

Abstract
Background
Hirsutism is a distressing and relatively common endocrine problem in women which may prove difficult to manage. Cyproterone acetate, an anti‐androgen, is frequently used to treat hirsutism, usually in combination with ethinyl estradiol.
Objectives
The objective of this review was to investigate the effectiveness of cyproterone acetate alone, or in combination with ethinyl estradiol, in reducing hair growth in women with hirsutism secondary to ovarian hyperandrogenism.
Search methods
The Cochrane Menstrual Disorders and Subfertility Group trials register was searched (last search ‐ 4 June 2002). The Cochrane Menstrual Disorders and Subfertility Group register is based on regular searches of MEDLINE (1966 to 2002), EMBASE (1980 to 2002), CINAHL (1982 to 2002), PsycINFO (1987 to 2002) and CENTRAL (Issue 2, 2002 of the Cochrane Library) the handsearching of several journals and conference proceedings, and searches of several key grey literature sources. All publications of randomised controlled trials of cyproterone acetate with or without estrogen versus placebo or other drug therapies for hirsutism were identified.
Selection criteria
All randomised controlled studies comparing: ‐ cyproterone acetate to placebo ‐ cyproterone acetate with ethinyl estradiol to placebo ‐ cyproterone acetate with ethinyl estradiol to cyproterone acetate alone ‐ cyproterone acetate (with or without estradiol) to other medical therapies for treatment of hirsutism.
Data collection and analysis
Eleven studies were identified which fulfilled the inclusion criteria. Nine randomised studies were included in the review, and two were excluded because of insufficient information. Only one study had more than 100 women included in the analysis. The major outcomes included: subjective improvement in hirsutism, changes in Ferriman Gallwey scores, changes in linear hair growth and hair shaft diameter, alterations in endocrine parameters, side effects to treatment, withdrawals during therapy
Main results
There were no clinical trials comparing cyproterone acetate alone with placebo. There was one small study comparing cyproterone acetate in combination with ethinyl estradiol to placebo. In this study there was a significant subjective reduction in hair growth with cyproterone acetate therapy, although the confidence limits were large. There were no studies comparing cyproterone acetate alone with cyproterone acetate in combination with ethinyl estradiol to treat hirsutism. In studies where cyproterone acetate was compared to other drug modalities (ketoconazole, spironolactone, flutamide, finasteride, GnRH analogues) no difference in clinical outcome was noted. There were, however, endocrinological differences in androgen and estrogen levels between different drug therapies. There were insufficient data to assess differences in side effects between women treated with cyproterone acetate and other medical therapy.
Authors' conclusions
Cyproterone acetate combined with estradiol results in a subjective improvement in hirsutism compared to placebo. Clinical differences in outcome between cyproterone acetate and other medical therapies were not demonstrated in the studies included in this review. This may be because of the small size of the studies, lack of standardized assessment and lack of objective determinants of improvement in hirsutism. The endocrinological effects of the different drug therapies reflect the mode of action. Larger carefully designed studies are needed to compare efficacy and safety profiles between drug therapies for hirsutism.
Keywords: Female; Humans; Androgen Antagonists; Androgen Antagonists/therapeutic use; Cyproterone Acetate; Cyproterone Acetate/therapeutic use; Drug Therapy, Combination; Ethinyl Estradiol; Ethinyl Estradiol/therapeutic use; Hirsutism; Hirsutism/drug therapy; Hirsutism/etiology; Hyperandrogenism; Hyperandrogenism/complications; Randomized Controlled Trials as Topic
Plain language summary
Cyproterone acetate appears to be as effective as other medications for hirsutism in women caused by excessive androgen production by the ovaries
One of the causes of hirsutism (excessive hair growth) in women is excessive production of the hormone androgens by the ovaries. A variety of medications can be used to counter the effects of the androgen. Cyproterone acetate is an anti‐androgen drug. Adverse effects that have been reported with its use include weight gain, depression, fatigue, breast symptoms and sexual dysfunction. The review of trials found that cyproterone acetate appears to have a similar impact on hirsutism as other drugs used for hirsutism caused by excessive androgen. There was not enough evidence to compare adverse effects of the treatment options.
Background
Hyperandrogenism (elevation of masculinizing hormones) is probably the commonest endocrine disturbance in women. The clinical manifestations of hyperandrogenism vary from mild skin changes (increased oiliness), acne, excess facial and body hair through to voice changes, enlargement of the clitoris and change in body habitus.
Hirsutism is the growth of terminal hair in sites at which it is usually considered a male secondary sexual characteristic e.g. chest and beard area. About one third of women in the reproductive years have some hair on their face, abdomen or chest (McKnight 1984). Among older women, up to 75% may have slightly increased facial hair, because the main product of the postmenopausal ovaries is androstenedione which is converted to testosterone in the peripheral tissue.
The three main naturally occurring steroids responsible for androgen action are testosterone, dehydroepiandrosterone (DHEA) and androstenedione. Testosterone is the most important androgen and conversion by five alpha‐reductase to the more potent dihydrotestosterone is necessary for its biological action (Franks 1989). Androstenedione and DHEA may be regarded as pre hormones which are converted in peripheral tissue to testosterone before they exert any androgenic influence. Production, peripheral conversion and protein binding are important determinants of androgenic effect. Total testosterone measurements, which reflect bound and free hormone do not accurately reflect tissue exposure to androgens. The derived free androgen index (testosterone x 100 divided by sex hormone binding globulin levels) may be used to give an indirect estimation of the free testosterone levels.
The distribution and quality of the hair and the concentration of androgen receptors in the skin are genetically determined, and hence the clinical effects of hyperandrogaenemia are influenced by genetic predisposition (Flamigni 1971; Mowszowicz 1981). Once five alpha‐reductase activity has been induced in a hair follicle, it remains sensitive to androgen stimulation for the rest of its life cycle. The hair cycle varies in different parts of the body ‐ from three‐six months on the face to five+ years on the scalp (Saitoh 1970; Seago 1985). As a result, therapeutic interventions result in gradual changes in the clinical presentation and the development of hirsutism itself reflects prolonged androgen stimulation.
Androgens also increase the rate of mitosis and epithelial proliferation of sebaceous gland acini and cause enhanced sebum production ‐ both these factors contribute to the development of acne (Ashton 1987; Nurnberger 1987).
Hyperandrogenism may result from ovarian and/or adrenal overproduction of androgens and/or altered peripheral metabolism and/or altered end organ sensitivity. The diagnosis in the majority of women who present with hirsutism will be the polycystic ovary syndrome which is characterised by a typical ultrasound appearance of the ovaries and a variable endocrine and clinical picture (Conway 1989; Adams 1986; Bunker 1989).
Objective scoring systems to assess hirsutism have been used in clinical practice, but these may be difficult to reproduce as there may be considerable inter‐observer variation (Ferriman 1961). Other methods of assessing hair growth include measuring the rate of hair growth with a trichometer or shaving and weighing the hair (Jones 1981). Sebum production is affected by androgens and is sometimes used as a surrogate marker for the effect of therapy on the skin. Many of these methods are impractical in current clinical practice.
Therapeutic options for the management of hirsutism have increased considerably over the past few decades.
Cyproterone acetate is an anti‐androgen with potent progestational action and in combination with ethinyl estradiol it inhibits five alpha‐reductase activity in the skin of hirsute women, increases SHBG levels and has a significant anti‐gonadotrophin effect (Neumann 1987). Cyproterone acetate is stored in adipose tissue which causes a marked depot effect when high doses are used. It has now been an accepted treatment of hirsutism for almost two decades with a reported good clinical response in sixty to eighty percent of patients (Mowszowicz 1983; Kuttenn 1980; Hammerstein 1975; Hammerstein 1983). The documented effects of cyproterone acetate on serum androgen concentrations are somewhat varied (Reed 1988; Rubens1984). Side effects of weight gain, depression, fatigue, breast symptoms and sexual dysfunction have been reported during cyproterone acetate therapy (Lunnell 1982; Appelt 1984).
Other therapeutic agents for hirsutism include spironolactone (which inhibits steroidogenesis, blocks the androgen receptor and inhibits five alpha reductase, ketoconazole (a powerful enzyme inhibitor), flutamide (a receptor blocker), finasteride (a five alpha reductase inhibitor) and GnRH agonist analogues (which cause pituitary down regulation) (van der spuy 1992).
The effectiveness of cyproterone acetate with or without estrogen therapy has not been confirmed by systematic review.
Objectives
To determine the effectiveness and safety of cyproterone acetate treatment with or without estrogen therapy in reducing hair growth in women with hirsutism by systematically reviewing randomised controlled trials.
We wished to test the following hypotheses:
1. The use of cyproterone acetate is more effective than placebo or other medical therapy in treating hirsutism.
2. The use of cyproterone acetate plus additional estrogen therapy is more effective than cyproterone acetate alone in treating hirsutism.
3. The use of cyproterone acetate in doses of greater than 2mg in combination with ethinyl estradiol is more effective than 2mg cyproterone acetate in combination with ethinyl estradiol in treating hirsutism. 4. The use of cyproterone acetate improves endocrine parameters when administered to women with hirsutism.
Methods
Criteria for considering studies for this review
Types of studies
1. All randomised controlled comparisons of cyproterone acetate therapy versus placebo. 2. All randomised controlled comparisons of cyproterone acetate therapy versus other medical therapy. 3. All randomised controlled comparisons of cyproterone acetate therapy plus estrogens vs cyproterone acetate alone to treat hirsutism will be assessed.
Types of participants
1. Women of reproductive years 2. Women requiring therapy for hirsutism measured either objectively or subjectively. 3. Women with hirsutism secondary to hyperandrogenism of ovarian origin. 4. Women with idiopathic hirsutism
Exclusion criteria: 1. Women outside reproductive years 2. Women with hirsutism secondary to a functional androgenic tumour 3. Women with iatrogenic causes of hyperandrogenism/hirsutism 4. Women with non‐endocrine causes of hyperandrogenism/hirsutism e.g. medical conditions such as porphyria.
Types of interventions
1. Cyproterone acetate therapy (with or without ethinyl estradiol) versus placebo or any other medical therapy. 2. Cyproterone acetate alone vs cyproterone acetate plus ethinyl estradiol.
Types of outcome measures
For cyproterone acetate therapy versus placebo and any other medical therapy and cyproterone acetate therapy alone versus cyproterone acetate plus ethinyl estradiol, each of the following outcome measures will be recorded where available ‐
1. Objective assessment of improvement in hirsutism a. validated scoring system ‐ Ferriman Gallwey Score b. validated measurement of hair growth ‐ hair shaft diameter, length or weight
2. Subjective assessment of improvement of hirsutism ‐ assessment by woman or medical attendant
3. Change in sebum production ‐ objectively measured
4. Improved endocrine parameters Testosterone ‐ free and total Dehydroepiandosterone (DHEA and DHEAS) Androstenedione Free androgen index Sex hormone binding globulin Cortisol Estradiol Estrone Insulin (resistance)
5. Other laboratory parameters Liver function tests Full blood count
6. Dose of cyproterone acetate
7. Acceptability and satisfaction to women, provided this is recorded in a validated format.
8. Adherence to / compliance with therapy.
9. Side effects Liver dysfunction Weight‐gain Decreased libido/sexual dysfunction Breast symptoms Depression Fatigue Menstrual cycle disruptions
10. Withdrawal from trials
Search methods for identification of studies
The Cochrane Menstrual Disorders and Subfertility Group trials register was searched (last search ‐ 4 June 2002). The Cochrane Menstrual Disorders and Subfertility Group register is based on regular searches of MEDLINE (1966 to 2002), EMBASE (1980 to 2002), CINAHL (1982 to 2002), PsycINFO (1987 to 2002) and CENTRAL (Issue 2, 2002 of the Cochrane Library) the handsearching of several journals and conference proceedings, and searches of several key grey literature sources. A full description is given in the Group's module on the Cochrane Library. All publications of randomised controlled trials of cyproterone acetate with or without estrogen versus placebo or other drug therapies for hirsutism were identified.
Data collection and analysis
Studies were excluded if they made comparisons other than those specified above. All assessments of the quality of trials and data extraction were performed unblinded by two reviewers. Selection of trials for inclusion in the review was performed together by the two reviewers (ZvdS and PleR) after employing the search strategy described previously.
If necessary, additional information was sought from the principal investigators of trials which appeared to meet the inclusion criteria. The standard check list developed by the review group was used to assess the quality of the included trial.
The quality of allocation concealment was graded either as A (adequate) B (unclear) or C (inadequate). For each included trial, information was collected regarding the method of randomisation, allocation concealment, blinding, whether an intention to treat analysis was performed and relevant interventions and outcomes. Data were extracted independently by the two reviewers using forms designed according to the Menstrual Disorders and Subfertility Group guidelines.
Statistical analyses were conducted in accordance with the guidelines developed by the Menstrual Disorders and Subfertility Group. The mean and standard deviation of measured parameters at defined time points during treatment were compared. In the case of cross‐over studies the duration prior to and after cross‐over would be included in the analysis.
Results
Description of studies
The forty five references to studies were obtained after following the Menstrual Disorders and Subfertility Group search strategy. Thirty four of these references were excluded because they did not fulfil the inclusion criteria for the review.
Eleven trials were identified which fulfilled the inclusion criteria for the review. Two trials were subsequently excluded because of lack of information regarding outcomes (Barth 1991; Belisle 1986). Nine studies were analysed in this review. Additional information was sought from two of these authors (Fruzetti 1999; Pazos 1999).
The studies were all performed in the 1990s, except one study which was performed in 1986. All nine studies analysed recruited women with hirsutism. Studies that only evaluated participants with acne and no hirsutism who were treated with cyproterone acetate were excluded. Three studies included the features or diagnosis of polycytic ovary in addition to hirsutism in their inclusion criteria (Couzinet 1986; Gokmen 1996; Saeed 1993). One author only included women where cosmetic measures had proved to be inadequate (O'Brien 1990).
All trials included cyproterone acetate as part of their intervention. Cyproterone acetate was used in combination with ethinyl estradiol in seven studies and alone in two studies. Doses of cyproterone acetate varied from 2mg (when used as the Diane/Dianette oral contraceptive preparation) up to 25‐100mg. Where only a 2mg dose of cyproterone acetate was used (as in the combined oral contraceptive Diane/ Dianette), the data was analysed separately from the groups where a dose of greater than 2mg was used. Cyproterone acetate in a dose of 2mg, combined with ethinyl estradiol, was compared to a larger dose of 100mg in addition to Diane/Dianette, given on days one‐ten of the menstrual cycle were compared by one author (Gokmen 1996). Cyproterone acetate (as a 2mg dose in combination with ethinyl estradiol) was only compared to placebo in one study.
Cyproterone acetate was compared to spironolactone in four studies (Dixon 1991; Erenus 1996; Gokmen 1996; O'Brien 1990), to flutamide in three studies (Fruzetti 1999; Grigoriou 1996; Pazos 1999)), to finasteride in one study (Fruzetti 1999), to ketoconazole in one study (Gokmen 1996) and to GnRH analogues in two studies (Couzinet 1986; Pazos 1999).
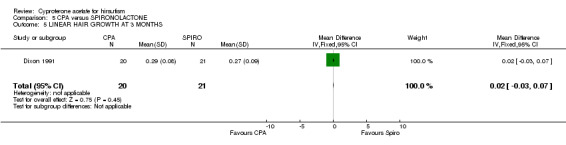
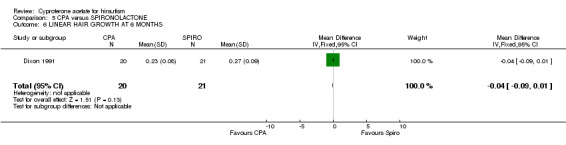
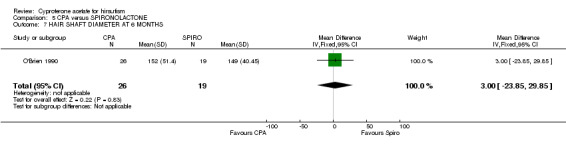
The main clinical outcome of improved hirsutism was assessed subjectively in one study (Saeed 1993), by photographic assessment to evaluate linear hair growth in one study (Dixon 1991) and hair diameter (O'Brien 1990) in another study. The other studies used the Ferriman Gallwey score to assess improvement in clinical outcome. Endocrine markers of therapy included serum levels of free and total testosterone, androstenedione, DHEAS, estradiol and SHBG. Urinary three alpha androstenediol glucuronide levels were also measured as an outcome in one study (Fruzetti 1999). None of the included studies assessed sebum production.
Risk of bias in included studies
One of the studies was rated A because the authors reported randomisation procedures adequately to control selection bias (Saeed 1993). The rest of the included studies did not report how randomisation was performed or did not document safeguard procedures and were given a quality score of B or C.
No studies included power calculations or an intention to treat analysis. Four studies did, however, describe the number of withdrawals during the study period (Fruzetti 1999; Gokmen 1996; O'Brien 1990; Pazos 1999). One study was double‐blinded (Saeed 1993) and one study had single blinding of the investigator performing the hair measurements (Erenus 1996). The rest of the studies were not blinded. One study was a cross over study after women had been randomly assigned treatment in the first instance. They crossed over to the second treatment after completing the first three months of therapy with the initial allocated therapy (Couzinet 1986). Both pre‐cross over and post‐cross over results were analysed, but a six month gap occurred between the two treatment periods. One study had a two stage randomisation procedure where women were initially randomised to receive either Diane or larger doses of cyproterone acetate and later another two other groups were added to the randomisation process where patients could also be treated with either Spironolactone or Ketoconazole (Gokmen 1996).
All trials were of adequate duration varying from 3 months to 12 months. One trial analysed 141 women (Gokmen 1996) who were divided into 4 treatment groups, and all other studies were small with less than 100 women suitable for analysis. The inclusion and exclusion criteria were clearly stated in four studies (Fruzetti 1999; Gokmen 1996; O'Brien 1990; Pazos 1999).
Effects of interventions
Hirsutism was evaluated between different treatment groups at defined time intervals (e.g. three months, six months, twelve months). The change in hirsutism from baseline in individual groups was not presented by the authors of these studies. The improvement with treatment could therefore only be assessed in comparison to other studied groups, rather than in an individual group alone over time.
CYPROTERONE ACETATE ALONE VERSUS PLACEBO There were no data available comparing cyproterone acetate alone to placebo.
CYPROTERONE ACETATE VERSUS CYPROTERONE ACETATE IN COMBINATION WITH ETHINYL ESTRADIOL There were also no data comparing cyproterone acetate alone to cyproterone acetate in combination with ethinyl estradiol.
CYPROTERONE ACETATE (2mg) COMBINED WITH ETHINYL ESTRADIOL VERSUS PLACEBO There was one study where cyproterone acetate in a dose of 2mg incorporated into an oral contraceptive (Diane) was compared to placebo (Saeed 1993). There was a subjective improvement in hirsutism (OR 45.0, 95% CI 2.01 to 1006.80), but no objective clinical assessment was performed. There were wide confidence limits in the subjective difference found and this finding may not be a reproducible indication of improvement in outcome.
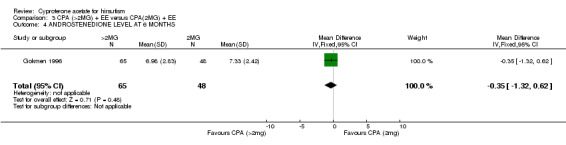
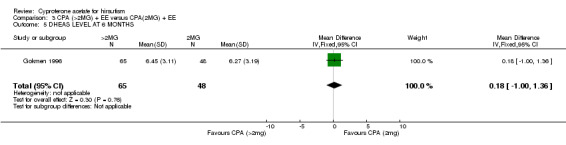
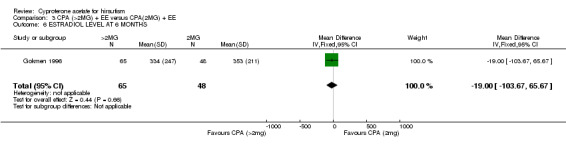
CYPROTERONE ACETATE (DOSE> 2mg) COMBINED WITH ETHINYL ESTRADIOL VERSUS CYPROTERONE ACETATE (2mg) COMBINED WITH ETHINYL ESTRADIOL When comparing cyproterone acetate in doses greater than 2mg (doses ranging from 25 to 100mg) in addition to ethinyl estradiol with the lower dose of 2mg in combination with ethinyl estradiol, there were no significant differences in the Ferriman Gallwey score or endocrine levels. Only one study was included in this analyses (Gokmen 1996) with relatively small numbers and the effect of a larger dose may be apparent in an expanded study.
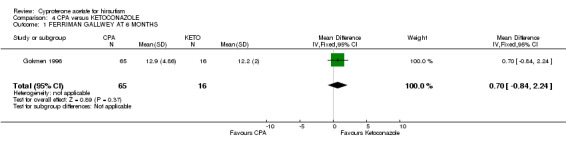
CYPROTERONE ACETATE VERSUS OTHER MEDICAL THERAPY Cyproterone acetate was then compared to other medical treatments ‐ ketoconazole (Gokmen 1996), spironolactone (O'Brien 1990; Dixon 1991; Erenus 1996; Gokmen 1996), flutamide (Pazos 1999; Fruzetti 1999; Grigoriou 1996), finasteride (Fruzetti 1999) and GnRH analogues (Pazos 1999; Couzinet 1986). There were no significant differences in clinical outcome with any of the medical therapies (other than the Ferriman Gallwey score at 12 months in the cyproterone acetate and flutamide groups favouring flutamide), but endocrine differences were observed during treatment.
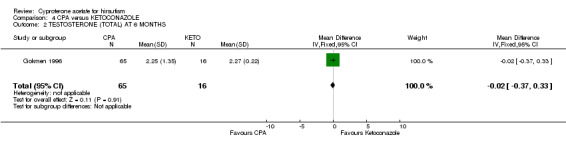
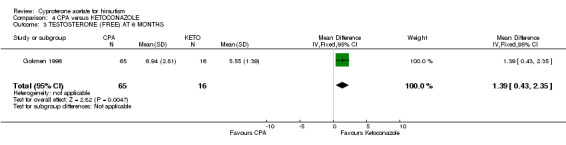
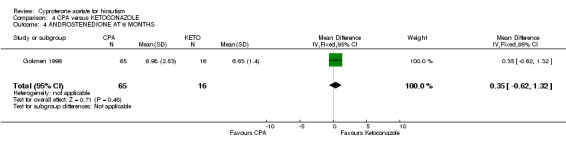
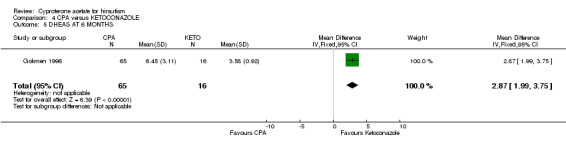
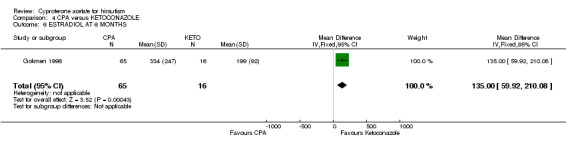
CYPROTERONE ACETATE VERSUS KETOCONAZOLE The serum free testosterone, DHEAS and estradiol levels were all significantly higher in the women treated with cyproterone acetate compared with those treated with ketoconazole. There were no differences in the total testosterone and androstenedione levels between these groups.
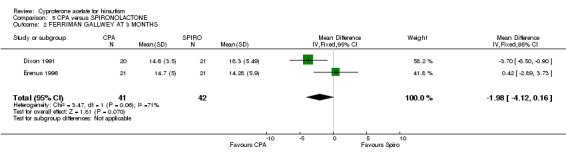
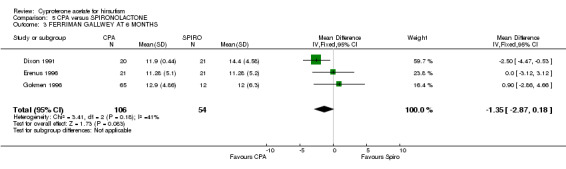
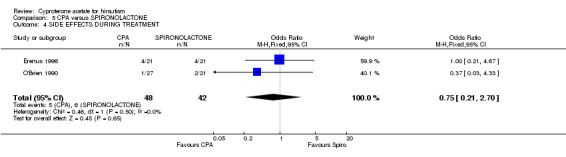
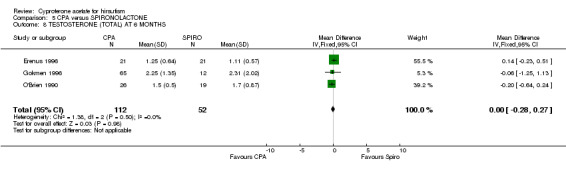
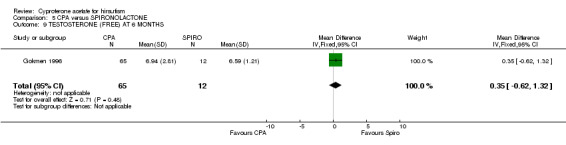
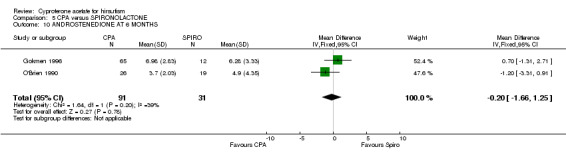
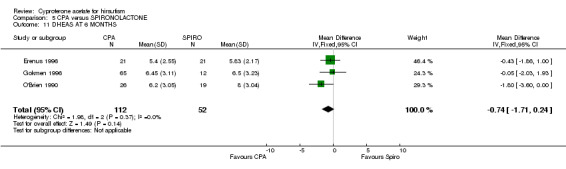
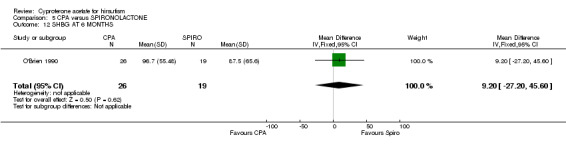
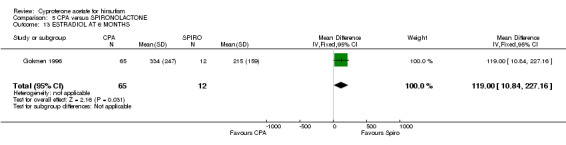
CYPROTERONE ACETATE VERSUS SPIRONOLACTONE There were no differences in serum androgens when cyproterone acetate was compared with spironolactone, but the estradiol levels were higher in the women treated with cyproterone acetate.
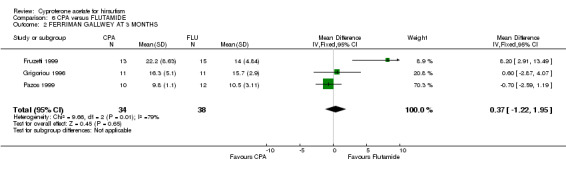
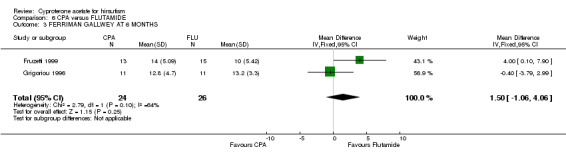
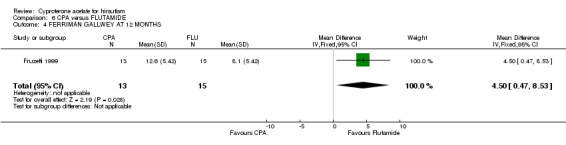
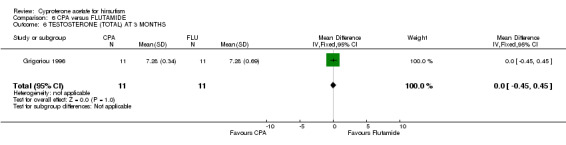
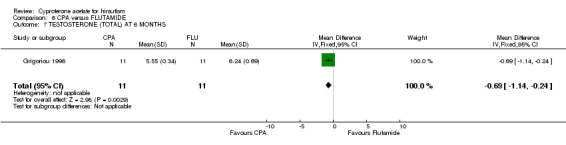
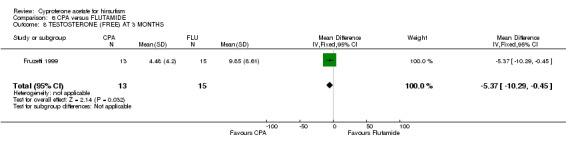
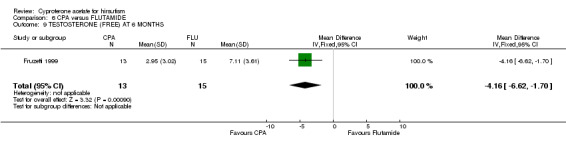
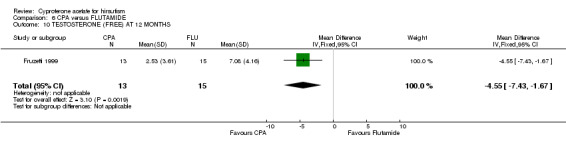
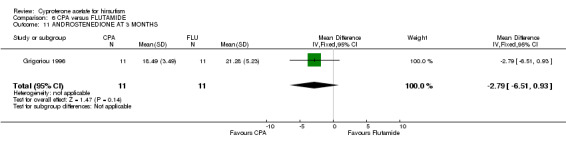
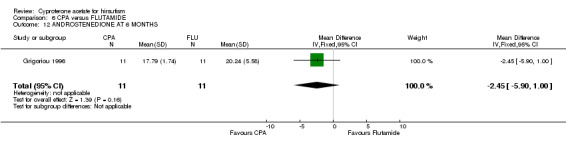
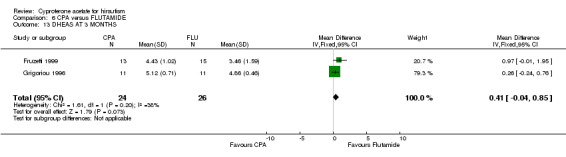
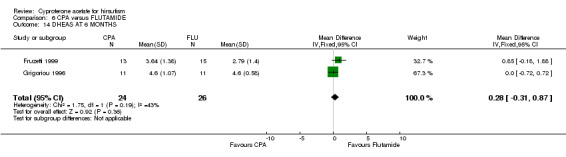
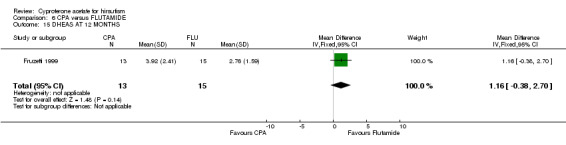
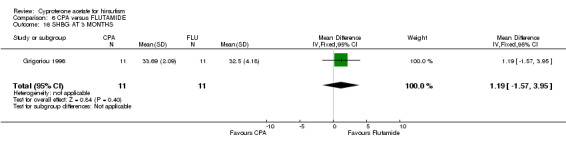
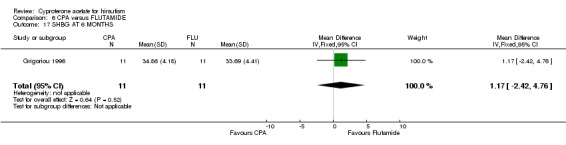
CYPROTERONE ACETATE VERSUS FLUTAMIDE The Ferriman Gallwey score was significantly higher at 12 months in the women treated with cyproterone acetate compared with flutamide. However, there was no difference in the Ferriman Gallwey scores between the groups at three and six months. There was only data from one study (Fruzetti 1999) available to compare the clinical outcome at 12 months, whereas there were three studies incorporated in the analysis of data at three months and two studies used in analysing the outcome at six months. The serum free testosterone was significantly lower at three, six and 12 months in the women treated with cyproterone acetate compared with flutamide. The total testosterone was also significantly lower at six months in the group treated with cyproterone acetate. There was no difference in androstenedione, DHEAS or SHBG levels.
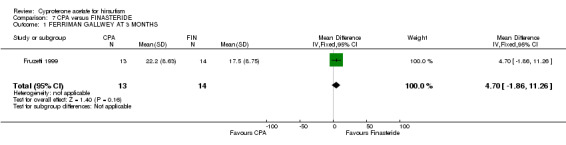
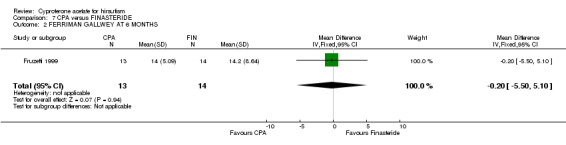
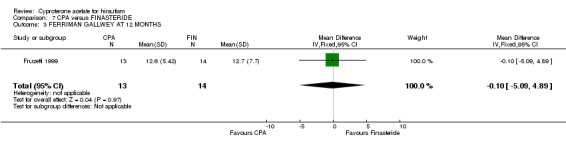
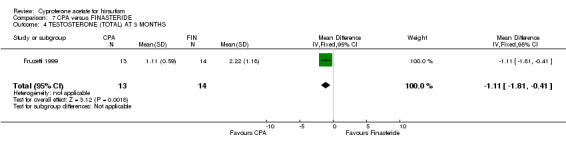
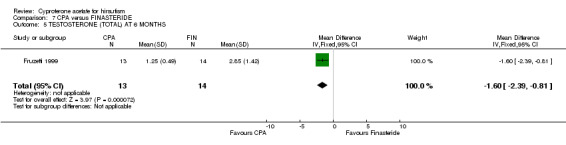
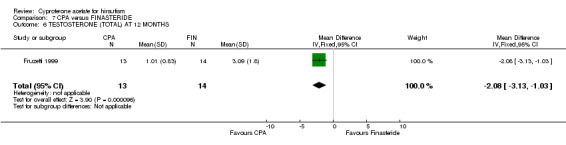
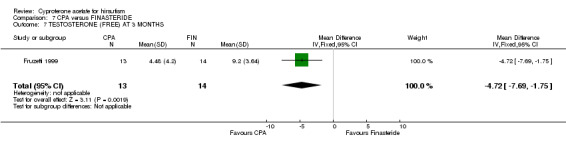
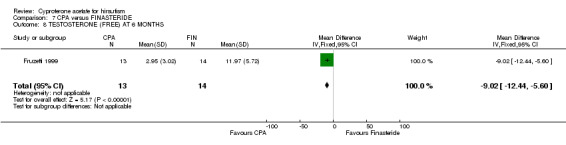
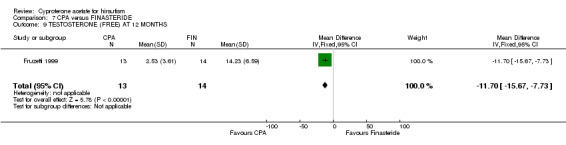
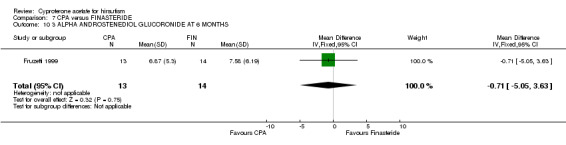
CYPROTERONE ACETATE VERSUS FINASTERIDE The total testosterone and free testosterone levels were lower in the women treated with cyproterone acetate group compared with those treated with finasteride at three, six and 12 months. There was no difference in the urinary three alpha androstanediol glucuronide levels between these groups.
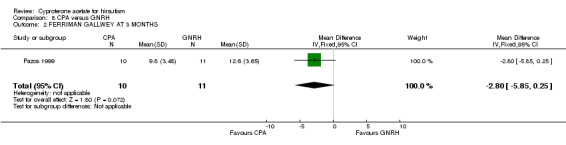
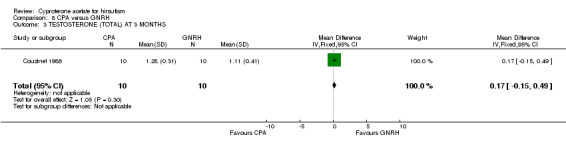
CYPROTERONE ACETATE VERSUS GnRH ANALOGUES There were no clinical or endocrine differences found when cyproterone acetate was compared with GnRH analogues.
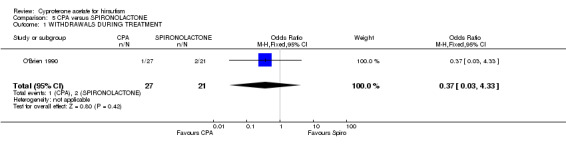
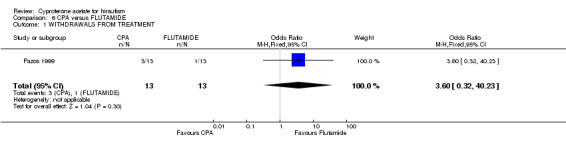
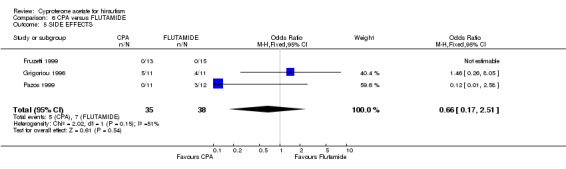
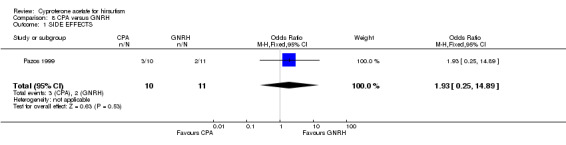
CYPROTERONE ACETATE VERSUS OTHER MEDICAL THERAPY ‐ SIDE EFFECTS AND WITHDRAWALS FROM THERAPY The incidence of side effects to therapy with cyproterone acetate compared to spironolactone, flutamide and GnRH analogues was not significantly different. There was insufficient data to compare side effects experienced with ketoconazole or finasteride therapy. There was no difference in the number of women withdrawing while on therapy from trials comparing cyproterone acetate to spironolactone or flutamide.
Discussion
There was considerable variation in the trial methods used to evaluate the effect of cyproterone acetate and other drugs on hirsutism in the studies which we reviewed. Most studies used the Ferriman Gallwey score to assess hirsutism clinically and androgen levels as surrogate markers. Linear hair growth and hair shaft diameter are more accurate objective ways to assess hirsutism, but were only used in one study in this review. Only studies evaluating hirsutism were included, whereas those assessing acne were excluded in order to have a more homogenous group for analysis. The previous review on therapy in hirsutism published in the Cochrane library evaluated spironolactone treatment in patients with acne or hirsutism.
There were no data comparing cyproterone acetate alone to placebo. In addition there were no data comparing cyproterone acetate alone to combination therapy using cyproterone acetate and ethinyl estradiol. The fundamental question of whether cyproterone acetate is less effective without ethinyl estradiol could not be answered in this review because of the lack of published data.
Only one double blind study comparing cyproterone acetate (2mg) in combination with ethinyl estradiol to placebo was included. Although there was a statistically significant subjective improvement in hirsutism, the finding was imprecise with large confidence limits. In addition, no objective evaluation was performed.
There were no clinical differences in hirsutism detected when cyproterone acetate was compared to other drug therapies (spironolactone, finasteride, GnRH analogues, ketoconazole). The only difference in clinical outcome was an improved Ferriman Gallwey score at 12 months when cyproterone acetate was compared with flutamide, but this finding was probably not a true difference since more robust comparative data at three and six months did not support any difference between the two drugs.
There were endocrinological differences in hormone levels in women treated with different therapies which may be explained by the mode of action of the drugs.
Cyproterone acetate works by various mechanisms. It binds to the dihydrotestosterone receptor in the cytoplasm in the hair follicle preventing its translocation into the nucleus to cause an androgenic effect. In addition to this receptor activity it inhibits five alpha reductase activity reducing DHT production, and also inhibits the production of the gonadotrophins. The reduced gonadotrophin levels in turn reduces steroidogenesis.
Ketoconazole is a enzyme inhibitor blocking the cytochrome P450 enzyme system reducing steroid hormone production. The women treated with ketoconazole had lower free testosterone, estradiol and DHEAS levels than those women treated with cyproterone acetate. The results indicate that ketoconazole is a more powerful enzyme inhibitor than CPA, resulting in lower serum levels of androgens. The most likely reason this did not translate into a clinical difference was because the cyproterone acetate also acts through additional mechanisms to reduce hirsutism.
Spironolactone is an aldosterone antagonist but is also know to have some effect on the cytochrome P450 enzyme system. It seemed to be as effective as cyproterone acetate in enzyme inhibition as no difference in serum androgens was demonstrated between these two therapies.
Flutamide does not reduce steroidogenesis but inhibits the effect of androgens by receptor blockade. The serum androgens (both free and total testosterone) were higher in the flutamide group than in the cyproterone acetate group. Although the serum androgen levels were higher with flutamide the net clinical effect was not worse because the androgen effect was blocked at the target tissue level.
Finasteride is a five alpha reductase inhibitor used in urology for treating prostatic disease and in gynaecology for treating hyperandrogenism. It is not known to reduce steroidogenesis, and the serum free and total testosterone levels were higher in this group than in the group treated with cyproterone acetate. Although the serum androgen levels were higher, the clinical effect was blocked by the lack of activity of the five alpha reductase enzyme which could not convert the testosterone to the highly active dihydro‐testosterone at the tissue level.
GnRH agonist analogues cause pituitary down regulation and desensitisation with the resultant reduction of bioactive gonadotrophins and decreased ovarian steroidogenesis. There were limited data available in this review to compare the effects on steroidogenesis of GnRH analogues in comparison to cyproterone acetate.
In summary, cyproterone acetate acts both by inhibition of steroidogenesis and through a peripheral effect (receptor blockade and five alpha reductase inhibition). Ketoconazole therapy resulted in more powerful inhibition of steroidogenesis than cyproterone acetate, whereas spironolactone resulted in a similar degree of inhibition. Neither flutamide and finasteride inhibited steroid hormone production but are active at a peripheral level. Although the medication caused different effects endocrinologically, this did not result in a clinical difference and was simply related to their mode of action.
In addition there were no reported differences in side effects between cyproterone acetate and flutamide or spironolactone. Data were not available comparing side effects between women treated with cyproterone acetate and ketoconazole, finasteride and GnRH analogue. This would be important information since it may ultimately determine which is the safest medication with which to treat women with hirsutism. Definitive conclusions cannot be drawn from this review on the true incidence of side effects related to the different drugs due to insufficient data.
Authors' conclusions
Implications for practice.
Although in one study cyproterone acetate therapy resulted in a subjective improvement in hirsutism compared with placebo, this was a small study with only 20 participants and the results had wide confidence intervals. All the medication used to treat hirsutism in this review (cyproterone acetate, spironolactone, ketoconazole, flutamide, finasteride and GnRH agonist analogues) resulted in a similar improvement in hirsutism. They acted by different mechanisms and the change in serum androgen levels therefore did not necessarily correlate with the degree of success in treating hirsutism.
The incidence of side effects with the different therapies could not be adequately assessed due to limited data. Cyproterone acetate (in combination with ethinyl estradiol) is a good first line therapy for treating hirsutism. Although it is generally accepted that cyproterone acetate is acceptable therapy, the lack of data from randomised controlled trials and the absence of objective assessments of therapy result in inadequate documentation and quantification of effect. Further studies are needed to evaluate the potential side effects of therapies to treating hirsutism.
Implications for research.
There is a need for larger randomised trials using objective methods to evaluate hirsutism combined with endocrinological assessment.
What's new
| Date | Event | Description |
|---|---|---|
| 31 March 2009 | Amended | Reference McKnight 1984 edited |
| 7 November 2008 | Amended | Converted to new review format. |
History
Protocol first published: Issue 2, 1998 Review first published: Issue 4, 2003
| Date | Event | Description |
|---|---|---|
| 17 July 2003 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
Nil
Data and analyses
Comparison 2. CPA (2MG) + EE versus PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SUBJECTIVE IMPROVEMENT IN HAIR GROWTH | 1 | 20 | Odds Ratio (M‐H, Fixed, 95% CI) | 45.0 [2.01, 1006.75] |
2.1. Analysis.
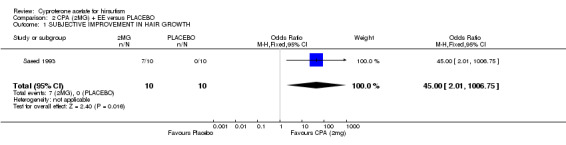
Comparison 2 CPA (2MG) + EE versus PLACEBO, Outcome 1 SUBJECTIVE IMPROVEMENT IN HAIR GROWTH.
Comparison 3. CPA (>2MG) + EE versus CPA(2MG) + EE.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 FERRIMAN GALLWEY AT 6 MONTHS | 1 | 113 | Mean Difference (IV, Fixed, 95% CI) | 1.10 [‐0.71, 2.91] |
| 2 TESTOSTERONE (TOTAL) AT 6 MONTHS | 1 | 113 | Mean Difference (IV, Fixed, 95% CI) | ‐0.49 [‐1.78, 0.80] |
| 3 TESTOSTERONE LEVEL (FREE) AT 6 MONTHS | 1 | 113 | Mean Difference (IV, Fixed, 95% CI) | 0.35 [‐0.61, 1.31] |
| 4 ANDROSTENEDIONE LEVEL AT 6 MONTHS | 1 | 113 | Mean Difference (IV, Fixed, 95% CI) | ‐0.35 [‐1.32, 0.62] |
| 5 DHEAS LEVEL AT 6 MONTHS | 1 | 113 | Mean Difference (IV, Fixed, 95% CI) | 0.18 [1.00, 1.36] |
| 6 ESTRADIOL LEVEL AT 6 MONTHS | 1 | 113 | Mean Difference (IV, Fixed, 95% CI) | ‐19.0 [‐103.67, 65.67] |
3.1. Analysis.
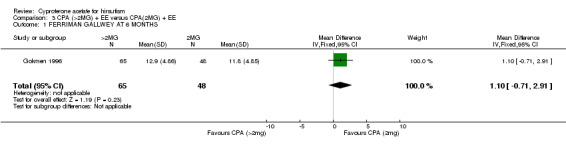
Comparison 3 CPA (>2MG) + EE versus CPA(2MG) + EE, Outcome 1 FERRIMAN GALLWEY AT 6 MONTHS.
3.2. Analysis.
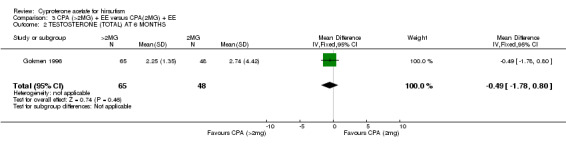
Comparison 3 CPA (>2MG) + EE versus CPA(2MG) + EE, Outcome 2 TESTOSTERONE (TOTAL) AT 6 MONTHS.
3.3. Analysis.
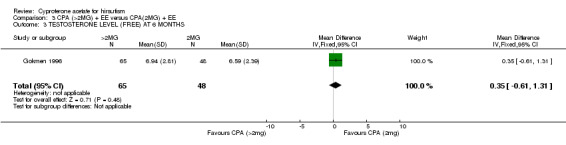
Comparison 3 CPA (>2MG) + EE versus CPA(2MG) + EE, Outcome 3 TESTOSTERONE LEVEL (FREE) AT 6 MONTHS.
3.4. Analysis.
Comparison 3 CPA (>2MG) + EE versus CPA(2MG) + EE, Outcome 4 ANDROSTENEDIONE LEVEL AT 6 MONTHS.
3.5. Analysis.
Comparison 3 CPA (>2MG) + EE versus CPA(2MG) + EE, Outcome 5 DHEAS LEVEL AT 6 MONTHS.
3.6. Analysis.
Comparison 3 CPA (>2MG) + EE versus CPA(2MG) + EE, Outcome 6 ESTRADIOL LEVEL AT 6 MONTHS.
Comparison 4. CPA versus KETOCONAZOLE.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 FERRIMAN GALLWEY AT 6 MONTHS | 1 | 81 | Mean Difference (IV, Fixed, 95% CI) | 0.70 [‐0.84, 2.24] |
| 2 TESTOSTERONE (TOTAL) AT 6 MONTHS | 1 | 81 | Mean Difference (IV, Fixed, 95% CI) | ‐0.02 [‐0.37, 0.33] |
| 3 TESTOSTERONE (FREE) AT 6 MONTHS | 1 | 81 | Mean Difference (IV, Fixed, 95% CI) | 1.39 [0.43, 2.35] |
| 4 ANDROSTENEDIONE AT 6 MONTHS | 1 | 81 | Mean Difference (IV, Fixed, 95% CI) | 0.35 [‐0.62, 1.32] |
| 5 DHEAS AT 6 MONTHS | 1 | 81 | Mean Difference (IV, Fixed, 95% CI) | 2.87 [1.99, 3.75] |
| 6 ESTRADIOL AT 6 MONTHS | 1 | 81 | Mean Difference (IV, Fixed, 95% CI) | 135.0 [59.92, 210.08] |
4.1. Analysis.
Comparison 4 CPA versus KETOCONAZOLE, Outcome 1 FERRIMAN GALLWEY AT 6 MONTHS.
4.2. Analysis.
Comparison 4 CPA versus KETOCONAZOLE, Outcome 2 TESTOSTERONE (TOTAL) AT 6 MONTHS.
4.3. Analysis.
Comparison 4 CPA versus KETOCONAZOLE, Outcome 3 TESTOSTERONE (FREE) AT 6 MONTHS.
4.4. Analysis.
Comparison 4 CPA versus KETOCONAZOLE, Outcome 4 ANDROSTENEDIONE AT 6 MONTHS.
4.5. Analysis.
Comparison 4 CPA versus KETOCONAZOLE, Outcome 5 DHEAS AT 6 MONTHS.
4.6. Analysis.
Comparison 4 CPA versus KETOCONAZOLE, Outcome 6 ESTRADIOL AT 6 MONTHS.
Comparison 5. CPA versus SPIRONOLACTONE.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 WITHDRAWALS DURING TREATMENT | 1 | 48 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.37 [0.03, 4.33] |
| 2 FERRIMAN GALLWEY AT 3 MONTHS | 2 | 83 | Mean Difference (IV, Fixed, 95% CI) | ‐1.98 [‐4.12, 0.16] |
| 3 FERRIMAN GALLWEY AT 6 MONTHS | 3 | 160 | Mean Difference (IV, Fixed, 95% CI) | ‐1.35 [‐2.87, 0.18] |
| 4 SIDE EFFECTS DURING TREATMENT | 2 | 90 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.75 [0.21, 2.70] |
| 5 LINEAR HAIR GROWTH AT 3 MONTHS | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | 0.02 [‐0.03, 0.07] |
| 6 LINEAR HAIR GROWTH AT 6 MONTHS | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | ‐0.04 [‐0.09, 0.01] |
| 7 HAIR SHAFT DIAMETER AT 6 MONTHS | 1 | 45 | Mean Difference (IV, Fixed, 95% CI) | 3.00 [‐23.85, 29.85] |
| 8 TESTOSTERONE (TOTAL) AT 6 MONTHS | 3 | 164 | Mean Difference (IV, Fixed, 95% CI) | ‐0.00 [‐0.28, 0.27] |
| 9 TESTOSTERONE (FREE) AT 6 MONTHS | 1 | 77 | Mean Difference (IV, Fixed, 95% CI) | 0.35 [‐0.62, 1.32] |
| 10 ANDROSTENEDIONE AT 6 MONTHS | 2 | 122 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.66, 1.25] |
| 11 DHEAS AT 6 MONTHS | 3 | 164 | Mean Difference (IV, Fixed, 95% CI) | ‐0.74 [‐1.71, 0.24] |
| 12 SHBG AT 6 MONTHS | 1 | 45 | Mean Difference (IV, Fixed, 95% CI) | 9.20 [‐27.20, 45.60] |
| 13 ESTRADIOL AT 6 MONTHS | 1 | 77 | Mean Difference (IV, Fixed, 95% CI) | 119.00 [10.84, 227.16] |
5.1. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 1 WITHDRAWALS DURING TREATMENT.
5.2. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 2 FERRIMAN GALLWEY AT 3 MONTHS.
5.3. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 3 FERRIMAN GALLWEY AT 6 MONTHS.
5.4. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 4 SIDE EFFECTS DURING TREATMENT.
5.5. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 5 LINEAR HAIR GROWTH AT 3 MONTHS.
5.6. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 6 LINEAR HAIR GROWTH AT 6 MONTHS.
5.7. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 7 HAIR SHAFT DIAMETER AT 6 MONTHS.
5.8. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 8 TESTOSTERONE (TOTAL) AT 6 MONTHS.
5.9. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 9 TESTOSTERONE (FREE) AT 6 MONTHS.
5.10. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 10 ANDROSTENEDIONE AT 6 MONTHS.
5.11. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 11 DHEAS AT 6 MONTHS.
5.12. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 12 SHBG AT 6 MONTHS.
5.13. Analysis.
Comparison 5 CPA versus SPIRONOLACTONE, Outcome 13 ESTRADIOL AT 6 MONTHS.
Comparison 6. CPA versus FLUTAMIDE.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 WITHDRAWALS FROM TREATMENT | 1 | 26 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.6 [0.32, 40.23] |
| 2 FERRIMAN GALLWEY AT 3 MONTHS | 3 | 72 | Mean Difference (IV, Fixed, 95% CI) | 0.37 [‐1.22, 1.95] |
| 3 FERRIMAN GALLWEY AT 6 MONTHS | 2 | 50 | Mean Difference (IV, Fixed, 95% CI) | 1.50 [‐1.06, 4.06] |
| 4 FERRIMAN GALLWEY AT 12 MONTHS | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | 4.5 [0.47, 8.53] |
| 5 SIDE EFFECTS | 3 | 73 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.17, 2.51] |
| 6 TESTOSTERONE (TOTAL) AT 3 MONTHS | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [‐0.45, 0.45] |
| 7 TESTOSTERONE (TOTAL) AT 6 MONTHS | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | ‐0.69 [‐1.14, ‐0.24] |
| 8 TESTOSTERONE (FREE) AT 3 MONTHS | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | ‐5.37 [‐10.29, ‐0.45] |
| 9 TESTOSTERONE (FREE) AT 6 MONTHS | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | ‐4.16 [‐6.62, ‐1.70] |
| 10 TESTOSTERONE (FREE) AT 12 MONTHS | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | ‐4.55 [‐7.43, ‐1.67] |
| 11 ANDROSTENEDIONE AT 3 MONTHS | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | ‐2.79 [‐6.51, 0.93] |
| 12 ANDROSTENEDIONE AT 6 MONTHS | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | ‐2.45 [‐5.90, 1.00] |
| 13 DHEAS AT 3 MONTHS | 2 | 50 | Mean Difference (IV, Fixed, 95% CI) | 0.41 [‐0.04, 0.85] |
| 14 DHEAS AT 6 MONTHS | 2 | 50 | Mean Difference (IV, Fixed, 95% CI) | 0.28 [‐0.31, 0.87] |
| 15 DHEAS AT 12 MONTHS | 1 | 28 | Mean Difference (IV, Fixed, 95% CI) | 1.16 [‐0.38, 2.70] |
| 16 SHBG AT 3 MONTHS | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | 1.19 [‐1.57, 3.95] |
| 17 SHBG AT 6 MONTHS | 1 | 22 | Mean Difference (IV, Fixed, 95% CI) | 1.17 [‐2.42, 4.76] |
6.1. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 1 WITHDRAWALS FROM TREATMENT.
6.2. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 2 FERRIMAN GALLWEY AT 3 MONTHS.
6.3. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 3 FERRIMAN GALLWEY AT 6 MONTHS.
6.4. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 4 FERRIMAN GALLWEY AT 12 MONTHS.
6.5. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 5 SIDE EFFECTS.
6.6. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 6 TESTOSTERONE (TOTAL) AT 3 MONTHS.
6.7. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 7 TESTOSTERONE (TOTAL) AT 6 MONTHS.
6.8. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 8 TESTOSTERONE (FREE) AT 3 MONTHS.
6.9. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 9 TESTOSTERONE (FREE) AT 6 MONTHS.
6.10. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 10 TESTOSTERONE (FREE) AT 12 MONTHS.
6.11. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 11 ANDROSTENEDIONE AT 3 MONTHS.
6.12. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 12 ANDROSTENEDIONE AT 6 MONTHS.
6.13. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 13 DHEAS AT 3 MONTHS.
6.14. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 14 DHEAS AT 6 MONTHS.
6.15. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 15 DHEAS AT 12 MONTHS.
6.16. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 16 SHBG AT 3 MONTHS.
6.17. Analysis.
Comparison 6 CPA versus FLUTAMIDE, Outcome 17 SHBG AT 6 MONTHS.
Comparison 7. CPA versus FINASTERIDE.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 FERRIMAN GALLWEY AT 3 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | 4.70 [‐1.86, 11.26] |
| 2 FERRIMAN GALLWEY AT 6 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐5.50, 5.10] |
| 3 FERRIMAN GALLWEY AT 12 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐5.09, 4.89] |
| 4 TESTOSTERONE (TOTAL) AT 3 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐1.11 [‐1.81, ‐0.41] |
| 5 TESTOSTERONE (TOTAL) AT 6 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐1.60 [‐2.39, ‐0.81] |
| 6 TESTOSTERONE (TOTAL) AT 12 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐2.08 [‐3.13, ‐1.03] |
| 7 TESTOSTERONE (FREE) AT 3 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐4.72 [‐7.69, ‐1.75] |
| 8 TESTOSTERONE (FREE) AT 6 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐9.02 [‐12.44, ‐5.60] |
| 9 TESTOSTERONE (FREE) AT 12 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐11.70 [‐15.67, ‐7.73] |
| 10 3 ALPHA ANDROSTENEDIOL GLUCORONIDE AT 6 MONTHS | 1 | 27 | Mean Difference (IV, Fixed, 95% CI) | ‐0.71 [‐5.05, 3.63] |
7.1. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 1 FERRIMAN GALLWEY AT 3 MONTHS.
7.2. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 2 FERRIMAN GALLWEY AT 6 MONTHS.
7.3. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 3 FERRIMAN GALLWEY AT 12 MONTHS.
7.4. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 4 TESTOSTERONE (TOTAL) AT 3 MONTHS.
7.5. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 5 TESTOSTERONE (TOTAL) AT 6 MONTHS.
7.6. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 6 TESTOSTERONE (TOTAL) AT 12 MONTHS.
7.7. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 7 TESTOSTERONE (FREE) AT 3 MONTHS.
7.8. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 8 TESTOSTERONE (FREE) AT 6 MONTHS.
7.9. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 9 TESTOSTERONE (FREE) AT 12 MONTHS.
7.10. Analysis.
Comparison 7 CPA versus FINASTERIDE, Outcome 10 3 ALPHA ANDROSTENEDIOL GLUCORONIDE AT 6 MONTHS.
Comparison 8. CPA versus GNRH.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 SIDE EFFECTS | 1 | 21 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.93 [0.25, 14.89] |
| 2 FERRIMAN GALLWEY AT 3 MONTHS | 1 | 21 | Mean Difference (IV, Fixed, 95% CI) | ‐2.80 [‐5.85, 0.25] |
| 3 TESTOSTERONE (TOTAL) AT 3 MONTHS | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | 0.17 [‐0.15, 0.49] |
| 4 ANDROSTENEDIONE AT 3 MONTHS | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | 0.66 [‐0.44, 1.76] |
8.1. Analysis.
Comparison 8 CPA versus GNRH, Outcome 1 SIDE EFFECTS.
8.2. Analysis.
Comparison 8 CPA versus GNRH, Outcome 2 FERRIMAN GALLWEY AT 3 MONTHS.
8.3. Analysis.
Comparison 8 CPA versus GNRH, Outcome 3 TESTOSTERONE (TOTAL) AT 3 MONTHS.
8.4. Analysis.
Comparison 8 CPA versus GNRH, Outcome 4 ANDROSTENEDIONE AT 3 MONTHS.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Couzinet 1986.
| Methods | Cross over study. 1 centre. No power calc. 10 women. No withdrawals. | |
| Participants | PCO by clinical and biochemical tests. Age 20‐35. Endo unit, Hospital de Bicentre, France. No exclusion criteria stated. | |
| Interventions | 1) CPA 50MG daily. 2) D‐ TRYPTOPHAN 6 LHRH IM monthly injection (GNRH) 3 months study duration for each intervention. | |
| Outcomes | FG score E2,E1,TESTO, DHEAS, ANDROSTENEDIONE, 3ALPHA ANDROSTANEDIOL. | |
| Notes | FG figures not available. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Dixon 1991.
| Methods | Not blinded. 1 centre. No power calc. 41 women analysed. Withdrawals not stated. No ITT analyses. | |
| Participants | Hirsute women. Age 18‐45. Gynae or Endo clinics, Guys Hospital, London. Exclusion criteria not stated. | |
| Interventions | 1) Spironolactone + EE (Ovysmen) 2) CPA + EE 6 months duration. | |
| Outcomes | FG score. Linear hair growth. | |
| Notes | Photographic method for hair measurement. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Erenus 1996.
| Methods | Single blinding. 1 centre. No power calc. 42 women randomised. 42 analysed. no withdrawals. No intention to treat (ITT) analyses. | |
| Participants | Hirsute women. Age mean group 1 20.1 (SD3.7), group 2 22.3 (SD 5.6). Marmara University School of Medicine. Istanbul, Turkey. Exclusion criteria not stated. | |
| Interventions | 1) Spironolactone (100MG) + EE (OC) 2) CPA 50MG Day 1‐10 + EE (OC ‐ Diane) 9 months. | |
| Outcomes | FG score. Testo, DHEAS. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Fruzetti 1999.
| Methods | Unclear blinding. No power calc. 45 women randomised. 42 analysed. 3 withdrawals for personal reasons. No ITT analyses. | |
| Participants | Women with hirsutism. No hormonal treatment for 6 months prior to study. Age 16‐29 years. Reprod. Endo. OPD Clinic. University of Pisa. | |
| Interventions | 1) CA 25MG Day 1‐10 plus EE 20mcg D1‐21. 2) Finasteride 5mg/day 3) Flutamide 250mg daily. No placebo. 12 months. | |
| Outcomes | FG score. Total / free testosterone, androstenedione, DHEAS, SHBG, DHT,3 alpha androstanediol glucuronide. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Gokmen 1996.
| Methods | Unclear blinding. One centre. 173 women randomised. Two stage randomisation. Second two groups added to randomisation after study already commenced. 141 analysed. 32 withdrawals. No ITT analysis. Source of funding ‐ not stated. | |
| Participants | Complaint hirsutism. PCO on ultrasound + 1 biochemical abnormality. Age 14‐39. Exclusions: ‐ Hyperandrogenism other than ovarian ‐ Failure to come for follow up. Reprod Endo Clinic. Ankara, Turkey. | |
| Interventions | 1) Diane 2) CA 100 Day 1‐10 OF Diane + Diane. 3) Spironolactone 100‐200mg individually adjusted. 4) Ketoconazole 400mg daily. Duration 6 months. | |
| Outcomes | FG score. BMI Estradiol Testosterone (free and total) Androstenedione DHEAS | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Grigoriou 1996.
| Methods | Not blinded. 1 centre. No power calc. 22 women randomised. No withdrawals. | |
| Participants | Idiopathic hirsutism. Age 16‐32. O&G dept, University of Athens, Greece. | |
| Interventions | 1) CPA 100mg Day 5‐14. 2) Flutamide 250mg twice daily. 9 months duration. | |
| Outcomes | FG score. Testosterone Androstenedione DHEAS SHBG | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | High risk | C ‐ Inadequate |
O'Brien 1990.
| Methods | Not blinded. 1 centre. No power calc. 50 women randomised. 2 withdrawals for personal reasons. 3 withdrawals during study period. Analysed ‐19 spironolactone and 26 CPA. | |
| Participants | Hirsute women. Cosmetic methods inadequate. Age 19‐46. Excluded: cliteromegaly. Endo Dept. Autin University Hospital. Heidelberg, Victoria, Australia. | |
| Interventions | 1) Spironolactone (100mg) + EE 2) CPA (100mg) Day 5‐14 + EE 6 months duration. | |
| Outcomes | Hair diameter. Testosterone Androstenedione DHEAS SHBG | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Pazos 1999.
| Methods | Unclear blinding. 39 randomised. 33 analysed. 6 withdrawals. No ITT analyses. | |
| Participants | Idiopathic and ovarian hirsutism. Exclusion: adrenal hyperandrogenism. Dept Endo, Hospital Ramon Ycajal, Madrid, Spain. |
|
| Interventions | 1) Triptorelin 3.75mg IM every 28 days 2) CA 100mg Day 1‐10 3) Flutamide 250mg twice daily. All patients on COCP. 9 months duration. | |
| Outcomes | FG score Endocrine measurements. | |
| Notes | Endocrine values not available ‐ only graphs. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Unclear risk | B ‐ Unclear |
Saeed 1993.
| Methods | Double blinded study. 1 centre. No power calc. 20 women randomised and analysed. | |
| Participants | PCOS with hirsutism. Age 17‐31. Exclusion criteria not stated. Iqbal Medical College, Lahore. | |
| Interventions | 1) CPA (2mg) + EE ‐ Diane 2) Placebo 12 months | |
| Outcomes | Subjective improvement in hirsutism. Testosterone DHEAS | |
| Notes | Endocrine values not available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Adamopoulous 1988 | Assessment of sexual activity before and after treatment with CPA. Not randomised study. |
| Barth 1991 | Mean data not presented in paper. Cannot be used in meta‐analysis. |
| Belisle 1986 | Randomised study. Insufficient data given for analysis. |
| Beylot 1998 | Review, not original study. |
| Carmina 1998 | No CPA included in groups. |
| Castelo‐Branco 1998 | Effects of CPA on bone mass. Not hirsute women. |
| Consoli 1994 | Randomised study comparing 2 routes of estrogen administration. Both groups received CPA. |
| Cremoncini 1976 | Not randomised |
| Erkkola 1990 | Some women only acne, not hirsutism. |
| Frank‐Raue 1990 | Not randomised. |
| Gruber 1998 | Topical CPA therapy. |
| Grund 1975 | Not a randomised study. |
| Holdaway 1985 | Women pre‐treated with study drug prior to randomisation. |
| Jasonni 1991 | Not randomised. |
| Kelestimur 1997 | Both groups contain CPA. Study to compare the additive effect of spironolactone with CPA. |
| Kuttenn 1980 | Not randomised. |
| Lachnit‐Fixson 1977 | Women with acne without hirsutism included. |
| Lachnit‐Fixson 1979 | Review, not original study. |
| Marcondes 1990 | Not randomised. No control. |
| Moltz 1984 | Women with acne or hirsutism recruited. Unable to differentiate groups in the results. |
| Pasquali 1986 | Randomised study of two diet regimes. CPA in both groups. |
| Porcile 1991 | Outcome data not available. |
| Pucci 1997 | Review. Not original study. |
| Pugeat 1991 | Not randomised. |
| Rigaud 1983 | Not randomised. |
| Rittmaster 1999 | Review. Not original study. |
| Sahin 1998 | Not randomised. |
| Schmidt 1987 | Both groups contain CPA. Dose finding study. |
| Tartagni 2000 | Both groups contain Diane. Study assessing the additive effect of adding finasteride. |
| Thomas 1985 | Not randomised. |
| van der Spuy 1995 | Both groups contain CPA. Study to assess the additive effect of GnRH agonist analogue. |
| Vegetti 1996 | Both groups contain CPA. A study to assess the additive effect of GnRH agonist analogue. |
| Ventoroli 1999 | 14 women in study had non‐classical congenital adrenal hyperplasia. |
| Vermeulen 1988 | Both groups contain Diane (CPA). A study to assess two doses of estradiol. |
| Vexiau 1995 | Randomised study of two routes of estrogen therapy. |
| Young 1998 | Review. Not original study. |
Contributions of authors
Both reviewers contributed to all aspects of the preparation of this review.
Declarations of interest
Schering Pharmaceuticals supplied some of the medication for an ongoing study of the treatment of hirsutism in our department, but were not involved in any way with this review.
Edited (no change to conclusions)
References
References to studies included in this review
Couzinet 1986 {published data only}
- Couzinet B, Strat N, Brailly S, Schaison G. Comparative effects of cyproterone acetate or a long acting gonadotrophin releasing hormone agonist in polycystic ovary disease. Journal of Clinical Endocrinology and Metabolism 1986;63(4):1031‐5. [DOI] [PubMed] [Google Scholar]
Dixon 1991 {published data only}
- Dixon JE, Hicks BH, Chapman MG. Hirsutography: photographic measurement of linear hair growth in hirsute women during comparison of anti‐androgen treatments. Journal of Obstetrics and Gynaecology 1991;11(1):63‐7. [Google Scholar]
Erenus 1996 {published data only}
- Erenus M, Yucelten D, Gurbuz O, Durmusoglu F, Pekin S. Comparison of spironolactone‐oral contraceptive versus cyproterone acetate‐estrogen regimens in the treatment of hirsutism. Fertility and Sterility 1996;22(2):216‐9. [DOI] [PubMed] [Google Scholar]
Fruzetti 1999 {published data only}
- Fruzetti F, Bersi C, Parrini D, Ricci C, Genazzani R. Treatment of hirsutism: comparisons between different antiandrogens with central and peripheral effects. Fertility and Sterility 1999;71(3):445‐51. [DOI] [PubMed] [Google Scholar]
Gokmen 1996 {published data only}
- Gokmen O, Senoz B, Gulekli B, Isik AZ. Comparison of four different treatment regimens in hirsutism related to polycystic ovary syndrome. Gynaecological Endocrinology 1996;10(4):249‐55. [DOI] [PubMed] [Google Scholar]
Grigoriou 1996 {published data only}
- Grigoriou O, Papadias C, Konidaris S, Antoniou G, Karakitsos P, Giannikos L. Comparison of flutamide and cyproterone acetate in the treatment of hirsutism: a randomised controlled trial. Gynaecological Endocrinology 1996;10(2):119‐23. [DOI] [PubMed] [Google Scholar]
O'Brien 1990 {published data only}
- O'Brien RC, Cooper ME, Murray RML, Seeman E, Thomas AK, Jerums G. Comparison of sequential cyproterone acetate/estrogen versus spironolactone /oral contraceptive in the treatment of hirsutism. Journal of Clinical Endocrinology and Metabolism 1991;72(5):1008‐13. [DOI] [PubMed] [Google Scholar]
Pazos 1999 {published data only}
- Pazos F, Escobar‐Morreale HF, Balsa J, Sancho JM, Varela C. Prospective randomised study comparing the long‐acting gonadotrophin‐releasing hormone agonist triptorelin, flutamide and cyproterone acetate, used in combination with an oral contraceptive, in the treatment of hirsutism. Fertility and Sterility 1999;71(1):122‐8. [DOI] [PubMed] [Google Scholar]
Saeed 1993 {published data only}
- Saeed R, Akram J, Changezi HU, Saeed M. Treatment of hirustism in polycystic ovary syndrome with Diane, 50 mcg ethinyl estradiol and 2mg cyproterone acetate. Pakistan Journal of Medical Science 1993;9(2):109‐12. [Google Scholar]
References to studies excluded from this review
Adamopoulous 1988 {published data only}
- Adamopoulos DA, Kampyli S, Georgiacodis F, Kapolla N, Abrahamian‐Michalakis A. Effects of anti‐androgen estrogen treatment on sexual and endocrine parameters in hirsute women. Archives of Sexual Behaviour 1988;17(5):421‐9. [DOI] [PubMed] [Google Scholar]
Barth 1991 {published data only}
- Barth JH, Cherry F, Wojnarowska F, Dawber RPR. Cyproterone acetate for severe hirsutism: results of a double blind dose‐ranging study. Clinical Endocrinology 1991;35(1):5‐10. [DOI] [PubMed] [Google Scholar]
Belisle 1986 {published data only}
- Belisle S, Love EJ. Clinical efficacy and safety of cyproterone acetate in severe hirsutism : results of a multicentered Canadian study. Fertility and Sterility 1986;46(6):1015‐20. [PubMed] [Google Scholar]
Beylot 1998 {published data only}
- Beylot C, Doutre MS, Barry M. Oral contraceptives and cyproterone acetate in female acne treatment. Dermatology 1998;196(1):148‐52. [DOI] [PubMed] [Google Scholar]
Carmina 1998 {published data only}
- Carmina E, Lobo RA. The addition of dexamethazone to antiandrogen therapy for hirsutism prolongs the duration of remission. Fertility and Sterility 1998;69(6):1075‐9. [DOI] [PubMed] [Google Scholar]
Castelo‐Branco 1998 {published data only}
- Castelo‐Branco C, Martinez de Osaba MJ, Pons F, Vanrell JA. Effects of bone mass of two oral contraceptives containing ethinylestradiol and cyproterone acetate or desogestrel: results of a two year follow‐up. The European Journal of Contraception and Reproductive Health Care: the Official Journal of the European Society of Contraception 1998;3(2):79‐84. [DOI] [PubMed] [Google Scholar]
Consoli 1994 {published data only}
- Consoli SM, Vexiau P, Consoli SG, Abramovici Y. Acceptance, tolerance and effects on quality of life of treatment of hiruste women with cyproterone acetate. Comparison of associated treatment with oral estradiol to transdermal estradiol [Acceptabilite, tolerance et impact sur la qualite de la vie du traitement de la femme hirsute par lacetate de cyproterone. Comparaison de 2 schemas l'associant soit a l' estradiol per os, soit par voie transdermique]. Contraception, Fertilite, Sexualite 1994;22(12):783‐7. [PubMed] [Google Scholar]
Cremoncini 1976 {published data only}
- Cremoncini C, Vignati E, Libroia A. Treatment of hirsutism and acne in women with two combinations of cyproterone acetate and ethinylestradiol. International Symposium on Androgens and Anti‐androgens. 1976:300‐13. [PubMed]
Erkkola 1990 {published data only}
- Erkkola R, Hirvonen E, Luikku R, Lumme R, Mannikko H, Aydinlik S. Ovulation inhibitors containing cyproterone acetate or desogestrel in the treatment of hyperandrogenic symptoms. Acta Obstetricia et Gynecologica Scandinavica 1990;69(1):61‐5. [DOI] [PubMed] [Google Scholar]
Frank‐Raue 1990 {published data only}
- Frank‐Raue K, Junga G, Raue F, Vecsei P, Ziegler R. Therapy for women with hirsutism with adrenal enzyme defects of enzyme biosynthesis: compared with dexamethazone compbined with cyproterone acetate [Therapie des hirsutismus bei frauen mit adrenalen enzymdefekten der steroidhormonbiosynthese: vergleich von dexamethason mit cyproteronacetat]. Klinische Wochenschrift 1990;68(12):597‐601. [DOI] [PubMed] [Google Scholar]
Gruber 1998 {published data only}
- Gruber DM, Sator MO, Joura MO, Kokoscha EM, Heinze G, Huber JC. Topical cyproterone acetate treatment in women with acne: a placebo‐controlled trial. Archives of Dermatology 1998;134(4):459‐63. [DOI] [PubMed] [Google Scholar]
Grund 1975 {published data only}
- Grund E, Schmidt‐Elmendorff H. The treatment of virilizing syndromes. Comparative clinical studies of 2 antiandrogen‐active gestagens (cyproterone acetate, megestrol acetate) [Behandlung von virilisierungs‐ erscheinungen. Vergleichende klinische untersuchung zweier antiandrogenwirksamer gestagene (cyproteronazetat, megestrolazetat)]. Die Medizinische Welt 1975;26(48):2180‐7. [PubMed] [Google Scholar]
Holdaway 1985 {published data only}
- Holdaway IM, Croxson MS, Ibbertson HK, Sheehan A, Knox B, France J. Cyproterone acetate as intial treatment and maintenance therapy for hirsutism. Acta Endocrinologica 1985;109(4):522‐9. [DOI] [PubMed] [Google Scholar]
Jasonni 1991 {published data only}
- Jasonni VM, Bulletti C, Naldi S, Cosmo E, Cappuccini F, Flamigni C. Treatment of hirustism by an association of oral cyproterone acetate and transdermal 17 beta estradiol. Fertility and Sterility 1991;55(4):742‐5. [PubMed] [Google Scholar]
Kelestimur 1997 {published data only}
- Kelestimur F, Sahin Y. Comparison of Diane 35 and Diane 35 plus spironolactone in the treatment of hirsutism. Fertility and Sterility 1997;69(1):66‐9. [DOI] [PubMed] [Google Scholar]
Kuttenn 1980 {published data only}
- Kuttenn F, Rigaud C, Wright F, Mauvais‐Jarvis P. Treatment of hirsutism by oral cyproterone acetate and percutaneous estradiol. Journal of Clinical Endocrinology and Metabolism 1980;51(5):1107‐11. [DOI] [PubMed] [Google Scholar]
Lachnit‐Fixson 1977 {published data only}
- Lachnit‐Fixson U, Kaufmann J. Therapy of androgenisation symptoms [Zur beeinflussung von androgenisierungserscheinungen]. Medizinische Klinik 1977;72(45):1922‐6. [PubMed] [Google Scholar]
Lachnit‐Fixson 1979 {published data only}
- Lachnit‐Fixson U. The development and evaluation of an ovulation inhibitor (Diane) containing an antiandrogen. Acta Obstetricia et Gynecologica Scandinavica 1979;88(Suppl):33‐42. [DOI] [PubMed] [Google Scholar]
Marcondes 1990 {published data only}
- Marcondes JAM, Wajchenberg BL, Abujamra AC, Luthold WW, Samojlik E, Kirschner MA. Monthly cyproterone acetate in the treatment of hirsute women: clinical and laboratory effects. Fertility and Sterility 1990;53(1):40‐4. [DOI] [PubMed] [Google Scholar]
Moltz 1984 {published data only}
- Moltz L, Kaiser E. Medium dose cyproterone acetate therapy for women with moderate hyperandrogenism [Mittelhochdosierte orale cyproteronacetat‐therapie bie frauen mit mittelgradig ausgepragten androgenisierungserscheinungen]. Geburtshilfe und Frauenheilkunde 1984;44(1):47‐52. [DOI] [PubMed] [Google Scholar]
Pasquali 1986 {published data only}
- Pasquali R, Fabbri R, Venturoli S, Paradisi R, Antenucci D, Melchionda N. Effect of weight loss and antiandrogenic therapy on sex hormone blood levels and insulin resistance in obese patients with polycystic ovaries. American Journal of Obstetrics and Gynaecology 1986;154(1):139‐44. [DOI] [PubMed] [Google Scholar]
Porcile 1991 {published data only}
- Porcile A, Gallardo E. Long term treatment of hirustism: desogestrel compared with cyproterone acetate in oral contraceptives. Fertility and Sterility 1991;55(5):877‐81. [DOI] [PubMed] [Google Scholar]
Pucci 1997 {published data only}
- Pucci E, Petraglia F. Treatment of androgen excess in females: yesterday, today and tomorrow. Gynaecological Endocrinology 1997;11(6):411‐33. [DOI] [PubMed] [Google Scholar]
Pugeat 1991 {published data only}
- Pugeat M, Nicolas MH, Dechaud H, Elmidani M. Administration of cyproterone acetate and natural estrogens in the treatment of hirustism [Association d'acetate de cyproterone et d'estrogenes naturels dans le traitement de l'hirsutisme]. Journal of Obstetrics and Gynaecology and Reproductive Biology 1991;20:1057‐62. [PubMed] [Google Scholar]
Rigaud 1983 {published data only}
- Rigaud C, Vincens M, Mowszomicz I, Wright F, Mavier P, Nahoul K, et al. Action mechanisms of cyproterone acetate in the treatment of hirustism [Mecamisme d'action de l'acetate de cyproterone dans le traitement de l'hirsutisme]. Annals of Endocrinology 1983;44:387‐92. [PubMed] [Google Scholar]
Rittmaster 1999 {published data only}
- Rittmaster RS. Antiandrogen treatment of polycystic ovary syndrome. Endocrinology and Metabolism Clinics of North America 1999;28(2):409‐21. [DOI] [PubMed] [Google Scholar]
Sahin 1998 {published data only}
- Sahin Y, Bayram F, Kelestimur F, Muderris I. Comparison of cyproterone acetate plus ethinyl estradiol and finasteride in the treatment of hirsutism. Journal of Endocrinological Investigation 1998;21(6):348‐52. [DOI] [PubMed] [Google Scholar]
Schmidt 1987 {published data only}
- Schmidt JB, Huber J, Spona J. Parenteral and oral cyproterone acetate treatment in severe hirsutism. Gynecologic and Obstetric Investigation 1987;24(2):125‐30. [DOI] [PubMed] [Google Scholar]
Tartagni 2000 {published data only}
- Tartagni M, Schonauer LM, Salvia MA, Cicinelli E, Pergola G, D'Addario V. Comparison of Diane 35 and Diane 35 plus finasteride in the treatment of hirsutism. Fertility and Sterility 2000;73(4):718‐23. [DOI] [PubMed] [Google Scholar]
Thomas 1985 {published data only}
- Thomas AK, Slobodniuk R, Taft J, Cooper M, Montalto J, Jerums G. The treatment of hirustism: experience with cyproterone acetate and spironolactone. Australian Journal of Dermatology 1985;26(19):20‐3. [DOI] [PubMed] [Google Scholar]
van der Spuy 1995 {unpublished data only}
- Spuy ZM, Nugent FA. The managment of hirustism in PCOS using GnRH agonist analogue therapy. Abstract ‐ 27th British Congress of Obstetrics and Gynaecology 1995.
Vegetti 1996 {published data only}
- Vegetti W, Testa G, Maggioni P, Motta T, Falsetti L, Crosignani PG. An open randomised comparative study of an oral contraceptive containing ethinyl estradiol and cyproterone acetate with and without the GnRH analogue goserelin in the long term treatment of hirsutism. Gynecologic and Obstetric Investigation 1996;41(4):260‐8. [DOI] [PubMed] [Google Scholar]
Ventoroli 1999 {published data only}
- Venturoli S, Marescalchi O, Colombo FM, Marcelli S, Ravaioli B, Bagnoli A, et al. A prospective randomised trial comparing low dose flutamide, finasteride, ketoconazole and cyproterone acetate‐estrogen regimens in the treatment of hirustism. Journal of Clinical Endocrinology and Metabolism 1999;84(4):1304‐10. [DOI] [PubMed] [Google Scholar]
Vermeulen 1988 {published data only}
- Vermeulen A, Rubens R. Effects of cyproterone acetate plus ethinylestradiol low dose on plasma androgens and lipids in mildly hirsute or acneic young women. Contraception 1988;38(4):419‐28. [DOI] [PubMed] [Google Scholar]
Vexiau 1995 {published data only}
- Vexiau P, Fiet J, Conard J, Abramovici Y, Boudou P, Hardy N, et al. 17 beta estradiol: oral or parenteral administration in hyperandrogenic women? Metabolic tolerance in association with cyproterone acetate. Fertility and Sterility 1995;63(3):508‐15. [DOI] [PubMed] [Google Scholar]
Young 1998 {published data only}
- Young R, Sinclair R. Hirsutes II: treatment. Australian Journal of Dermatology 1998;39(3):151‐7. [DOI] [PubMed] [Google Scholar]
Additional references
Adams 1986
- Adams J, Polson DW, Franks S. Prevalence of polycystic ovaries in women with anovulation and idiopathic hirsutism. British Medical Journal Clinical Research Edition 1986;293(6543):355‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Appelt 1984
- Appelt H, Strauss B. Effects of anti‐androgen treatment on the sexuality of women with hyperandrogenism. Psychotherapy and psychosomatics 1984;42(1‐4):177‐81. [DOI] [PubMed] [Google Scholar]
Ashton 1987
- Ashton RE, Miller JA, Wojnarowska FT, et al. Antiandrogen treatment in women with acne: a controlled trial. In: Schindler AE editor(s). Antiandrogen‐estrogen therapy for signs of androgenisation. Berlin: Walter de Gruyter, 1987:117‐38. [Google Scholar]
Bunker 1989
- Bunker CB, Newton JA, Kilborn J, Patel A, Conway GS, Jacobs HS. Most women with acne have polycystic ovaries. British Journal of Dermatology 1989;121(6):675‐80. [DOI] [PubMed] [Google Scholar]
Conway 1989
- Conway GS, Honour JW, Jacobs HS. Heterogeneity of the polycystic ovary syndrome: clinical, endocrine and ultrasound features in 556 patients. Clinical Endocrinology 1989;30(4):459‐70. [DOI] [PubMed] [Google Scholar]
Ferriman 1961
- Ferriman D, Gallwey JD. Clinical assessment of body hair growth in women. Journal of Clinical Endocrinology and Metabolism 1961;21:1440‐7. [DOI] [PubMed] [Google Scholar]
Flamigni 1971
- Flamigni C, Collins WP, Koullapis, Craft I, Dewhurst CJ, Sommerville IF. Androgen metabolism in human skin. Journal of Clinical Endocrinology and Metabolism 1971;32(6):737‐43. [DOI] [PubMed] [Google Scholar]
Franks 1989
- Franks S. Polycystic ovary syndrome: a changing perspective. Clinical Endocrinology 1989;31(1):87‐120. [DOI] [PubMed] [Google Scholar]
Hammerstein 1975
- Hammerstein J, Meckies J, Leo‐Rossberg I, Moltz L, Zielske F. Use of cyproterone acetate (CPA) in the treatment of acne, hirsutism and virilism. Journal of Steroid Biochemistry 1975;6(6):827‐36. [DOI] [PubMed] [Google Scholar]
Hammerstein 1983
- Hammerstein J, Moltz L, Schwartz U. Antiandrogens in the treatment of acne and hirsutism. Journal of Steroid Biochemistry 1983;19(1B):591‐7. [DOI] [PubMed] [Google Scholar]
Jones 1981
- Jones KR, Katz M, Keyzer C, Gordon W. Effect of cyproterone acetate on rate of hair growth in hirsute women. British Journal of Dermatology 1981;105(6):685‐92. [DOI] [PubMed] [Google Scholar]
Kuttenn 1980
- Kuttenn F, Rigaud C, Wright F, Mauvais‐Jarvis P. Treatment of hirsutism by oral cyproterone acetate and percutaneous estradiol. Journal of Clinical Endocrinology and Metabolism 1980;51(5):1107‐11. [DOI] [PubMed] [Google Scholar]
Lunnell 1982
- Lunnell NO, Zador G, Carlstrom K, Eneroth P, Patek E, Wagner J. The effect of cyproterone acetate on pituitary‐ovarian function and clinical symptoms in hirsute women. Acta Endocrinology 1982;100:91‐7. [DOI] [PubMed] [Google Scholar]
McKnight 1984
- McKnight E. The prevalence of "hirsutism" in young women. Psychotherapy and Psychosomatics 1964;42:177‐81. [Google Scholar]
Mowszowicz 1981
- Mowszowicz I, Riahi M, Wright F, Bouchard F, Kuttenn F, Mauvais‐Jarvis P. Androgen receptor in human skin cytosol. Journal of Clinical Endocrinology and Metabolism 1981;52(2):338‐41. [DOI] [PubMed] [Google Scholar]
Mowszowicz 1983
- Mowszowicz I, Melanitou E, Kirchhoffer MO, Mauvais‐Jarvis P. Dihydrotestosterone stimulates 5‐alpha reductase activity in pubic skin fibroblasts. Journal of Clinical Endocrinology and Metabolism 1983;56(2):320‐5. [DOI] [PubMed] [Google Scholar]
Neumann 1987
- Neumann F. Pharmacological aspects of cyproterone acetate. In: Schindler editor(s). Anti‐androgen estrogen therapy for signs of androgenisation. Berlin: Walter de Gruyter, 1987:23‐40. [Google Scholar]
Nurnberger 1987
- Nurnberger F. Comparison of Diane 35 with Neo‐Eunomin from the dermatological viewpoint. In: Schindler AE editor(s). Anti‐androgen estrogen therapy for signs of androgenisation. Berlin: Walter de Gruyter, 1987:197‐206. [Google Scholar]
Reed 1988
- Reed MJ, Franks S. Anti‐androgens in gynaecological practice. Baillieres Clinical Obstetrics & Gynaecology 1988;2(3):581‐95. [DOI] [PubMed] [Google Scholar]
Rubens1984
- Rubens R. Androgen levels during cyproterone acetate in ethinyl estradiol treatment of hirsutism. Clinical Endocrinology 1984;20(3):313‐25. [DOI] [PubMed] [Google Scholar]
Saitoh 1970
- Saitoh M, Uzuka M, Sakamoto M. Human hair cycle. Journal of Dermatology Investigation 1970;54:65‐81. [DOI] [PubMed] [Google Scholar]
Seago 1985
- Seago SV, Ebling FJ. The hair cycle on the human thigh and upper arm. British Journal of Dermatology 1985;113(1):9‐16. [DOI] [PubMed] [Google Scholar]
van der spuy 1992
- Spuy ZM. Management of hyperandrogenism. Contemporary Reviews in Obstetrics and Gynaecology 1992;4(2):90‐101. [Google Scholar]