

Abstract
Introduction:
Mesenchymal stromal cells (MSCs; AKA mesenchymal stem cells) stimulate healing and reduce inflammation. Promising therapeutic responses are seen in many late-phase clinical trials, but others have not satisfied their primary endpoints, making translation of MSCs into clinical practice difficult. These inconsistencies may be related to the route of MSC delivery, lack of product optimization, or varying background therapies received in clinical trials over time.
Areas covered:
Here we discuss the different routes of MSC delivery, highlighting the proposed mechanism(s) of therapeutic action as well as potential safety concerns. PubMed search criteria used: MSC plus: local administration; routes of administration; delivery methods; mechanism of action; therapy in different diseases.
Expert Opinion:
Direct injection of MSCs using a controlled local delivery approach appears to have benefits in certain disease states, but further studies are required to make definitive conclusions regarding the superiority of one delivery method over another.
Keywords: Local Injection, Mechanism of Action, Mesenchymal Stem Cells, MSCs
1. Introduction
MSCs are multipotent stromal/stem cells widely distributed in the body. They are a heterogeneous population that was first discovered in the bone marrow (BM-MSCs)1, but later, they were obtained from various adult tissues, such as adipose tissues (AD-MSCs)2, placenta (p-MSCs)3, dental pulp (DP-MSCs)4 and umbilical cord (Wharton’s Jelly-MSC) or amniotic fluid5. They are characterized by their ability to differentiate into three distinct lineages: osteoblasts, chondrocytes, and adipocytes; their expression of a specific set of cluster of differentiation (CD) markers: e.g., CD73, CD105, and CD90; the absence of other such markers, e.g., CD34, and their ability to adhere to plastic and form colony-forming unit fibroblasts (CFU-Fs) when maintained under standard culture conditions6. Attachment to plastic is an important characteristic of MSCs and facilitates their isolation. MSCs are not a homogenous population and the tissue source, such as adipose tissue, bone marrow or umbilical cord, introduces (subtle) differences in gene expression7 which may predispose these cells to having tissue specific therapeutic properties7. Additional factors that affect therapeutic potency include donor-related variation such as the health status (morbidities), genetics, sex, and age8, cell population, and timing of MSC administration. Furthermore, the route of delivery appears to affect therapeutic efficacy, particularly with respect to heart disease9. Therefore, as treatment with MSCs becomes more widely studied and potentially clinically available, the route of administration and the mechanism of action must be considered and optimized.
2. Routes of administration
The choice of delivery route appears to be one of the most critical factors influencing the distribution, retention, survival, and efficacy of cell therapy. A gold standard has not been established and further study is needed. For current cell therapies, routes include local administration directly into tissues and organs, and systemic delivery via intra-arterial, intravenous (IV), and intraperitoneal (IP) injection, although there is very limited data regarding this last route. These methods can be roughly classified into two groups: systemic delivery and local delivery (Figure 1, illustrates the systemic and local routes of MSC administration into the heart).
Figure 1. Systemic (Sys) and local (Loc) routes of MSC administration into the heart.
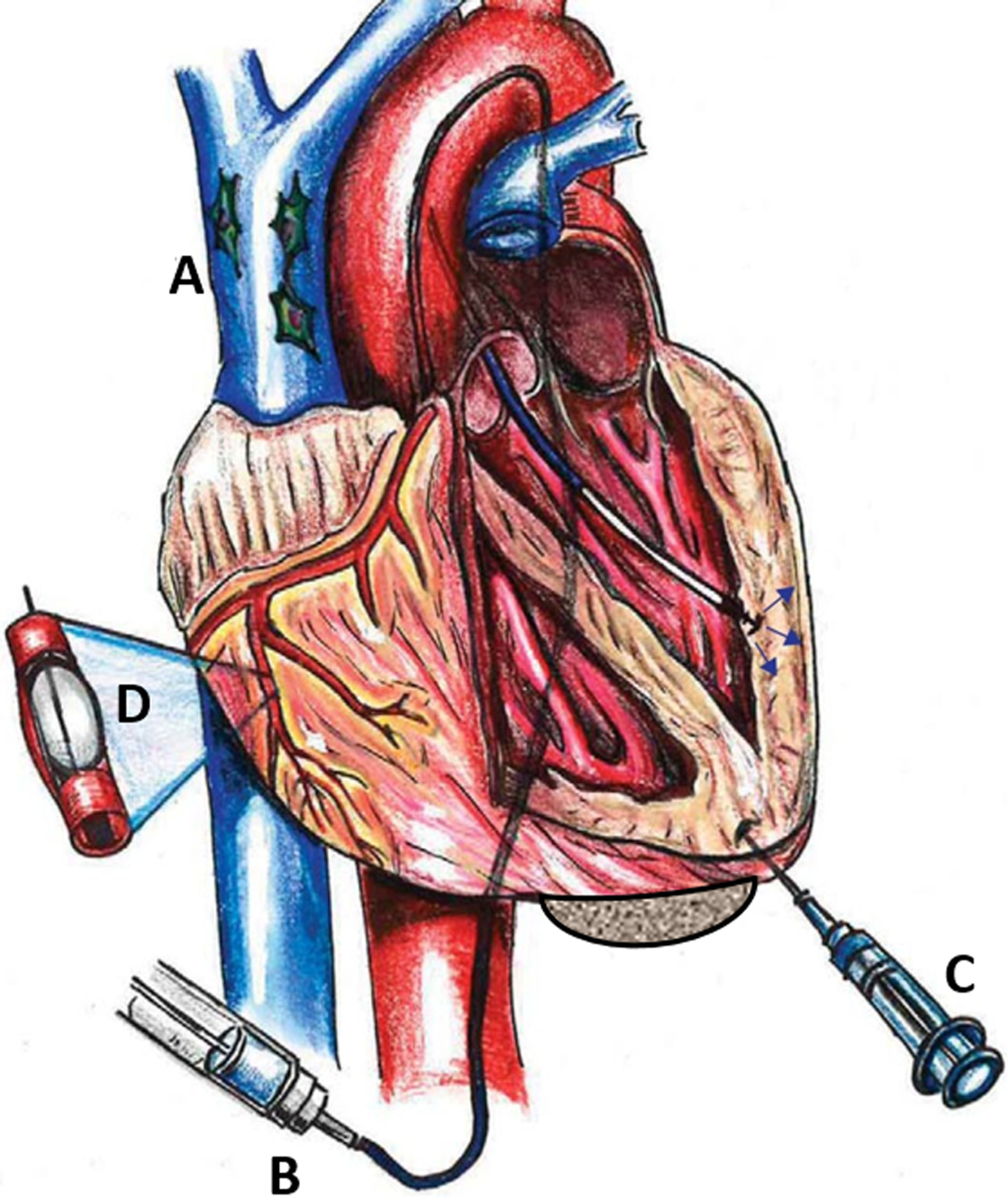
(A) intravenous (IV) infusion of mesenchymal stem cells (MSCs; peripheral IV not shown) (Sys). (B) administration of MSCs through transendocardial injection (TESI) (Loc). (C) direct epicardial injection of MSCs (Loc). (D) delivery of MSCs via intracoronary infusion (Sys). Reproduced with permission from Golpanian et al74.
Systemic delivery is a well-documented10 and minimally invasive approach. Upon intravenous delivery, cells travel through the systemic circulation reaching target sites (e.g., infarcted myocardium, inflamed joint), where they receive local signals from injured, inflamed tissue11, or cancerous tissues. This ‘homing capacity’, suggests that MSCs could serve as a cellular drug delivery system for multiple applications12. Luger and colleagues13 demonstrated that despite low myocardial engraftment, IV-administered MSCs improved cardiac function in both acute myocardial infarction and ischemic cardiomyopathy, outcomes modulated in part by systemic anti-inflammatory effects. Another advantage of IV administration is that cells are delivered into a nutrient- and oxygen-rich environment and following extravasation, MSCs remain in close proximity to the vasculature14. Despite the benefits and feasibility of systemic IV delivery, such as donor cell accumulation at the site of damage, there is a potential for cells to be trapped within the liver, lungs, and/or spleen15. The adherent nature of MSCs favors formation of a cell mass when injected via the tail vein in pre-clinical studies16, which could explain why cells applied intravenously have a higher risk of capture within capillary-like lung tissue17. Cells with diameters up to 20–50 μm, remain within the systemic vasculature, where there is a risk producing vascular occlusion18, particularly considering that systemic administration often requires that the cells be diluted, and multiple cell infusions performed. IV administration of 0.5×106 cells/kg body weight was sufficient to cause a myocardial infarction (MI) in mice, even in a previously healthy vasculature19, an important consideration since patients with end-stage HF may require a higher dose of cells and longer repair time, which may further induce a severe systemic immune response20. Therefore, IV administration is a better suited approach for early-stage heart injury20.
Intra-arterial (IA) delivery may prove the most efficacious method in some treatment indications. IA delivery of MSCs allows for infusion of cells within the local vascular system of the target organ resulting in more cells reaching the target tissue without the physical risks of direct implantation and the pitfalls of IV administration, in particular the trapping of cells within the lung microvasculature21. However, IA delivery of MSCs into the cerebral microvasculature as a treatment for stroke, may prove harmful, since it entails the potential risk of cerebral infarcts, caused by emboli of cells22 (reviewed in23). Factors such as vascular access, cell size, cell dosage and delivery speed must be considered, especially when delivering cells into coronary or cerebral arteries24, 25. IA cell delivery has also been utilized in other pathologies including, but not limited to, intra-carotid delivery in stroke, intra-renal delivery for renovascular disease, and intra-hepatic delivery for cirrhosis26, 27.
There are beneficial effects for intraperitoneal (IP) injection of MSCs, although the fate, benefits and limitations of this method have not been well investigated28, 29. IP injection produces a slower rate of cell migration from the peritoneal cavity, which could avoid the potentially lethal rapid embolization of the lung vasculature30, allowing for the administration of more cells. IP injected MSC have comparable or even more profound effects in preclinical models of multiple diseases31 compared to IV administration. The beneficial effects of MSCs in these and other disease models are linked to their ability to modify both the innate and acquired immune systems. Bazhanov et al. 2016 showed that IP injected hMSCs rapidly formed aggregates with mouse macrophages and B220+ lymphocytes and these aggregates attach to the mesentery, omentum, and other sites in the peritoneal cavity. In contrast, only small numbers of cells migrate into the systemic circulation28 from where they can engraft into multiple distal organs.
Local administration of MSCs into target tissues or into the vicinity of the injury site has important advantages, including rapid and localized reaction32. Cells can be administered into a precise, targeted location, increasing the chance of engraftment (associated with tissue regeneration)33 and prolonging their therapeutic potential (direct paracrine support)34. Local injection to the injury site in conjunction with biomaterials/scaffolds may decrease the risk of lung or cardiac infarction17. Cells migrating from a scaffold tend to migrate individually, making them less likely to aggregate in the lung17. However, local administration also involves risks, such as cells inducing apoptosis when administered at high density35. A “washout” effect is highlighted in many local cell delivery routes, in particular, intramyocardial injection11, 36. During invasive surgery, needles or catheters can cause mechanical damage to cardiac tissue, opening blood vessels and leaving needle tracks in the myocardium creating a space through which cells in suspension can travel11. Additional properties for local administration are discussed in detail below.
3. Mechanisms of action after local delivery
Due to the significant clinical relevance of the application of MSCs for treating tissue damage, there is an urgent need to better characterize the mechanism of action of MSCs after local injection. Several possible mechanisms by which MSCs exert their beneficial effects have been proposed. Despite early evidence of direct differentiation of MSCs and cell replacement, recent studies strongly suggest that their most significant mechanisms of action can be attributed to their ability to, secrete paracrine factors37 including extracellular vesicles (EVs)38 and cytokines39, transfer mitochondria to nearby cells40 (Figure 2), migrate41 and modify the immune response (immunomodulation)42.
Figure 2. MSCs’ mechanism of action.
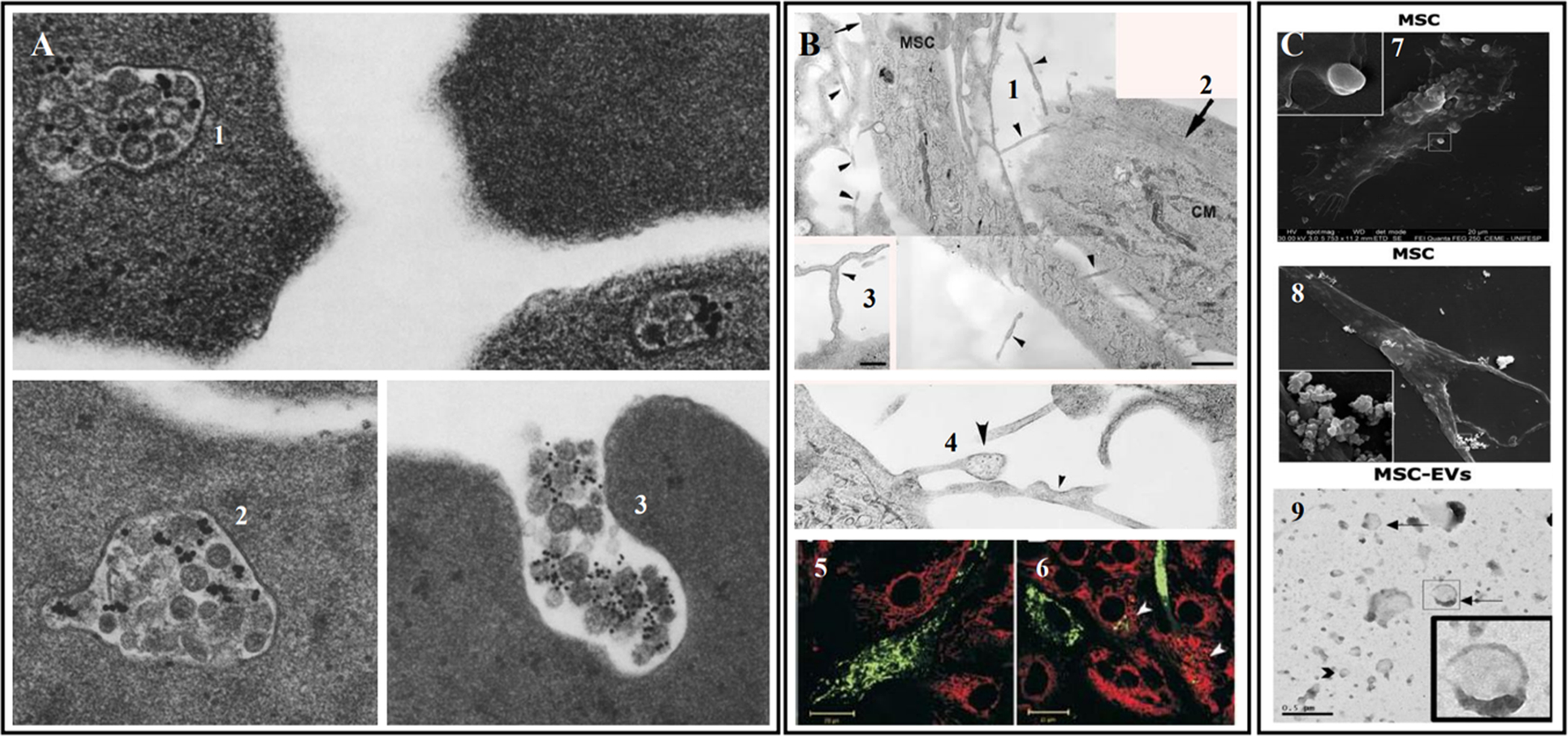
(A) Intracellular localization of multivesicular elements and their fusion with the plasma membrane in a sheep reticulocyte. 1. & 2. Inside these MVEs, which have a diameter of 200–400 nm, are small round bodies with an average diameter of 30–50 nm. 3. Fusion of multivesicular elements with the plasma membrane and release of round bodies. The figure shows exocytosis into the medium of small dense bodies (exosomes)164. (B) Electron microscopy of intercellular tunneling nanotubes (shown by black arrowheads) and mitochondria transfer from MSC to cardiomyocytes analyzed in fluorescence microscopy. 1. & 2. Two communicating cells, mesenchymal stem cell (MSC) and cardiomyocyte (CM); big arrow points to muscle fiber bundles; small arrow points to a funnel-shaped initiation/termination of the nanotube. 3. Small diameter branching nanotubes (arrowhead). 4. One nanotube with variable diameter and another with granular content are shown by big and small arrowheads correspondingly. Bar, 1 μm for A; 0.5 μm. 5. In majority of cells, mono-colored fluorescing mitochondria are dominating. 6. In some cardiomyocytes (arrowheads), green-fluorescent mitochondria derived from MSCs are present. MSCs are stained with Mitotracker Green FM (green fluorescence), while cardiomyocytes with Mitotracker Red (red fluorescence)165. (C) The release of vesicles of different sizes is demonstrated. In 7. a larger vesicle is budding from the cell membrane, while in 8. a pool of smaller vesicles is released. 9. MSC-EVs are visualized by transmission electron microscopy, showing the characteristic double membrane structure. Arrows indicate larger vesicles, compatible with microvesicles, whereas arrow heads indicate smaller vesicles, compatible with exosomes166.
3.1. Paracrine factors
MSCs release a plethora of biologically active factors (e.g., cytokines, chemokines, hormones, growth factors, and miRNAs), which have profound effects on local cellular dynamics. This multitude of paracrine factors forms part of a complex network that serves to protect injured tissue and encourage endogenous repair/regenerative mechanisms37 and immune-mediated phagocytosis43, which can lead to long-term beneficial effects.
The secretome is the repertoire of factors secreted by MSCs and can impact the activities of other cells in the local microenvironment. Up to 80% of the therapeutic effect of adult MSCs may occur through such paracrine-mediated actions, and proteins secreted by MSCs have been documented to be antimicrobial, antifibrotic, and pro-regenerative, exerting effects on processes such as angiogenesis, proliferation, differentiation, immune modulation, wound healing, bone regeneration, and kidney and cardiac repair44. While MSCs from different sources share a substantial degree of similarity, there are variations in marker expression profile and secretomes45. In vitro, AT-MSCs secrete higher amounts of angiogenic and anti-apoptotic growth factors, such as hepatocyte growth factor (HGF) and VEGF, as well as IL-6, whereas BM-MSCs secrete higher amounts of the cell migration-related chemokine, stromal cell-derived factor (SDF)-1α46. Wharton’s jelly-MSCs secrete higher levels of immune-signaling molecules and neurotrophic factors, such as brain-derived neurotrophic factor (BDNF), compared to BM-MSCs, suggesting a greater beneficial role for Wharton jelly-MSCs in neurodegenerative diseases47.
These secreted, biologically active molecules, including nucleic acids, proteins and lipids, are (primarily) transported to their targets within MSC-derived EVs (≤1000 nm in diameter) and exosomes (EVs ≤200 nm in diameter), and can retain the biological activity of the parental MSCs, producing similar therapeutic effects across different animals models48. The exchange of EVs, macromolecular complexes and exosomes with target cells49 releases a wide range of functional proteins, mRNAs, and microRNAs (miRNAs) capable of protecting the target tissue from ischemic injury by promoting neovascularization, cell proliferation and preventing apoptosis50. Moreover, EVs can mediate the transfer of mitochondrial and non-mitochondrial cargos, contributing to improved intracellular energetics51. Ongoing studies are examining the efficacy of MSC-derived exosomes and EVs as novel “cell-free” approaches to recapitulate MSC activity without the need to administer cells, an approach that obviates the unique challenges and considerations associated with cell administration52. One of the potential offshoots of research in cell-based therapy is the development of drug-free or surgical-free options recapitulating the secretome; this is under development in many indications, including chronic pain and severe injuries53. Gupta et al. described a cell-free stem cell-derived extract (CCM) formulation containing GFs, CKs, and EVs, including a high density of exosomes54, that appears effective for enhancing the rate of cell proliferation and inducing stem cell migration54.
Local, rather than systemic, transplantation of MSCs is associated with greater paracrine potency in the production of trophic factors55. These paracrine signals are generally transmitted over only short distances, thereby producing local effects56 and the crosstalk between the local microenvironment of injured host tissues and MSCs activates MSC production of cytoprotective paracrine factors. Therefore, the proximity of donor cells to the injury site is essential for paracrine-protective effects57. However, MSCs can also elicit responses at a distance using a paracrine mechanism.
In preclinical and clinical trials, local injection of MSCs into the border zone of the heart (between infarcted and viable cardiac tissue) results in a powerful anti-fibrotic effect, reduces tissue injury, and augments viable and perfused tissue49, 58. The improvement in contractile cardiac muscle results predominantly from enhanced endogenous regenerative mechanisms. Since relatively few MSCs engraft at the site of injury relative to the degree of functional recovery, a paracrine mechanism appears to be the primary driver of this therapeutic effect. Additionally, endogenous precursor cells and myocyte mitosis is upregulated following MSC treatment59. Cell therapy may activate endogenous cardiac repair mechanisms by inactivation of both the retinoblastoma and CDKN2a pathways60.
Mechanistically, MSC-derived EVs are enriched for transcriptionally active-signal transducer and activator of transcription (STAT) 3, which, among other effects, controls, angiogenesis by regulating VEGF expression61. Moreover, proangiogenic factors from BM-MSC-derived EVs that induce endothelial cell migration through extracellular signal-regulated kinase (ERK)/Akt signaling revealed the presence of high levels of extracellular matrix metalloproteinase inducer (EMMPRIN), an important factor for endothelial activation, in these vesicles62. Single cell analysis of infarcted hearts63 profiled the expression of twenty-one paracrine factors produced by locally transplanted MSCs, provides in vivo evidence that MSCs exert a paracrine effect on surrounding cardiomyocytes to help improve cardiac function after infarction. Additional favorable outcomes including enhanced engraftment and capillary density and reduced fibrosis were observed in infarcted rats following local injection of cardiac stem cells pre-treated with MSC-derived exosomes50. Intramyocardial injection of 1.0 × 108 M-EVs can improve cardiac function in infarcted mice51. A recent study showed that mitochondria-rich extracellular vesicles (M-EVs) collected from induced pluripotent stem cell-derived cardiomyocyte (iCM)-conditioned medium following intramyocardial injection can restore intracellular bioenergetics and contractile properties51.
3.2. Cell-to-cell contact
MSCs are distinct from other cell therapies because of their cell-to-cell interactions, therapeutic effects, and a so-called “hit-and-run” mechanism. Cell-to-cell contact or heterocellular coupling64, occurs through the formation of gap junctions or tunneling nanotubes with adjacent or nearby cells, respectively. Gap junctions are comprised of six connexin molecules and form a channel between adjacent cells through which small molecules, ≤1 kDa, can travel. Tunneling nanotubes allow the transfer of larger molecules and even cell organelles, such as mitochondria between nearby cells65 (Figure 3). Both forms of communication require that the MSCs be in close proximity to the target cell and allows for the transfer of small molecules, e.g., microRNA (miRNA), peptides and organelles, such as mitochondria, from MSCs to host cells. Accumulating data implicates mitochondrial donation from MSCs as another critical component of their therapeutic efficacy. The local microenvironment of an injured cell releases physiological cues that trigger transfer of mitochondria66. The regulation of mitochondrial transport from MSCs to other cells has been attributed to MSC intrinsic expression of MIRO1, a mitochondrial Rho GTPase167. Moreover, the efficiency of this transfer is enhanced by the formation of tunneling nanotubes (TNTs) via activation of the TNF-α/NF-κB-signaling pathway. iPSC-MSCs have high intrinsic MIRO1 and are highly responsive to the pro-inflammatory cytokine TNF-α, boosting mitochondrial transfer potency compared to BM-MSCs68. In an in vivo model of myocardial infarction, mitochondria released from local damaged cells activate anti-apoptotic signals in MSCs69. There is bidirectional mitochondrial transfer between MSCs and endogenous cells40. Mitochondria from other cells can be engulfed and degraded within MSCs, leading to induction of cytoprotective enzyme HO-1, and stimulation of mitochondrial biogenesis. This activity triggers enhanced mitochondrial donation from MSCs69. Additionally, in an ex vivo model of ischemic heart disease, BM-MSCs rescued damaged cardiomyocytes through TNT-mediated mitochondrial transfer70. Mitochondrial membrane potential and function were elevated in the cardiomyocytes and apoptosis was reduced70.
Figure 3. Mechanisms by which Mesenchymal Stromal Cell (MSC) attenuate inflammation and injury.
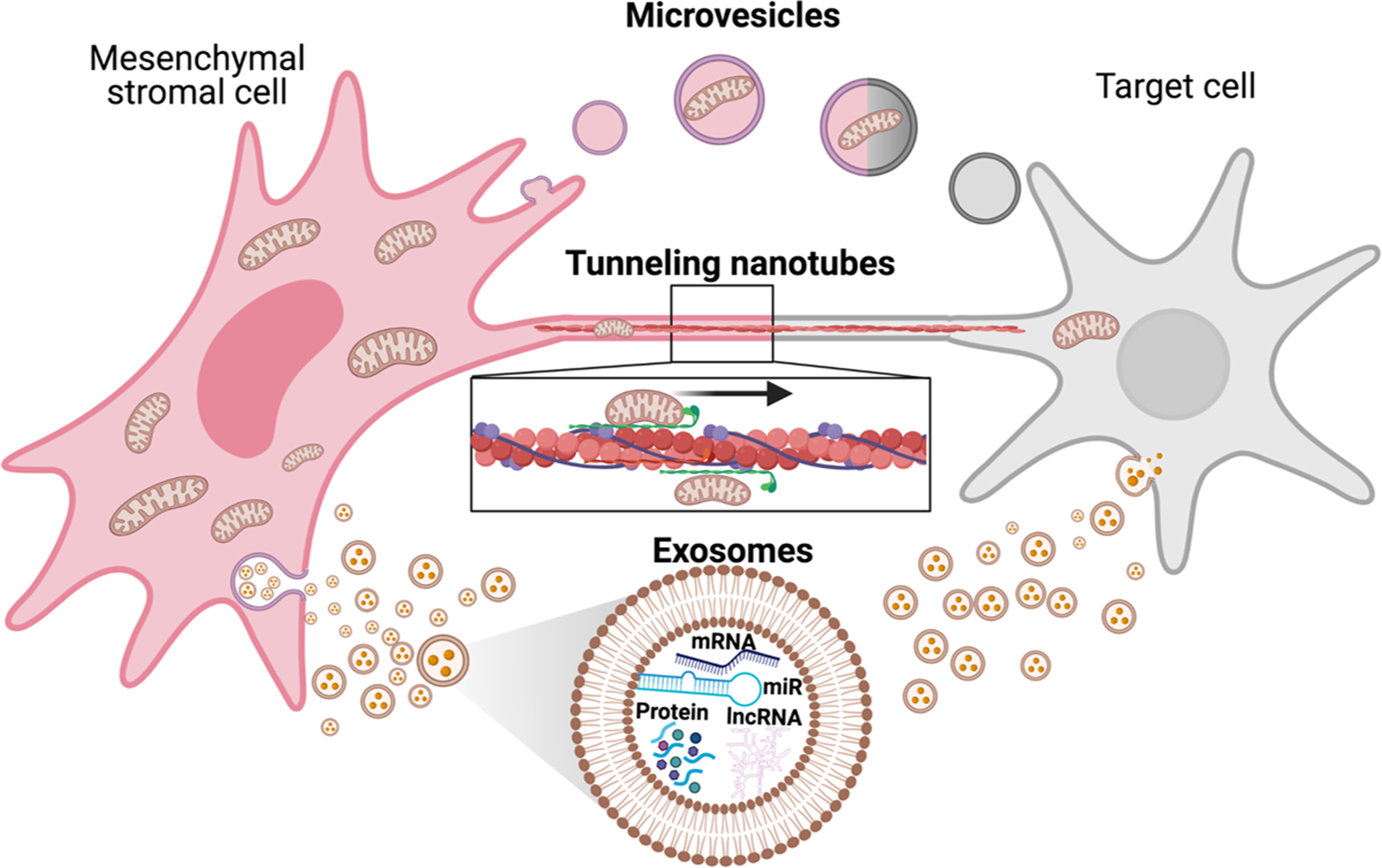
Microvesicles (MVs), membrane-bound vesicles that are released by many types of cell, including MSCs, are considered important mediators of cell-to-cell communication. MVs serve as vehicles for transferring proteins, peptides, messenger RNA and microRNA (miRNA) to alter gene expression, proliferation and differentiation of the recipient cells. Tunneling nanotubes (TNTs) are long, ultrathin structures with diameters ranging from 50 to 200 nm and a length that allows organelle transfer between two spatially separated cells. TNTs contain cytoskeletal elements such as actin and microtubules, depending on the cell type. Myosin is a fundamental protein required for organelle transfer, a process requiring high rates of ATP consumption. MSC-derived exosomes play crucial roles in intercellular communications and contain cytokines and growth factors, signaling lipids, mRNAs and regulatory miRNAs that are released into target cells by receptors, endocytosis, and fusion with plasma membrane. Figure created using BioRender.com
3.3. Immunomodulation
MSCs possess broad immunomodulation capabilities and are capable of influencing both adaptive and innate immune responses71. Current evidence suggests that MSCs exert variable immunomodulatory effects on the same types of immune cell depending upon the local microenvironment or disease status72. MSCs are extensively described as immune-privileged cells because of their lack of cell-surface histocompatibility complex (HLA) class II molecules and the presence of T-cell costimulatory molecules73. This property allows MSCs to evade immune detection and enables their use as an allogeneic therapy without concurrent immunosuppression74, 75. Additionally, MSCs, via their paracrine effects and release of EVs, interact with and inhibit the local and systemic immune system76. Modulation of the immune system occurs even while MSCs are engulfed by antigen-presenting cells (APCs)76. The subsequent interaction can result in a chain of anti-inflammatory activities and downstream beneficial therapeutic outcomes. The recognition and removal of MSCs by the host immune system is likely the greatest limitation on the duration and efficacy of many MSC-mediated therapeutic effects76.
Following the local administration of MSCs in a murine myocardial infarction model, the expression of TNF-α, IL-1 and IL-6 and the apoptosis of myocardial cells is significantly reduced, leading to significant improvement of cardiac function77. In a rat model of MI, MSCs reduced the level of CD68-positive inflammatory cells and monocyte chemotactic protein-1 (MCP-1) in the myocardium, thereby improving cardiac function78. TSG-6, a key anti-inflammatory protein secreted by MSCs, has been proposed as a surrogate biomarker predicting the therapeutic efficacy of and anti-inflammatory mediators secreted by MSCs79. Hamidian and co-workers demonstrated that IM delivery increases MSC dwell-time, resulting in sustained modulation of the inflammatory milieu. TSG-6 was released at the site of MSC delivery, while neutrophil infiltration was abrogated, and inflammation reduced at the contralateral site80. Nitric oxide (NO) is another factor that inhibits T-cell proliferation and NO produced by MSCs is implicated in contributing to T-cell suppression81. Downregulating the production of suppressor of cytokine signaling (SOCS) 1 in MSCs increased NO production and enhanced the immunosuppressive capacity of MSCs81. Chen et al. demonstrated that over-expression of eNOS/NOS3 by MSCs injected into the myocardium of rats with MI, enhances cardiac repair82. Additionally, iNOS activity is required for the anti-fibrotic therapeutic properties of MSC83.
Allogeneic MSCs appear safe and effective for the treatment of heart disease84, and their potent immunomodulatory properties have led to their widespread testing in immunologic disorders ranging from multiple sclerosis to aging frailty85, 86. However, the severity of the inflammatory environment determines the immunoregulatory effect of MSCs. It appears that the inflammatory microenvironment associated with acute MI inhibits the ability of MSCs to promote repair of the injured myocardium87. Severe inflammation causes MSCs to suppress the immune response, whereas weak inflammation leads to enhancement of the immune reaction. MSC1 and MSC2 designate the pro-inflammatory and anti-inflammatory phenotypes of MSCs, respectively88. In the absence of pro-inflammatory cytokines, the activation of TLR4 can promote differentiation of MSCs into a MSC1 phenotype. Conversely, differentiation into the MSC2 phenotype can be induced by the delivery of anti-inflammatory signals to MSCs through TLR388. A randomized, double-blind clinical trial evaluating the efficacy of human umbilical cord-derived mesenchymal stem cells (hUC-MSCs) for the treatment of lupus nephritis (LN) was abandoned after hUC-MSCs produced no additional beneficial effects over and above standard immunosuppression89. However, this failure appears to be disease-specific, since the hUC-MSC immunosuppressive effect has been clearly demonstrated in other inflammatory immune-mediated diseases90.
Zha et al.91 utilized CRISPR/Cas9 to target the MHC class I molecule, β2 microglobulin (B2M), to generate “less immunogenic” iPSC-derived MSC (iPSC-MSC) lines for allogenic transplantation. B2M-knockout (KO) iPSC-MSCs escape immune response-mediated killing by peripheral blood-derived monocytes (PBMCs) more efficiently than control cells. The loss of B2M did not alter the innate immunosuppressive feature of MSCs. Overexpressing IL-10- in MSCs using the dCas9-activation mediator system, suppressed immune cell accumulation and pro-inflammatory response in a diabetes-associated myocardial infarction model92.
3.4. Migration (Homing)
“Homing” is the ability of MSCs to respond to the sustained delivery of trophic signals and selectively traffic toward the site of injury. Site-specific homing requires either recruitment of local MSCs or transplantation of exogenous cells in close proximity to the target area. Directed migration follows activation and polarization of MSCs, during which a front pole is formed that guides interstitial locomotion by sensing a chemokine gradient released by injured or inflamed tissue. Migration is terminated after reaching the target site93. Once MSCs have homed, specific receptors or ligands expressed by the damaged tissues facilitate MSC trafficking adhesion and infiltration. The mechanisms used by MSCs to migrate and home to tissues have not been fully elucidated. It is generally assumed that circulating MSCs initially contact endothelium by tethering and rolling, resulting in a deceleration of the cells, activation of G-protein-coupled receptors, followed by integrin-mediated activation-dependent arrest. The cells must then transmigrate through the endothelium and the underlying basement membrane and through the interstitium to the site of injury. This latter step is guided by chemotactic signals released in response to tissue damage15, 41.
3.5. Improving local administration of MSCs
Multiple factors can contribute to poor retention following local administration, including the hostile environment that MSCs encounter at the disease site, causing cell death and poor engraftment into the tissue94. Priming of MSCs in vitro is a simple approach to improving retention and therapeutic efficacy following local administration. For example, hypoxic priming up-regulates expression of prosurvival factors such as Hif-1, which can contribute to MSC adaptation to the typically hypoxic disease site. Consequently, hypoxia-primed MSCs exhibit ~40% less cell death on day 3 after intramyocardial injection compared with non-primed MSCs in a rat model of MI, resulting in improved vascularization in the infarcted myocardium and greater therapeutic efficacy95. However, the effect of priming may not be preserved upon cryopreservation/thawing.
Using biomaterials to encapsulate MSCs is another promising strategy to overcome the challenges associated with local administration. Hydrogel is one of the most common biomaterials used to encapsulate MSCs and enhance their survival for several weeks following administration, but the bulk size of hydrogel is only suitable for local not systemic administration. For example, in a separate rat MI model, immunohistology studies showed that MSC survival was sustained for up to 16 days following delivery of HGF-overexpressing MSCs within a synthetic peptide-based hydrogel compared to native MSCs, which did not survive past day 2. This engineered MSC therapy demonstrated superior reduction in scar formation, accelerated angiogenesis and increased ventricular wall thickness compared with native MSCs96. Microgels are another bioengineering solution to enhance the residence time and survival of MSCs. However, the microgel may form a physical barrier that masks receptors on MSCs important for homing to disease sites, a problem that may be addressed by using additional homing ligands within the microgel97. Another innovative biomaterial is the cardiac patch98, which increases cell retention and improves cardiac function. Cardiac patches have also been used for dual stem cell therapy to treat MI98.
As described above, CRISPR/Cas9-mediated gene knockdown in MSCs has proved effective in treating diseases such as myocardial infarction99. The converse, targeted gene knock-in, where a gene is inserted into the genome via homologous recombination, resulting in overexpression of the protein, can also be beneficial. Tilokee et al. demonstrated that paracrine engineering of human cardiac stem cells to overexpress SDF-1α enhances recruitment of endogenous stem cells, promotes myocyte/vessel formation, and salvages reversibly damaged myocardium to enhance cardiac repair in a mouse model of MI100. These and other cell pre-conditioning and genetic modifications are promising options for augmenting MSC- and other stem cell-based therapies101 and represent viable approaches for improving treatment for a wide variety of diseases.
3.6. Safety and tumorgenicity
While MSCs exert positive outcomes in numerous diseases, there are a few concerns regarding their tumorigenic potential that must be addressed. The possibility of tumorigenic transformations in MSCs is minimal compared to other stem cell sources such as pluripotent stem cells (iPSCs and embryonic stem cells), and while spontaneous malignant transformations of human MSCs, and the injection of these transformed cells has led to the development of tumors in mice102. MSCs can also home to tumor sites and contribute to tumor growth and progression because of their immunosuppressive properties. In a preclinical model of breast cancer, MSCs injected directly into a site containing a pre-existing tumor can promote metastasis, possibly through the induction of epithelial-to-mesenchymal transition (EMT) of the primary tumor cells103. Clinically, there are no reports of tumors in patients originating from administered MSCs, demonstrating that following current Good Manufacturing Practices (GMP) by closely monitoring and minimizing the time in culture needed for in vitro expansion and karyotyping cells to detect cytogenic aberrations before the cells are released, is crucial for eliminating any malignant potential of MSCs104.
The utilization of MSCs as delivery vehicles for different types of anticancer therapy has been an emerging concept pursued by several research groups105, 106. Briefly, the “suicide gene” strategy foresees the insertion of a gene that enables selective targeting of the transfected cells by the subsequent administration of an otherwise nontoxic drug. When this drug is administered after MSCs home to a tumor, the conversion/uptake of the then toxic drug, kills not only MSCs but also the surrounding tumor and stromal cells107. These suicide genes can encode either an enzyme by Gene-directed enzyme-producing therapy (GDEPT) or the sodium/iodide symporter, NIS. The next challenge is to understand better the interactions between MSCs and cancer cells in order to improve the clinical safety of these MSC-based therapeutic approaches.
4. Efficacy and safety of the local administration of MSCs for specific diseases
As of 2018, the delivery of MSCs in registered clinical trials was split nearly evenly between systemic and local delivery, with the majority of late-phase clinical trials using local delivery108, e.g., via intrathecal, intralesional and endocardial routes, for the treatment of back pain, perianal fistulas and chronic heart failure, respectively97. The direct in-situ administration of MSCs represents a more controlled delivery approach to directly access the local injury, generally resulting in better therapeutic responses9. For example, a meta-analysis of preclinical MSC studies in ischemic stroke models showed that administering MSCs to the damaged site is more effective at improving the neurological severity score than intra-arterial or intravascular MSC injections109, although direct injection, intra-arterial and intra-venous, consistently also demonstrated significant improvement in outcomes109.
4.1. Cardiovascular efficacy
Local injection of MSCs into the cardiovascular system produces positive outcomes. In general, intracoronary and intramyocardial (epicardial and transendocardial) injections are the two most widely used methods of delivery of cellular therapies in cardiovascular disease110. Intracoronary injections deliver cells into one of the major coronary arteries (left anterior descending, left circumflex, or right coronary arteries). This administration route is less invasive than intramyocardial injection, which typically involves surgical intervention or endocardial access, and some studies have reported intracoronary and intramyocardial injections to be equally effective110. A meta-analysis of both preclinical and clinical studies of MSC therapy in acute myocardial infarction concluded that transendocardial stem cell injection (TESI) exhibits the greatest infarct size reduction and left ventricle ejection fraction (LVEF) increase. In contrast, intracoronary delivery demonstrated no improvement9.
In the heart, TESI seems to be the favored method for the local administration of MSCs with a minimally invasive, catheter-based route of delivery, where cells are injected directly into the myocardium through the endocardium9. Swine studies using TESI as the delivery route revealed both a reduction in infarct scar and improvement of LVEF111, 112. TESI also improved LVEF in acute myocardial infarction (AMI) clinical trials113. Nevertheless, there are still clinical challenges associated with local administration that impede therapeutic efficacy, mostly due to insufficient retention and survival of transplanted MSCs at the administration site.
4.2. Neurologic efficacy
MSCs have attracted much attention for their potential to treat neurologic disorders114. In the context of neuronal damage, a local injection of MSCs to the lesion site in a rat stroke model improved coordinated function, inhibited scar tissue formation and cell apoptosis, and stimulated angiogenesis114.
Neurorestorative and neuroprotective effects as a tissue repair property of MSCs, are characterized primarily by two mechanisms of action: (1) neurogenic differentiation and cell replacement, and (2) secretion of neurotrophic factors. MSCs can significantly alleviate ischemic injury, and the rescue arises from the differentiation of transplanted cells into neurons and astrocytes115. In contrast, the paracrine effects of MSCs on nerve regeneration occurs via the secretion of neurotrophic factors116. The inoculation of cortical neurons with (exogenous) MSC-derived exosomes boosts their growth-promoting and target activation effects117, while MSC-conditioned medium enhances Schwann cell viability and proliferation via increases in nerve growth factor (NGF) and brain-derived neurotrophic factor (BDNF) expression116.
In Alzheimer’s disease, MSC-derived exosomes play a potential role in promoting neurite outgrowth, suggesting the possibility of their clinical use118. Recent findings indicate that hMSC-derived EVs protect hippocampal neurons via blocking oxidative stress and synapse damage following exposure to amyloid-beta oligomers (AβOs)119. The neuroprotection mechanism of MSC-derived EVs is related to their cargo. Those carrying antioxidant enzymes, such as catalase120, can be neuroprotective. Exosomes derived from hypoxia-preconditioned MSCs significantly enhance expression of the synaptic proteins Synapsin 1 and PSD95121, proteins that help to maintain normal synaptic function. Moreover, MSC-derived exosomes can also transfer miRs that promote the recovery of neural function, such as miR-133b, into astrocytes and neurons122.
4.3. Orthopedic efficacy
In recent years, local intra-articular injection of MSCs promotes the regeneration and repair of cartilage tissue and alleviates the degeneration caused by osteoarthritis (OA). Zhou et al.123 found that local intra-articular injection of adipose-derived MSCs (AD-MSCs) effectively alleviate OA in rat models by reducing the secretion of pro-inflammatory cytokines through induction of autophagy. Toghraie et al.124 reported that a single dose of 1 × 106/mL AD-MSCs injected into the joint cavity in a OA rabbit model significantly repaired and improved cartilage tissue 8 weeks post-OA. A phase I/II trial indicated that BM-MSCs injected into the knee of patients with OA was associated with cartilage biomarker expression, reduced synovial inflammation, pain and symptom mitigation, without any serious adverse events125. Another proof-of-concept phase I/II clinical trial showed that intra-articular injection of 1.0 × 108 AD-MSCs into OA knees improved function and reduced pain in the knee joint and reduced cartilage defects by regeneration of hyaline-like articular cartilage without causing adverse events126.
The local injection of BM- or AD-MSCs significantly improved bone healing. Despite differences in molecular cues between BM- and AD-MSCs, both cell types induced comparable amounts and properties of bone formation127. Bone marrow aspirates directly injected into the fracture site successfully repaired 53 of 60 unconsolidated fractures, and the local injection of osteoblasts also accelerated bone repair in long bone fractures128. A single local administration of MSCs in a rat distraction osteogenesis model accelerated early bone consolidation coincident with the serum level SDF-1 and the ratio of circulating MSCs reaching the highest level at the lengthening phase129.
MSCs may also stimulate cartilage regeneration by their interaction with synovial macrophages, leading to a reduction in proinflammatory cytokines such as IL1β. Indeed, MSCs administered into an OA knee joint contact synovial macrophages130, and were able to induce polarization toward M2 cells, which promote tissue repair131. In agreement with these findings, Satué et al. also found evidence that intraarticular-injected MSCs decrease the inflammatory response caused by cartilage injury and promote cartilage regeneration132.
MSCs can not only differentiate into tendon cells (tenocytes), but also modulate inflammation and tissue healing133. Several clinical trials investigating the use of MSCs for tendon healing are ongoing (NCT03688308, NCT01788683, NCT02484950, NCT03449082, NCT03279796, NCT03752827, NCT03454737)133. Six patients suffering from chronic epicondylitis were treated with local allogenic AD-MSCs injections. After 52 weeks, the visual analogic scale (VAS) and the modified Mayo Clinic Performance Index (mMCPI) were decreased by 52%, and increased by 26.6%, respectively, and on ultrasound examination, a reduction in defect areas was observed134. Subjects with rotator cuff tears (RCT) who did not respond to physical therapy for at least 6 weeks were randomly assigned to receive a single local injection of, on average, 11.4 × 106 autologous adipose-derived regenerative cells UA-ADRCs or corticosteroid injections. ADMSCs were safe and led to improved shoulder function without adverse effects at 12-month follow-up135.
4.4. Dermatologic efficacy
In dermatology, topically applied MSCs elicit improved outcomes, wound healing, and skin graft survival due to burns, diabetes and other chronic diseases136. Preclinical data demonstrate that local injection of BM-MSCs into an incisional full-thickness wound significantly shortens the healing time while stimulating angiogenesis, re-epithelialization and granulation136. Preclinical and early human trials demonstrate accelerated wound healing of diabetic ulcers following BM-MSCs application136. A fibrin polymer spray system to apply MSCs improved wound closure rates in a preclinical model as well as in patients with chronic non-healing lower extremity wounds137. For local skin wounds, human (h)AD-MSC-exosomes markedly shortened healing time and enhanced re-epithelialization138. However, hAD-MSC-exosomes alone are inadequate for the treatment of extensive burns and scalds139. Combining topical and intravenous injection of hAD-MSCs and hAD-MSC-exosomes offers the additional benefit of promoting wound healing, accelerating re-epithelialization, reducing scar widths, and enhancing angiogenesis and collagen synthesis138. Possible mechanisms by which AD-MSCs promote wound healing include reduction of inflammation, induction of angiogenesis, promotion of keratinocyte and fibroblast growth, and reduction of tissue scarring140. AD-MSCs may reduce inflammation by inducing conversion of M1 macrophages, associated with chronic wounds, into the anti-inflammatory and wound healing M2 phenotype141. Inhibition of extracellular matrix (ECM) degradation by AD-MSCs occurs through increased binding of matrix metalloproteinases (MMPs) and secretion of tissue inhibitors of metalloproteinases (TIMPs)142.
A single injection of 5 × 106 allogeneic WJ-MSCs into selected alopecia areata (AA) foci, produced an average of 67% hair regrowth at the sites where cell suspension was administered 6 months after treatment in all patients. This therapy was safe and had no side effects143. Patients affected by androgenetic alopecia (AGA) have also been treated with human follicular stem cells (HFSCs) obtained by centrifugation of scalp punch biopsies. Twenty-three weeks after the last treatment with HFSCs a 29%±5% increase in mean hair density in the treated area over baseline values, whereas there was only a 1% increase in hair density for the placebo-treated area144. Other studies have established a role of autologous human hair follicle mesenchymal stem cells (HF-MSCs) for therapeutic hair regrowth. A placebo-controlled, randomized, evaluator-blinded, half-head group study to compare hair regrowth with micrograft-containing HF-MSCs vs. placebo was reported145. After 58 weeks, 27 patients displayed an increased hair count and density within the targeted area, of 18.0 hairs per 0.65 cm2 and 23.3 hairs per cm2, respectively, compared with baseline, while the control area displayed a mean decrease of 1.1 hairs per 0.65 cm2 and 0.7 hairs per cm2145, respectively. Srifa et al.146 performed site-specific mutagenesis and integration of exogenous DNA in BM-, AT-, and UC-derived hMSCs using an optimized Cas9-AAV6-based genome editing tool platform generating cells that worked as transient therapeutic agents within the wound bed of db/db mice146.
4.5. Gastroenterology efficacy
MSC treatment has recently been approved by the European Medicines Agency (EMA) for the treatment for perianal fistulizing Crohn’s disease. Darvadstrocel, composed of MSCs, is safe and effective for inducing fistula healing when the cells are injected into both internal and external openings, as well as inside the fistula tracks147.
5. Situations where systemic delivery of MSCs is the best choice
Human diseases and disorders such as frailty and COVID-19, where the most detrimental symptoms are mediated by increased activity of the immune system, are some of the best candidates for IV administration of MSCs. This approach results in numerous MSCs accumulating in the lungs, but also distributed throughout the body and other organs, such as the spleen, within 24–48 hours30.
IV infusion of MSCs for frailty has been tested in Phase I85 and Phase II148 clinical trials. Frailty, a primarily geriatric syndrome that increases in incidence with advancing age, is characterized by multiple systemic conditions including sarcopenia, inflammation, and diminution of physical performance, often culminating in an inability to perform activities of daily living149. These small, early-stage studies demonstrated that administering allogeneic MSCs obtained from healthy young adults to frail older adults is safe and potentially efficacious. Cell treatment ameliorated signs and symptoms of frailty, producing improvements in physical activity, quality of life, cognitive status, and inflammatory markers150. Compared to autologous MSCs from these frail individuals, allogeneic cells are thought to be more therapeutic since they are not burdened by patient co-morbidities. Administering MSCs obtained from young, healthy adults to frail patients, improved the functions of multiple organs, including lung, heart, and the immune system151–153.
The recent (ongoing) COVID-19 pandemic has negatively impacted public health on a global scale and is associated with an extremely high mortality rate. There has been an urgent need for an effective therapy to treat COVID-19 patients. A primary cause of death in patients infected with SARS-CoV-2, (the virus that causes COVID-19) is acute respiratory distress syndrome (ARDS), an inflammatory condition caused primarily by an overactive immune response154. MSCs, with their immune-moderating properties, as well as their regenerative potential and antimicrobial properties, were assessed for their efficacy against the effects of COVID-19155. IV administration of allogeneic human MSCs proved successful in reducing mortality and other effects related to SARS-CoV-2 infections155. To date, there are ~70 clinical trials registered on clinicaltrials.gov designed to evaluate the use of MSCs in COVID-19 patients. However, most of these trials are either incomplete or the outcomes are not published156. In one case report, the triple IV infusion of UC-MSCs into a critically ill COVID-19 patient was well tolerated and resulted in reduced serum C-reactive protein (CRP), normalized white blood cell counts, and alleviated the effects of pneumonia157. In a 51-year-old male patient with multi-organ involvement due to SARS-CoV-2 infection and who experienced cardiac arrest, MSCs were systemically transplanted four times plus once intrathecally. Following the first MSC administration, the values of AST, ALT, LDH, CK, pro-BNP, ferritin, triglyceride, fibrinogen, ammonia, and myoglobin began decreasing. After the second injection, CRP reached normal values. This patient also exhibited very low ejection fraction (EF; 25%) that responded to the systematic administration of MSCs; with EF increasing to 60%. The authors concluded that the MSCs had a therapeutic effect on the heart. After the fourth MSC dose, the patient’s heart functions returned to normal158.
Leng et al.159, showed that 7 SARS-CoV-2 positive patients, with COVID-19 pneumonia (study group), exhibited significantly improved pulmonary functional activity after an intravenous administration of clinical-grade MSCs. Compared to the placebo-treated controls, patients in the MSC-treated group experienced normalization of immune cell populations, reduced serum TNF-α, and increased IL-10159. The results of this work suggest the possibility of using autologous or allogeneic adipose stem cells (ASCs) administered either intravenously or directly through a ventilation mask (aerosol)160–162. Tao et al.156 reported a single COVID-19 critical patient treated with MSCs and lung transplantation. This patient was admitted with the diagnosis of COVID-19, ARDS, type-2 diabetes, diabetic nephropathy, renal insufficiency, and hypertension. His situation continued to worsen and became life-threatening, even after receiving various traditional treatment options, including antiviral therapy and extracorporeal membrane oxygenation. The patient then received five intravenous infusions of MSCs. Lymphocytes increased and renal function improved, static pulmonary compliance increased significantly, and the PaO2/FiO2 ratio stabilized. All these improvements delayed the severe deterioration of the patient’s condition, gaining valuable time needed to find a suitable lung donor and receive a lung transplant156.
In a patient with severe SARS-CoV-2-induced pneumonia, administration of Wharton’s Jelly-derived MSCs resulted in resolution of fever and shortness of breath within two days and a significant reduction in ground-glass opacity and pneumonia infiltration after six days. Functional improvement of this patient was associated with an increased number of T cell and a reduction in inflammatory mediators such as CRP, IL-6, and TNF-α163.
Together, the data from these reports suggest that the systemic administration of MSCs to patients with severe manifestations of SARS-CoV-2 infection is beneficial and resolves disease symptoms.
6. Expert Opinion
As the growth of MSC based clinical trials advances, it is vitally important to remember historical safety concerns, recognize modern clinical risks, and use methodology and delivery consistent with the intended mechanism of action to produce the most effective, safe, economically viable and ethical therapeutic approaches. Knowledge gaps remain in the understanding of mechanism(s) underlying efficacy of MSCs, which could be unique in different tissues. We must determine if MSCs from different tissues are more therapeutic for distinct diseases or if allogeneic MSCs are more therapeutic than autologous MSCs in all or only specific diseases. Given the plasticity and the paracrine-mediated immunomodulatory activity of MSCs, they are increasingly being studied for their effectiveness in a variety of clinical settings, presenting promising outcomes.
We discussed critical aspects of the effective and safe delivery of MSCs in the context of preclinical and clinical studies by focusing on the mechanism of action when these cells are administered via local injection. This route of administration appears to be more efficacious than delivering cells through the circulation for most diseases. However, bioengineered patches containing MSCs are also useful, albeit requiring more invasive surgical procedures, and systemic delivery may be optimal for certain diseases, such as frailty and COVID-19. Therefore, determining the best route(s) of MSC administration is an ongoing, disease-specific process.
One of the biggest challenges facing MSC-based therapy is the optimization of cell expansion to avoid development of aneuploidy in vitro, which has potential to promote cancer development or progression in vivo. For the future, it is imperative to understand how MSCs communicate with tumor cells and within the tumor stroma. Interestingly, an exciting new area of investigations is focused upon the cell secretome rather than the cells themselves. As discussed above, recent studies suggest that a large proportion of the damage repair can be attributed to a paracrine mechanism including EVs and exosomes, membrane-bound vesicles that are released by the cells. MSC-derived EVs and exosomes have gained significant interest in regenerative medicine due to their ability to promote tissue homeostasis and angiogenesis and inhibit inflammation, thereby stimulating recovery in a variety of diseases. Additionally, unlike cell therapy, EVs and exosomes eliminate the risk of aneuploidy and reduce immune rejection following allogeneic administration. Therefore, EV therapy is being considered as an alternative to MSC therapy and may prove to be the next generation cellular therapeutic for many diseases.
Despite promising pre-clinical data with EVs and exosomes, several challenges impede the translation of this therapy into clinics, including improved characterization methods for documented reproducibility, large-scale production, isolation and processing of clinical-grade, FDA compliant exosome products. Traditional EV production techniques are often limited in their clinical translation due to the need for repeated and lengthy manufacturing protocols and time-consuming characterization of each product lot. Furthermore, the need for repetitive lot productions of cell products often leads to greater batch-to-batch variability and the need for even more replicates and testing time.
Future studies must focus on the role and mechanism(s) of the MSC secretome. Are these effects mediated exclusively through paracrine signaling, or must some of these materials be transferred by direct cell-cell contact? We must elucidate the molecular mechanisms that function in specific organs/tissues/diseases to guide the choice of the delivery strategy in order to optimize treatment of each disease.
Article Highlights:
It is essential to determine the delivery route and dosing of cell therapy for optimal clinical translation, given the important influences on the distribution, retention, and survival of the administered cells.
Local administration of mesenchymal stromal cells (MSCs) into target tissues has important advantages, including rapid and localized reaction. Cells can be administered into a precise, targeted location, increasing the chance of engraftment and/or local paracrine activity, which has the potential to prolong and/or enhance therapeutic potential.
The mechanism of action of MSCs can be attributed to secretion of paracrine factors, including extracellular vesicles and cytokines, transfer of mitochondria to nearby cells via hetero-cellular coupling, and modification of immune responses.
Local, rather than systemic, transplantation of MSCs influences the paracrine potency in the production of trophic factors. Certain paracrine signals are transmitted over short distances, thereby producing local effects, and the crosstalk between the local microenvironment of injured host tissues and MSCs activates MSC production of cytoprotective paracrine factors.
Biomaterials, cell pre-conditioning, priming and genetic modifications represent promising approaches for improving local administration of MSCs in the treatment of a wide variety of diseases.
Local injections of MSCs have been tested for specific diseases including those affecting the cardiovascular, neurologic, orthopedic, dermatologic and gastroenterologic systems.
Systemic MSC infusions have been tested in numerous settings including but not limited to aging frailty, Alzheimer’s disease, COVID-19, idiopathic pulmonary fibrosis, and congestive heart failure.
Funding
This work was funded by the National Institutes of Health (NIH) grant, 1R01 HL107110, and 1R01 HL13735 to JMH. JMH is also supported by NIH grants 5UM1 HL113460, 1R01 HL134558, 5R01429 CA136387, and HHSN268201600012I, Department of Defense grant W81XWH-19-PRMRP-CTA and The Lipson Family and Starr Foundations.
Declaration of Interests
Dr. Joshua Hare previously owned equity in Biscayne Pharmaceuticals, licensee of intellectual property used in this study. Biscayne Pharmaceuticals did not provide funding for this study. Dr. Joshua Hare is the Chief Scientific Officer, a compensated consultant and advisory board member for Longeveron and holds equity in Longeveron. Dr. Hare is also the co-inventor of intellectual property licensed to Longeveron. Longeveron did not play a role in the design, conduct, or funding of the study. Dr. Hare’s relationships are reported to the University of Miami, and an appropriate management plan is in place. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Footnotes
Reviewer Disclosures
Peer reviewers on this manuscript have no relevant financial relationships or otherwise to disclose.
References
- 1.Charbord P Bone marrow mesenchymal stem cells: historical overview and concepts. Hum Gene Ther 2010. Sep;21(9):1045–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Strioga M, Viswanathan S, Darinskas A, Slaby O, Michalek J. Same or not the same? Comparison of adipose tissue-derived versus bone marrow-derived mesenchymal stem and stromal cells. Stem Cells Dev 2012. Sep 20;21(14):2724–52. [DOI] [PubMed] [Google Scholar]
- 3.Pelekanos RA, Sardesai VS, Futrega K, Lott WB, Kuhn M, Doran MR. Isolation and Expansion of Mesenchymal Stem/Stromal Cells Derived from Human Placenta Tissue. J Vis Exp 2016. Jun 6(112). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sharpe PT. Dental mesenchymal stem cells. Development 2016. Jul 1;143(13):2273–80. [DOI] [PubMed] [Google Scholar]
- 5.Lee OK, Kuo TK, Chen WM, Lee KD, Hsieh SL, Chen TH. Isolation of multipotent mesenchymal stem cells from umbilical cord blood. Blood 2004. Mar 1;103(5):1669–75. [DOI] [PubMed] [Google Scholar]
- 6.Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D, et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006;8(4):315–7. [DOI] [PubMed] [Google Scholar]
- 7.Pires AO, Mendes-Pinheiro B, Teixeira FG, Anjo SI, Ribeiro-Samy S, Gomes ED, et al. Unveiling the Differences of Secretome of Human Bone Marrow Mesenchymal Stem Cells, Adipose Tissue-Derived Stem Cells, and Human Umbilical Cord Perivascular Cells: A Proteomic Analysis. Stem cells and development 2016. Jul 15;25(14):1073–83. [DOI] [PubMed] [Google Scholar]
- 8.Shi Y, Wang Y, Li Q, Liu K, Hou J, Shao C, et al. Immunoregulatory mechanisms of mesenchymal stem and stromal cells in inflammatory diseases. Nat Rev Nephrol 2018. Aug;14(8):493–507. [DOI] [PubMed] [Google Scholar]
- 9.Kanelidis AJ, Premer C, Lopez J, Balkan W, Hare JM. Route of Delivery Modulates the Efficacy of Mesenchymal Stem Cell Therapy for Myocardial Infarction: A Meta-Analysis of Preclinical Studies and Clinical Trials. Circulation research 2017. Mar 31;120(7):1139–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Leibacher J, Henschler R. Biodistribution, migration and homing of systemically applied mesenchymal stem/stromal cells. Stem Cell Res Ther 2016. Jan 11;7:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Li J, Hu S, Zhu D, Huang K, Mei X, Lopez de Juan Abad B, et al. All Roads Lead to Rome (the Heart): Cell Retention and Outcomes From Various Delivery Routes of Cell Therapy Products to the Heart. J Am Heart Assoc 2021. Apr 20;10(8):e020402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Xie C, Yang Z, Suo Y, Chen Q, Wei D, Weng X, et al. Systemically Infused Mesenchymal Stem Cells Show Different Homing Profiles in Healthy and Tumor Mouse Models. Stem Cells Transl Med 2017. Apr;6(4):1120–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Luger D, Lipinski MJ, Westman PC, Glover DK, Dimastromatteo J, Frias JC, et al. Intravenously Delivered Mesenchymal Stem Cells: Systemic Anti-Inflammatory Effects Improve Left Ventricular Dysfunction in Acute Myocardial Infarction and Ischemic Cardiomyopathy. Circ Res 2017. May 12;120(10):1598–613. [DOI] [PubMed] [Google Scholar]
- 14.Pittenger MF, Discher DE, Peault BM, Phinney DG, Hare JM, Caplan AI. Mesenchymal stem cell perspective: cell biology to clinical progress. NPJ Regen Med 2019;4:22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.De Becker A, Riet IV. Homing and migration of mesenchymal stromal cells: How to improve the efficacy of cell therapy? World J Stem Cells 2016. Mar 26;8(3):73–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zhang Q, Nguyen P, Xu Q, Park W, Lee S, Furuhashi A, et al. Neural Progenitor-Like Cells Induced from Human Gingiva-Derived Mesenchymal Stem Cells Regulate Myelination of Schwann Cells in Rat Sciatic Nerve Regeneration. Stem Cells Transl Med 2017. Feb;6(2):458–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Ueda N, Atsuta I, Ayukawa Y, Yamaza T, Furuhashi A, Narimatsu I, et al. Novel Application Method for Mesenchymal Stem Cell Therapy Utilizing Its Attractant-Responsive Accumulation Property. Appl Sci-Basel 2019. Nov 2;9(22). [Google Scholar]
- 18.Masterson CH, Tabuchi A, Hogan G, Fitzpatrick G, Kerrigan SW, Jerkic M, et al. Intra-vital imaging of mesenchymal stromal cell kinetics in the pulmonary vasculature during infection. Sci Rep 2021. Mar 4;11(1):5265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hoogduijn MJ, Roemeling-van Rhijn M, Engela AU, Korevaar SS, Mensah FK, Franquesa M, et al. Mesenchymal stem cells induce an inflammatory response after intravenous infusion. Stem Cells Dev 2013. Nov 1;22(21):2825–35. [DOI] [PubMed] [Google Scholar]
- 20.Liu Z, Mikrani R, Zubair HM, Taleb A, Naveed M, Baig M, et al. Systemic and local delivery of mesenchymal stem cells for heart renovation: Challenges and innovations. Eur J Pharmacol 2020. Jun 5;876:173049. [DOI] [PubMed] [Google Scholar]
- 21.Watanabe M, Yavagal DR. Intra-arterial delivery of mesenchymal stem cells. Brain Circ 2016. Jul-Sep;2(3):114–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Yavagal DR, Lin B, Raval AP, Garza PS, Dong C, Zhao W, et al. Efficacy and dose-dependent safety of intra-arterial delivery of mesenchymal stem cells in a rodent stroke model. PloS one 2014;9(5):e93735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Argibay B, Trekker J, Himmelreich U, Beiras A, Topete A, Taboada P, et al. Intraarterial route increases the risk of cerebral lesions after mesenchymal cell administration in animal model of ischemia. Sci Rep 2017. Jan 16;7:40758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Guzman R, Janowski M, Walczak P. Intra-Arterial Delivery of Cell Therapies for Stroke. Stroke 2018. May;49(5):1075–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Sarmah D, Agrawal V, Rane P, Bhute S, Watanabe M, Kalia K, et al. Mesenchymal Stem Cell Therapy in Ischemic Stroke: A Meta-analysis of Preclinical Studies. Clinical pharmacology and therapeutics 2018. Jun;103(6):990–98. [DOI] [PubMed] [Google Scholar]
- 26.Suk KT, Yoon JH, Kim MY, Kim CW, Kim JK, Park H, et al. Transplantation with autologous bone marrow-derived mesenchymal stem cells for alcoholic cirrhosis: Phase 2 trial. Hepatology 2016. Dec;64(6):2185–97. [DOI] [PubMed] [Google Scholar]
- 27.Saad A, Dietz AB, Herrmann SMS, Hickson LJ, Glockner JF, McKusick MA, et al. Autologous Mesenchymal Stem Cells Increase Cortical Perfusion in Renovascular Disease. J Am Soc Nephrol 2017. Sep;28(9):2777–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bazhanov N, Ylostalo JH, Bartosh TJ, Tiblow A, Mohammadipoor A, Foskett A, et al. Intraperitoneally infused human mesenchymal stem cells form aggregates with mouse immune cells and attach to peritoneal organs. Stem Cell Res Ther 2016. Feb 10;7:27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Nam Y, Jung SM, Rim YA, Jung H, Lee K, Park N, et al. Intraperitoneal infusion of mesenchymal stem cell attenuates severity of collagen antibody induced arthritis. PLoS One 2018;13(6):e0198740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lee RH, Pulin AA, Seo MJ, Kota DJ, Ylostalo J, Larson BL, et al. Intravenous hMSCs improve myocardial infarction in mice because cells embolized in lung are activated to secrete the anti-inflammatory protein TSG-6. Cell Stem Cell 2009. Jul 2;5(1):54–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wang M, Liang C, Hu H, Zhou L, Xu B, Wang X, et al. Intraperitoneal injection (IP), Intravenous injection (IV) or anal injection (AI)? Best way for mesenchymal stem cells transplantation for colitis. Sci Rep 2016. Aug 4;6:30696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ezquer M, Urzua CA, Montecino S, Leal K, Conget P, Ezquer F. Intravitreal administration of multipotent mesenchymal stromal cells triggers a cytoprotective microenvironment in the retina of diabetic mice. Stem Cell Res Ther 2016. Mar 16;7:42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Petrella F, Spaggiari L, Acocella F, Barberis M, Bellomi M, Brizzola S, et al. Airway fistula closure after stem-cell infusion. N Engl J Med 2015. Jan 1;372(1):96–7. [DOI] [PubMed] [Google Scholar]
- 34.Qazi TH, Duda GN, Ort MJ, Perka C, Geissler S, Winkler T. Cell therapy to improve regeneration of skeletal muscle injuries. J Cachexia Sarcopenia Muscle 2019. Jun;10(3):501–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Himeoka Y, Kaneko K. Enzyme oscillation can enhance the thermodynamic efficiency of cellular metabolism: consequence of anti-phase coupling between reaction flux and affinity. Phys Biol 2016. Apr 5;13(2):026002. [DOI] [PubMed] [Google Scholar]
- 36.van den Akker F, Feyen DA, van den Hoogen P, van Laake LW, van Eeuwijk EC, Hoefer I, et al. Intramyocardial stem cell injection: go(ne) with the flow. Eur Heart J 2017. Jan 14;38(3):184–86. [DOI] [PubMed] [Google Scholar]
- 37.Li H, Rong P, Ma X, Nie W, Chen C, Yang C, et al. Paracrine effect of mesenchymal stem cell as a novel therapeutic strategy for diabetic nephropathy. Life Sci 2018. Dec 15;215:113–18. [DOI] [PubMed] [Google Scholar]
- 38.Fiore EJ, Dominguez LM, Bayo J, Garcia MG, Mazzolini GD. Taking advantage of the potential of mesenchymal stromal cells in liver regeneration: Cells and extracellular vesicles as therapeutic strategies. World J Gastroenterol 2018. Jun 21;24(23):2427–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Leuning DG, Beijer NRM, du Fosse NA, Vermeulen S, Lievers E, van Kooten C, et al. The cytokine secretion profile of mesenchymal stromal cells is determined by surface structure of the microenvironment. Sci Rep 2018. May 16;8(1):7716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Patananan AN, Sercel AJ, Wu TH, Ahsan FM, Torres A Jr., Kennedy SAL, et al. Pressure-Driven Mitochondrial Transfer Pipeline Generates Mammalian Cells of Desired Genetic Combinations and Fates. Cell Rep 2020. Dec 29;33(13):108562. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ullah M, Liu DD, Thakor AS. Mesenchymal Stromal Cell Homing: Mechanisms and Strategies for Improvement. iScience 2019. May 31;15:421–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Weiss ARR, Dahlke MH. Immunomodulation by Mesenchymal Stem Cells (MSCs): Mechanisms of Action of Living, Apoptotic, and Dead MSCs. Front Immunol 2019;10:1191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Xia X, Chan KF, Wong GTY, Wang P, Liu L, Yeung BPM, et al. Mesenchymal stem cells promote healing of nonsteroidal anti-inflammatory drug-related peptic ulcer through paracrine actions in pigs. Sci Transl Med 2019. Oct 30;11(516). [DOI] [PubMed] [Google Scholar]
- 44.Zriek F, Di Battista JA, Alaaeddine N. Mesenchymal Stromal Cell Secretome: Immunomodulation, Tissue Repair and Effects on Neurodegenerative Conditions. Curr Stem Cell Res Ther 2021. Feb 2. [DOI] [PubMed] [Google Scholar]
- 45.Shin S, Lee J, Kwon Y, Park KS, Jeong JH, Choi SJ, et al. Comparative Proteomic Analysis of the Mesenchymal Stem Cells Secretome from Adipose, Bone Marrow, Placenta and Wharton’s Jelly. Int J Mol Sci 2021. Jan 15;22(2). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Trzyna A, Banas-Zabczyk A. Adipose-Derived Stem Cells Secretome and Its Potential Application in “Stem Cell-Free Therapy”. Biomolecules 2021. Jun 13;11(6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Donders R, Bogie JFJ, Ravanidis S, Gervois P, Vanheusden M, Maree R, et al. Human Wharton’s Jelly-Derived Stem Cells Display a Distinct Immunomodulatory and Proregenerative Transcriptional Signature Compared to Bone Marrow-Derived Stem Cells. Stem cells and development 2018. Jan 15;27(2):65–84. [DOI] [PubMed] [Google Scholar]
- 48.Park KS, Bandeira E, Shelke GV, Lasser C, Lotvall J. Enhancement of therapeutic potential of mesenchymal stem cell-derived extracellular vesicles. Stem Cell Res Ther 2019. Sep 23;10(1):288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Karantalis V, Suncion-Loescher VY, Bagno L, Golpanian S, Wolf A, Sanina C, et al. Synergistic Effects of Combined Cell Therapy for Chronic Ischemic Cardiomyopathy. Journal of the American College of Cardiology 2015. Nov 3;66(18):1990–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Zhang Z, Yang J, Yan W, Li Y, Shen Z, Asahara T. Pretreatment of Cardiac Stem Cells With Exosomes Derived From Mesenchymal Stem Cells Enhances Myocardial Repair. Journal of the American Heart Association 2016. Jan 25;5(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Ikeda G, Santoso MR, Tada Y, Li AM, Vaskova E, Jung JH, et al. Mitochondria-Rich Extracellular Vesicles From Autologous Stem Cell-Derived Cardiomyocytes Restore Energetics of Ischemic Myocardium. Journal of the American College of Cardiology 2021. Mar 2;77(8):1073–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Phinney DG, Pittenger MF. Concise Review: MSC-Derived Exosomes for Cell-Free Therapy. Stem Cells 2017. Apr;35(4):851–58. [DOI] [PubMed] [Google Scholar]
- 53.Fisher SA, Doree C, Mathur A, Taggart DP, Martin-Rendon E. Stem cell therapy for chronic ischaemic heart disease and congestive heart failure. Cochrane Database Syst Rev 2016. Dec 24;12:CD007888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Gupta A, Cady C, Fauser AM, Rodriguez HC, Mistovich RJ, Potty AGR, et al. Cell-free Stem Cell-Derived Extract Formulation for Regenerative Medicine Applications. Int J Mol Sci 2020. Dec 9;21(24). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Sung DK, Chang YS, Ahn SY, Sung SI, Yoo HS, Choi SJ, et al. Optimal Route for Human Umbilical Cord Blood-Derived Mesenchymal Stem Cell Transplantation to Protect Against Neonatal Hyperoxic Lung Injury: Gene Expression Profiles and Histopathology. PLoS One 2015;10(8):e0135574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Doorn J, Moll G, Le Blanc K, van Blitterswijk C, de Boer J. Therapeutic applications of mesenchymal stromal cells: paracrine effects and potential improvements. Tissue Eng Part B Rev 2012. Apr;18(2):101–15. [DOI] [PubMed] [Google Scholar]
- 57.Park WS, Ahn SY, Sung SI, Ahn JY, Chang YS. Strategies to enhance paracrine potency of transplanted mesenchymal stem cells in intractable neonatal disorders. Pediatr Res 2018. Jan;83(1–2):214–22. [DOI] [PubMed] [Google Scholar]
- 58.Karantalis V, DiFede DL, Gerstenblith G, Pham S, Symes J, Zambrano JP, et al. Autologous mesenchymal stem cells produce concordant improvements in regional function, tissue perfusion, and fibrotic burden when administered to patients undergoing coronary artery bypass grafting: The Prospective Randomized Study of Mesenchymal Stem Cell Therapy in Patients Undergoing Cardiac Surgery (PROMETHEUS) trial. Circulation research 2014. Apr 11;114(8):1302–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Wehman B, Sharma S, Pietris N, Mishra R, Siddiqui OT, Bigham G, et al. Mesenchymal stem cells preserve neonatal right ventricular function in a porcine model of pressure overload. Am J Physiol Heart Circ Physiol 2016. Jun 1;310(11):H1816–26. [DOI] [PubMed] [Google Scholar]
- 60.Hatzistergos KE, Williams AR, Dykxhoorn D, Bellio MA, Yu W, Hare JM. Tumor Suppressors RB1 and CDKN2a Cooperatively Regulate Cell-Cycle Progression and Differentiation During Cardiomyocyte Development and Repair. Circulation research 2019. Apr 12;124(8):1184–97. [DOI] [PubMed] [Google Scholar]
- 61.Shabbir A, Cox A, Rodriguez-Menocal L, Salgado M, Van Badiavas E. Mesenchymal Stem Cell Exosomes Induce Proliferation and Migration of Normal and Chronic Wound Fibroblasts, and Enhance Angiogenesis In Vitro. Stem Cells Dev 2015. Jul 15;24(14):1635–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Vrijsen KR, Maring JA, Chamuleau SA, Verhage V, Mol EA, Deddens JC, et al. Exosomes from Cardiomyocyte Progenitor Cells and Mesenchymal Stem Cells Stimulate Angiogenesis Via EMMPRIN. Adv Healthc Mater 2016. Oct;5(19):2555–65. [DOI] [PubMed] [Google Scholar]
- 63.Yao Y, Huang J, Geng Y, Qian H, Wang F, Liu X, et al. Paracrine action of mesenchymal stem cells revealed by single cell gene profiling in infarcted murine hearts. PLoS One 2015;10(6):e0129164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Mayourian J, Cashman TJ, Ceholski DK, Johnson BV, Sachs D, Kaji DA, et al. Experimental and Computational Insight Into Human Mesenchymal Stem Cell Paracrine Signaling and Heterocellular Coupling Effects on Cardiac Contractility and Arrhythmogenicity. Circ Res 2017. Aug 4;121(4):411–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Bagno L, Hatzistergos KE, Balkan W, Hare JM. Mesenchymal Stem Cell-Based Therapy for Cardiovascular Disease: Progress and Challenges. Mol Ther 2018. Jul 5;26(7):1610–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Paliwal S, Chaudhuri R, Agrawal A, Mohanty S. Regenerative abilities of mesenchymal stem cells through mitochondrial transfer. J Biomed Sci 2018. Mar 30;25(1):31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Ahmad T, Mukherjee S, Pattnaik B, Kumar M, Singh S, Kumar M, et al. Miro1 regulates intercellular mitochondrial transport & enhances mesenchymal stem cell rescue efficacy. EMBO J 2014. May 2;33(9):994–1010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Zhang Y, Yu Z, Jiang D, Liang X, Liao S, Zhang Z, et al. iPSC-MSCs with High Intrinsic MIRO1 and Sensitivity to TNF-alpha Yield Efficacious Mitochondrial Transfer to Rescue Anthracycline-Induced Cardiomyopathy. Stem Cell Reports 2016. Oct 11;7(4):749–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Mahrouf-Yorgov M, Augeul L, Da Silva CC, Jourdan M, Rigolet M, Manin S, et al. Mesenchymal stem cells sense mitochondria released from damaged cells as danger signals to activate their rescue properties. Cell Death Differ 2017. Jul;24(7):1224–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Han H, Hu J, Yan Q, Zhu J, Zhu Z, Chen Y, et al. Bone marrow-derived mesenchymal stem cells rescue injured H9c2 cells via transferring intact mitochondria through tunneling nanotubes in an in vitro simulated ischemia/reperfusion model. Mol Med Rep 2016. Feb;13(2):1517–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Zhu H, Yu B, Yang L. Exogenous and Endogenous Stem Cells for Skeletal Regeneration. Stem Cells Int 2018;2018:2574243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Raicevic G, Najar M, Najimi M, El Taghdouini A, van Grunsven LA, Sokal E, et al. Influence of inflammation on the immunological profile of adult-derived human liver mesenchymal stromal cells and stellate cells. Cytotherapy 2015. Feb;17(2):174–85. [DOI] [PubMed] [Google Scholar]
- 73.Berglund AK, Fortier LA, Antczak DF, Schnabel LV. Immunoprivileged no more: measuring the immunogenicity of allogeneic adult mesenchymal stem cells. Stem Cell Res Ther 2017. Dec 22;8(1):288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Golpanian S, Wolf A, Hatzistergos KE, Hare JM. Rebuilding the Damaged Heart: Mesenchymal Stem Cells, Cell-Based Therapy, and Engineered Heart Tissue. Physiol Rev 2016. Jul;96(3):1127–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Hare JM, DiFede DL, Rieger AC, Florea V, Landin AM, El-Khorazaty J, et al. Randomized Comparison of Allogeneic Versus Autologous Mesenchymal Stem Cells for Nonischemic Dilated Cardiomyopathy: POSEIDON-DCM Trial. Journal of the American College of Cardiology 2017. Feb 07;69(5):526–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Caplan H, Olson SD, Kumar A, George M, Prabhakara KS, Wenzel P, et al. Mesenchymal Stromal Cell Therapeutic Delivery: Translational Challenges to Clinical Application. Front Immunol 2019;10:1645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Guo J, Lin GS, Bao CY, Hu ZM, Hu MY. Anti-inflammation role for mesenchymal stem cells transplantation in myocardial infarction. Inflammation 2007. Aug;30(3–4):97–104. [DOI] [PubMed] [Google Scholar]
- 78.Ohnishi S, Yanagawa B, Tanaka K, Miyahara Y, Obata H, Kataoka M, et al. Transplantation of mesenchymal stem cells attenuates myocardial injury and dysfunction in a rat model of acute myocarditis. J Mol Cell Cardiol 2007. Jan;42(1):88–97. [DOI] [PubMed] [Google Scholar]
- 79.Lee RH, Yu JM, Foskett AM, Peltier G, Reneau JC, Bazhanov N, et al. TSG-6 as a biomarker to predict efficacy of human mesenchymal stem/progenitor cells (hMSCs) in modulating sterile inflammation in vivo. Proc Natl Acad Sci U S A 2014. Nov 25;111(47):16766–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Hamidian Jahromi S, Estrada C, Li Y, Cheng E, Davies JE. Human Umbilical Cord Perivascular Cells and Human Bone Marrow Mesenchymal Stromal Cells Transplanted Intramuscularly Respond to a Distant Source of Inflammation. Stem Cells Dev 2018. Mar 15;27(6):415–29. [DOI] [PubMed] [Google Scholar]
- 81.Zhang L, Dang RJ, Li H, Li P, Yang YM, Guo XM, et al. SOCS1 regulates the immune modulatory properties of mesenchymal stem cells by inhibiting nitric oxide production. PLoS One 2014;9(5):e97256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Chen L, Zhang Y, Tao L, Yang Z, Wang L. Mesenchymal Stem Cells with eNOS Over-Expression Enhance Cardiac Repair in Rats with Myocardial Infarction. Cardiovasc Drugs Ther 2017. Feb;31(1):9–18. [DOI] [PubMed] [Google Scholar]
- 83.Maria ATJ, Rozier P, Fonteneau G, Sutra T, Maumus M, Toupet K, et al. iNOS Activity Is Required for the Therapeutic Effect of Mesenchymal Stem Cells in Experimental Systemic Sclerosis. Front Immunol 2018;9:3056. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Guo Y, Yu Y, Hu S, Chen Y, Shen Z. The therapeutic potential of mesenchymal stem cells for cardiovascular diseases. Cell Death Dis 2020. May 11;11(5):349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Golpanian S, DiFede DL, Khan A, Schulman IH, Landin AM, Tompkins BA, et al. Allogeneic Human Mesenchymal Stem Cell Infusions for Aging Frailty. The journals of gerontology Series A, Biological sciences and medical sciences 2017. Oct 12;72(11):1505–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Florea V, Rieger AC, DiFede DL, El-Khorazaty J, Natsumeda M, Banerjee MN, et al. Dose Comparison Study of Allogeneic Mesenchymal Stem Cells in Patients With Ischemic Cardiomyopathy (The TRIDENT Study). Circulation research 2017. Nov 10;121(11):1279–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Khodayari S, Khodayari H, Amiri AZ, Eslami M, Farhud D, Hescheler J, et al. Inflammatory Microenvironment of Acute Myocardial Infarction Prevents Regeneration of Heart with Stem Cells Therapy. Cell Physiol Biochem 2019;53(5):887–909. [DOI] [PubMed] [Google Scholar]
- 88.Waterman RS, Tomchuck SL, Henkle SL, Betancourt AM. A new mesenchymal stem cell (MSC) paradigm: polarization into a pro-inflammatory MSC1 or an Immunosuppressive MSC2 phenotype. PLoS One 2010. Apr 26;5(4):e10088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Deng D, Zhang P, Guo Y, Lim TO. A randomised double-blind, placebo-controlled trial of allogeneic umbilical cord-derived mesenchymal stem cell for lupus nephritis. Ann Rheum Dis 2017. Aug;76(8):1436–39. [DOI] [PubMed] [Google Scholar]
- 90.Garcia-Olmo D, Schwartz DA. Cumulative Evidence That Mesenchymal Stem Cells Promote Healing of Perianal Fistulas of Patients With Crohn’s Disease--Going From Bench to Bedside. Gastroenterology 2015. Oct;149(4):853–7. [DOI] [PubMed] [Google Scholar]
- 91.Zha S, Tay JC, Zhu S, Li Z, Du Z, Wang S. Generation of Mesenchymal Stromal Cells with Low Immunogenicity from Human PBMC-Derived beta2 Microglobulin Knockout Induced Pluripotent Stem Cells. Cell Transplant 2020. Jan-Dec;29:963689720965529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Meng X, Zheng M, Yu M, Bai W, Zuo L, Bu X, et al. Transplantation of CRISPRa system engineered IL10-overexpressing bone marrow-derived mesenchymal stem cells for the treatment of myocardial infarction in diabetic mice. J Biol Eng 2019;13:49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Nitzsche F, Muller C, Lukomska B, Jolkkonen J, Deten A, Boltze J. Concise Review: MSC Adhesion Cascade-Insights into Homing and Transendothelial Migration. Stem Cells 2017. Jun;35(6):1446–60. [DOI] [PubMed] [Google Scholar]
- 94.Madl CM, Heilshorn SC, Blau HM. Bioengineering strategies to accelerate stem cell therapeutics. Nature 2018. May;557(7705):335–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Hu X, Yu SP, Fraser JL, Lu Z, Ogle ME, Wang JA, et al. Transplantation of hypoxia-preconditioned mesenchymal stem cells improves infarcted heart function via enhanced survival of implanted cells and angiogenesis. J Thorac Cardiovasc Surg 2008. Apr;135(4):799–808. [DOI] [PubMed] [Google Scholar]
- 96.Wu Z, Chen G, Zhang J, Hua Y, Li J, Liu B, et al. Treatment of Myocardial Infarction with Gene-modified Mesenchymal Stem Cells in a Small Molecular Hydrogel. Sci Rep 2017. Nov 20;7(1):15826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Levy O, Kuai R, Siren EMJ, Bhere D, Milton Y, Nissar N, et al. Shattering barriers toward clinically meaningful MSC therapies. Sci Adv 2020. Jul;6(30):eaba6884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Park SJ, Kim RY, Park BW, Lee S, Choi SW, Park JH, et al. Dual stem cell therapy synergistically improves cardiac function and vascular regeneration following myocardial infarction. Nat Commun 2019. Jul 16;10(1):3123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Golchin A, Shams F, Karami F. Advancing Mesenchymal Stem Cell Therapy with CRISPR/Cas9 for Clinical Trial Studies. Adv Exp Med Biol 2020;1247:89–100. [DOI] [PubMed] [Google Scholar]
- 100.Tilokee EL, Latham N, Jackson R, Mayfield AE, Ye B, Mount S, et al. Paracrine Engineering of Human Explant-Derived Cardiac Stem Cells to Over-Express Stromal-Cell Derived Factor 1alpha Enhances Myocardial Repair. Stem Cells 2016. Jul;34(7):1826–35. [DOI] [PubMed] [Google Scholar]
- 101.Kulandavelu S, Balkan W, Hare JM. Next-Generation Stem Cell Therapy: Genetically Modified Mesenchymal Stem Cells for Cardiac Repair : Editorial to: “Mesenchymal Stem Cells with eNOS Over-Expression Enhance Cardiac Repair in Rats with Myocardial Infarction” by Leilei Chen et al et al. Cardiovasc Drugs Ther 2017. Feb;31(1):5–7. [DOI] [PubMed] [Google Scholar]
- 102.Vishnubalaji R, Elango R, Al-Toub M, Manikandan M, Al-Rikabi A, Harkness L, et al. Neoplastic Transformation of Human Mesenchymal Stromal Cells Mediated via LIN28B. Sci Rep 2019. May 30;9(1):8101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Lacerda L, Debeb BG, Smith D, Larson R, Solley T, Xu W, et al. Mesenchymal stem cells mediate the clinical phenotype of inflammatory breast cancer in a preclinical model. Breast Cancer Res 2015. Mar 20;17:42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Guess AJ, Daneault B, Wang R, Bradbury H, La Perle KMD, Fitch J, et al. Safety Profile of Good Manufacturing Practice Manufactured Interferon gamma-Primed Mesenchymal Stem/Stromal Cells for Clinical Trials. Stem Cells Transl Med 2017. Oct;6(10):1868–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Niess H, von Einem JC, Thomas MN, Michl M, Angele MK, Huss R, et al. Treatment of advanced gastrointestinal tumors with genetically modified autologous mesenchymal stromal cells (TREAT-ME1): study protocol of a phase I/II clinical trial. BMC Cancer 2015. Apr 8;15:237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Ouyang X, Wang X, Kraatz HB, Ahmadi S, Gao J, Lv Y, et al. A Trojan horse biomimetic delivery strategy using mesenchymal stem cells for PDT/PTT therapy against lung melanoma metastasis. Biomater Sci 2020. Feb 21;8(4):1160–70. [DOI] [PubMed] [Google Scholar]
- 107.Niess H, Thomas MN, Schiergens TS, Kleespies A, Jauch KW, Bruns C, et al. Genetic engineering of mesenchymal stromal cells for cancer therapy: turning partners in crime into Trojan horses. Innov Surg Sci 2016. Sep;1(1):19–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Moll G, Ankrum JA, Kamhieh-Milz J, Bieback K, Ringden O, Volk HD, et al. Intravascular Mesenchymal Stromal/Stem Cell Therapy Product Diversification: Time for New Clinical Guidelines. Trends Mol Med 2019. Feb;25(2):149–63. [DOI] [PubMed] [Google Scholar]
- 109.Vu Q, Xie K, Eckert M, Zhao W, Cramer SC. Meta-analysis of preclinical studies of mesenchymal stromal cells for ischemic stroke. Neurology 2014. Apr 8;82(14):1277–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Terashvili M, Bosnjak ZJ. Stem Cell Therapies in Cardiovascular Disease. J Cardiothorac Vasc Anesth 2019. Jan;33(1):209–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111.Schuleri KH, Amado LC, Boyle AJ, Centola M, Saliaris AP, Gutman MR, et al. Early improvement in cardiac tissue perfusion due to mesenchymal stem cells. Am J Physiol Heart Circ Physiol 2008. May;294(5):H2002–11. [DOI] [PubMed] [Google Scholar]
- 112.Hatzistergos KE, Quevedo H, Oskouei BN, Hu Q, Feigenbaum GS, Margitich IS, et al. Bone marrow mesenchymal stem cells stimulate cardiac stem cell proliferation and differentiation. Circ Res 2010. Oct 1;107(7):913–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Rodrigo SF, van Ramshorst J, Hoogslag GE, Boden H, Velders MA, Cannegieter SC, et al. Intramyocardial injection of autologous bone marrow-derived ex vivo expanded mesenchymal stem cells in acute myocardial infarction patients is feasible and safe up to 5 years of follow-up. J Cardiovasc Transl Res 2013. Oct;6(5):816–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Guo Y, Peng Y, Zeng H, Chen G. Progress in Mesenchymal Stem Cell Therapy for Ischemic Stroke. Stem Cells Int 2021;2021:9923566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Ding DC, Shyu WC, Chiang MF, Lin SZ, Chang YC, Wang HJ, et al. Enhancement of neuroplasticity through upregulation of beta1-integrin in human umbilical cord-derived stromal cell implanted stroke model. Neurobiol Dis 2007. Sep;27(3):339–53. [DOI] [PubMed] [Google Scholar]
- 116.Guo ZY, Sun X, Xu XL, Zhao Q, Peng J, Wang Y. Human umbilical cord mesenchymal stem cells promote peripheral nerve repair via paracrine mechanisms. Neural Regen Res 2015. Apr;10(4):651–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Zhang Y, Chopp M, Liu XS, Katakowski M, Wang X, Tian X, et al. Exosomes Derived from Mesenchymal Stromal Cells Promote Axonal Growth of Cortical Neurons. Mol Neurobiol 2017. May;54(4):2659–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Elia CA, Tamborini M, Rasile M, Desiato G, Marchetti S, Swuec P, et al. Intracerebral Injection of Extracellular Vesicles from Mesenchymal Stem Cells Exerts Reduced Abeta Plaque Burden in Early Stages of a Preclinical Model of Alzheimer’s Disease. Cells 2019. Sep 10;8(9). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Bodart-Santos V, de Carvalho LRP, de Godoy MA, Batista AF, Saraiva LM, Lima LG, et al. Extracellular vesicles derived from human Wharton’s jelly mesenchymal stem cells protect hippocampal neurons from oxidative stress and synapse damage induced by amyloid-beta oligomers. Stem Cell Res Ther 2019. Nov 20;10(1):332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.de Godoy MA, Saraiva LM, de Carvalho LRP, Vasconcelos-Dos-Santos A, Beiral HJV, Ramos AB, et al. Mesenchymal stem cells and cell-derived extracellular vesicles protect hippocampal neurons from oxidative stress and synapse damage induced by amyloid-beta oligomers. J Biol Chem 2018. Feb 9;293(6):1957–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Cui GH, Wu J, Mou FF, Xie WH, Wang FB, Wang QL, et al. Exosomes derived from hypoxia-preconditioned mesenchymal stromal cells ameliorate cognitive decline by rescuing synaptic dysfunction and regulating inflammatory responses in APP/PS1 mice. FASEB J 2018. Feb;32(2):654–68. [DOI] [PubMed] [Google Scholar]
- 122.Xin H, Li Y, Liu Z, Wang X, Shang X, Cui Y, et al. MiR-133b promotes neural plasticity and functional recovery after treatment of stroke with multipotent mesenchymal stromal cells in rats via transfer of exosome-enriched extracellular particles. Stem Cells 2013. Dec;31(12):2737–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Zhou J, Wang Y, Liu Y, Zeng H, Xu H, Lian F. Adipose derived mesenchymal stem cells alleviated osteoarthritis and chondrocyte apoptosis through autophagy inducing. J Cell Biochem 2018. Oct 13. [DOI] [PubMed] [Google Scholar]
- 124.Toghraie F, Razmkhah M, Gholipour MA, Faghih Z, Chenari N, Torabi Nezhad S, et al. Scaffold-free adipose-derived stem cells (ASCs) improve experimentally induced osteoarthritis in rabbits. Arch Iran Med 2012. Aug;15(8):495–9. [PubMed] [Google Scholar]
- 125.Chahal J, Gomez-Aristizabal A, Shestopaloff K, Bhatt S, Chaboureau A, Fazio A, et al. Bone Marrow Mesenchymal Stromal Cell Treatment in Patients with Osteoarthritis Results in Overall Improvement in Pain and Symptoms and Reduces Synovial Inflammation. Stem Cells Transl Med 2019. Aug;8(8):746–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Jo CH, Chai JW, Jeong EC, Oh S, Shin JS, Shim H, et al. Intra-articular Injection of Mesenchymal Stem Cells for the Treatment of Osteoarthritis of the Knee: A 2-Year Follow-up Study. Am J Sports Med 2017. Oct;45(12):2774–83. [DOI] [PubMed] [Google Scholar]
- 127.Freitas GP, Lopes HB, Souza ATP, Oliveira P, Almeida ALG, Souza LEB, et al. Cell Therapy: Effect of Locally Injected Mesenchymal Stromal Cells Derived from Bone Marrow or Adipose Tissue on Bone Regeneration of Rat Calvarial Defects. Sci Rep 2019. Sep 17;9(1):13476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Kim SJ, Shin YW, Yang KH, Kim SB, Yoo MJ, Han SK, et al. A multi-center, randomized, clinical study to compare the effect and safety of autologous cultured osteoblast(Ossron) injection to treat fractures. BMC Musculoskelet Disord 2009. Feb 12;10:20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Yang Y, Pan Q, Zou K, Wang H, Zhang X, Yang Z, et al. Administration of allogeneic mesenchymal stem cells in lengthening phase accelerates early bone consolidation in rat distraction osteogenesis model. Stem Cell Res Ther 2020. Mar 20;11(1):129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Desando G, Cavallo C, Sartoni F, Martini L, Parrilli A, Veronesi F, et al. Intra-articular delivery of adipose derived stromal cells attenuates osteoarthritis progression in an experimental rabbit model. Arthritis Res Ther 2013. Jan 29;15(1):R22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Zhang QZ, Su WR, Shi SH, Wilder-Smith P, Xiang AP, Wong A, et al. Human gingiva-derived mesenchymal stem cells elicit polarization of m2 macrophages and enhance cutaneous wound healing. Stem Cells 2010. Oct;28(10):1856–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Satue M, Schuler C, Ginner N, Erben RG. Intra-articularly injected mesenchymal stem cells promote cartilage regeneration, but do not permanently engraft in distant organs. Sci Rep 2019. Jul 12;9(1):10153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Migliorini F, Tingart M, Maffulli N. Progress with stem cell therapies for tendon tissue regeneration. Expert Opin Biol Ther 2020. Nov;20(11):1373–79. [DOI] [PubMed] [Google Scholar]
- 134.Lee SY, Kim W, Lim C, Chung SG. Treatment of Lateral Epicondylosis by Using Allogeneic Adipose-Derived Mesenchymal Stem Cells: A Pilot Study. Stem Cells 2015. Oct;33(10):2995–3005. [DOI] [PubMed] [Google Scholar]
- 135.Hurd JL, Facile TR, Weiss J, Hayes M, Hayes M, Furia JP, et al. Safety and efficacy of treating symptomatic, partial-thickness rotator cuff tears with fresh, uncultured, unmodified, autologous adipose-derived regenerative cells (UA-ADRCs) isolated at the point of care: a prospective, randomized, controlled first-in-human pilot study. J Orthop Surg Res 2020. Mar 30;15(1):122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136.Magne B, Lataillade JJ, Trouillas M. Mesenchymal Stromal Cell Preconditioning: The Next Step Toward a Customized Treatment For Severe Burn. Stem Cells Dev 2018. Oct 15;27(20):1385–405. [DOI] [PubMed] [Google Scholar]
- 137.Falanga V, Iwamoto S, Chartier M, Yufit T, Butmarc J, Kouttab N, et al. Autologous bone marrow-derived cultured mesenchymal stem cells delivered in a fibrin spray accelerate healing in murine and human cutaneous wounds. Tissue Eng 2007. Jun;13(6):1299–312. [DOI] [PubMed] [Google Scholar]
- 138.Zhou Y, Zhao B, Zhang XL, Lu YJ, Lu ST, Cheng J, et al. Combined topical and systemic administration with human adipose-derived mesenchymal stem cells (hADSC) and hADSC-derived exosomes markedly promoted cutaneous wound healing and regeneration. Stem Cell Res Ther 2021. May 1;12(1):257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Hu P, Yang Q, Wang Q, Shi C, Wang D, Armato U, et al. Mesenchymal stromal cells-exosomes: a promising cell-free therapeutic tool for wound healing and cutaneous regeneration. Burns Trauma 2019;7:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Hyldig K, Riis S, Pennisi CP, Zachar V, Fink T. Implications of Extracellular Matrix Production by Adipose Tissue-Derived Stem Cells for Development of Wound Healing Therapies. Int J Mol Sci 2017. May 31;18(6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Lo Sicco C, Reverberi D, Balbi C, Ulivi V, Principi E, Pascucci L, et al. Mesenchymal Stem Cell-Derived Extracellular Vesicles as Mediators of Anti-Inflammatory Effects: Endorsement of Macrophage Polarization. Stem Cells Transl Med 2017. Mar;6(3):1018–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Lozito TP, Jackson WM, Nesti LJ, Tuan RS. Human mesenchymal stem cells generate a distinct pericellular zone of MMP activities via binding of MMPs and secretion of high levels of TIMPs. Matrix Biol 2014. Feb;34:132–43. [DOI] [PubMed] [Google Scholar]
- 143.Czarnecka A, Odziomek A, Murzyn M, Dubis J, Baglaj-Oleszczuk M, Hryncewicz-Gwozdz A. Wharton’s jelly-derived mesenchymal stem cells in the treatment of four patients with alopecia areata. Adv Clin Exp Med 2021. Feb;30(2):211–18. [DOI] [PubMed] [Google Scholar]
- 144.Gentile P, Scioli MG, Bielli A, Orlandi A, Cervelli V. Stem cells from human hair follicles: first mechanical isolation for immediate autologous clinical use in androgenetic alopecia and hair loss. Stem Cell Investig 2017;4:58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Gentile P, Scioli MG, Cervelli V, Orlandi A, Garcovich S. Autologous Micrografts from Scalp Tissue: Trichoscopic and Long-Term Clinical Evaluation in Male and Female Androgenetic Alopecia. Biomed Res Int 2020;2020:7397162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Srifa W, Kosaric N, Amorin A, Jadi O, Park Y, Mantri S, et al. Cas9-AAV6-engineered human mesenchymal stromal cells improved cutaneous wound healing in diabetic mice. Nat Commun 2020. May 18;11(1):2470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Meng ZW, Baumgart DC. Darvadstrocel for the treatment of perianal fistulas in Crohn’s disease. Expert Rev Gastroenterol Hepatol 2020. Jun;14(6):405–10. [DOI] [PubMed] [Google Scholar]
- 148.Tompkins BA, DiFede DL, Khan A, Landin AM, Schulman IH, Pujol MV, et al. Allogeneic Mesenchymal Stem Cells Ameliorate Aging Frailty: A Phase II Randomized, Double-Blind, Placebo-Controlled Clinical Trial. The journals of gerontology Series A, Biological sciences and medical sciences 2017. Oct 12;72(11):1513–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Walston J, Robinson TN, Zieman S, McFarland F, Carpenter CR, Althoff KN, et al. Integrating Frailty Research into the Medical Specialties-Report from a U13 Conference. J Am Geriatr Soc 2017. Oct;65(10):2134–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Florea V, Bagno L, Rieger AC, Hare JM. Attenuation of frailty in older adults with mesenchymal stem cells. Mech Ageing Dev 2019. Jul;181:47–58. [DOI] [PubMed] [Google Scholar]
- 151.Pahor M, Kritchevsky SB, Waters DL, Villareal DT, Morley J, Hare JM, et al. Designing Drug Trials for Frailty: ICFSR Task Force 2018. J Frailty Aging 2018;7(3):150–54. [DOI] [PubMed] [Google Scholar]
- 152.Schulman IH, Balkan W, Hare JM. Mesenchymal Stem Cell Therapy for Aging Frailty. Front Nutr 2018;5:108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Oliva AA, McClain-Moss L, Pena A, Drouillard A, Hare JM. Allogeneic mesenchymal stem cell therapy: A regenerative medicine approach to geroscience. Aging Med (Milton) 2019. Sep;2(3):142–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Durand N, Mallea J, Zubair AC. Insights into the use of mesenchymal stem cells in COVID-19 mediated acute respiratory failure. NPJ Regen Med 2020. Oct 26;5(1):17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 155.Qu W, Wang Z, Hare JM, Bu G, Mallea JM, Pascual JM, et al. Cell-based therapy to reduce mortality from COVID-19: Systematic review and meta-analysis of human studies on acute respiratory distress syndrome. Stem Cells Transl Med 2020. Sep;9(9):1007–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Tao J, Nie Y, Wu H, Cheng L, Qiu Y, Fu J, et al. Umbilical cord blood-derived mesenchymal stem cells in treating a critically ill COVID-19 patient. J Infect Dev Ctries 2020. Oct 31;14(10):1138–45. [DOI] [PubMed] [Google Scholar]
- 157.Liang B, Chen J, Li T, Wu H, Yang W, Li Y, et al. Clinical remission of a critically ill COVID-19 patient treated by human umbilical cord mesenchymal stem cells: A case report. Medicine (Baltimore) 2020. Jul 31;99(31):e21429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 158.Yilmaz R, Adas G, Cukurova Z, Kart Yasar K, Isiksacan N, Oztel ON, et al. Mesenchymal stem cells treatment in COVID-19 patient with multi-organ involvement. Bratisl Lek Listy 2020;121(12):847–52. [DOI] [PubMed] [Google Scholar]
- 159.Leng Z, Zhu R, Hou W, Feng Y, Yang Y, Han Q, et al. Transplantation of ACE2(−) Mesenchymal Stem Cells Improves the Outcome of Patients with COVID-19 Pneumonia. Aging Dis 2020. Apr;11(2):216–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Gentile P, Sterodimas A. Adipose Stem Cells (ASCs) and Stromal Vascular Fraction (SVF) as a Potential Therapy in Combating (COVID-19)-Disease. Aging Dis 2020. May;11(3):465–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.Gentile P, Sterodimas A, Pizzicannella J, Calabrese C, Garcovich S. Research progress on Mesenchymal Stem Cells (MSCs), Adipose-Derived Mesenchymal Stem Cells (AD-MSCs), Drugs, and Vaccines in Inhibiting COVID-19 Disease. Aging Dis 2020. Oct;11(5):1191–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Gentile P SARS-CoV-2: the “Uncensored” Truth about Its Origin and Adipose-Derived Mesenchymal Stem Cells as New Potential Immune-Modulatory Weapon. Aging Dis 2021. Apr;12(2):330–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Zhang Y, Ding J, Ren S, Wang W, Yang Y, Li S, et al. Intravenous infusion of human umbilical cord Wharton’s jelly-derived mesenchymal stem cells as a potential treatment for patients with COVID-19 pneumonia. Stem Cell Res Ther 2020. May 27;11(1):207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Pan BT, Teng K, Wu C, Adam M, Johnstone RM. Electron microscopic evidence for externalization of the transferrin receptor in vesicular form in sheep reticulocytes. J Cell Biol 1985. Sep;101(3):942–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Plotnikov EY, Khryapenkova TG, Vasileva AK, Marey MV, Galkina SI, Isaev NK, et al. Cell-to-cell cross-talk between mesenchymal stem cells and cardiomyocytes in co-culture. J Cell Mol Med 2008. Sep-Oct;12(5A):1622–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 166.Franco da Cunha F, Andrade-Oliveira V, Candido de Almeida D, Borges da Silva T, Naffah de Souza Breda C, Costa Cruz M, et al. Extracellular Vesicles isolated from Mesenchymal Stromal Cells Modulate CD4(+) T Lymphocytes Toward a Regulatory Profile. Cells 2020. Apr 23;9(4). [DOI] [PMC free article] [PubMed] [Google Scholar]