics of patients who leave emergency departments without being seen. Acad Emerg Med. 2006;13(8):848‐852. [DOI] [PubMed] [Google Scholar]
- 6. Ding R, McCarthy ML, Li G, Kirsch TD, Jung JJ, Kelen GD. Patients who leave without being seen: their characteristics and history of emergency department use. Ann Emerg Med. 2006;48(6):686‐693. [DOI] [PubMed] [Google Scholar]
- 7. Friedman AB, Saloner B, Hsia RY. No place to call home—policies to reduce ED use in medicaid. N Engl J Med. 2015;372(25):2382‐2385. [DOI] [PubMed] [Google Scholar]
- 8. Friedman A. The uncertain economics of insurance enabling more emergency department visits. Ann Emerg Med. 2017;70(2):226‐228. [DOI] [PubMed] [Google Scholar]
- 9. Centers for Medicare & Medicaid Services . Official Hospital Compare data. 2013. https://data.medicare.gov/data/hospital-compare/Timely%20%26%20Effective%20Care
- 10. Centers for Medicare and Medicaid Services . Data validation overview. 2020. https://qualitynet.cms.gov/outpatient/data‐management/data‐validation. Accessed July, 2021.
- 11. Kaiser Family Foundation . Status of State Action on the Medicaid Expansion Decision. https://www.kff.org/health‐reform/state‐indicator/state‐activity‐around‐expanding‐medicaid‐under‐the‐affordable‐care‐act/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D. Accessed January, 2019.
- 12. Nikpay S, Freedman S, Levy H, Buchmueller T. Effect of the Affordable Care Act Medicaid expansion on emergency department visits: evidence from state‐level emergency department databases. Ann Emerg Med. 2017;70(2):215‐225.e6. [DOI] [PubMed] [Google Scholar]
- 13. Pines JM, Zocchi M, Moghtaderi A, et al. Medicaid expansion in 2014 did not increase emergency department use but did change insurance payer mix. Health Aff (Project Hope). 2016;35(8):1480‐1486. [DOI] [PubMed] [Google Scholar]
- 14. Sommers BD, Maylone B, Blendon RJ, Orav EJ, Epstein AM. Three‐year impacts of the Affordable Care Act: improved medical care and health among low‐income adults. Health Aff. 2017;36(6):1119‐1128. [DOI] [PubMed] [Google Scholar]
- 15. Wherry LR, Miller S. Early coverage, access, utilization, and health effects associated with the Affordable Care Act Medicaid expansions: a quasi‐experimental study. Ann Intern Med. 2016;164(12):795‐803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Dresden SM, Powell ES, Kang R, McHugh M, Cooper AJ, Feinglass J. Increased emergency department use in Illinois after implementation of the Patient Protection and Affordable Care Act. Ann Emerg Med. 2017;69(2):172‐180. [DOI] [PubMed] [Google Scholar]
- 17. Polsky D, Candon M, Saloner B, et al. Changes in primary care access between 2012 and 2016 for new patients with Medicaid and private coverage. JAMA Intern Med. 2017;177(4):588‐590. [DOI] [PubMed] [Google Scholar]
- 18. Garthwaite C, Graves JA, Gross T, Karaca Z, Marone VR, Notowidigdo MJ. All Medicaid Expansions Are Not Created Equal: The Geography and Targeting of the Affordable Care Act. National Bureau of Economic Research; 2019. [Google Scholar]
- 19. Danagoulian S, Janke A & Levy P Medicaid expansion after the ACA: intensity of treatment and billing in emergency departments. Available at SSRN 3261600; 2018.
- 20. Smalley CM, Simon EL, Meldon SW, et al. The impact of hospital boarding on the emergency department waiting room. J Am Coll Emerg Physicians Open. 2020;1(5):1052‐1059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. White BA, Biddinger PD, Chang Y, Grabowski B, Carignan S, Brown DF. Boarding inpatients in the emergency department increases discharged patient length of stay. J Emerg Med. 2013;44(1):230‐235. [DOI] [PubMed] [Google Scholar]
- 22. Pickens G, Karaca Z, Cutler E, et al. Changes in hospital inpatient utilization following health care reform. Health Serv Res. 2018;53(4):2446‐2469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Admon AJ, Valley TS, Ayanian JZ, Iwashyna TJ, Cooke CR, Tipirneni R. Trends in hospital utilization after medicaid expansion. Med Care. 2019;57(4):312‐317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Freedman S, Nikpay S, Carroll A, Simon K. Changes in inpatient payer‐mix and hospitalizations following Medicaid expansion: evidence from all‐capture hospital discharge data. PLoS One. 2017;12(9):e0183616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Fraser J, Atkinson P, Gedmintas A, Howlett M, McCloskey R, French J. A comparative study of patient characteristics, opinions, and outcomes, for patients who leave the emergency department before medical assessment. CJEM. 2017;19(5):347‐354. [DOI] [PubMed] [Google Scholar]